Вам также может понравиться
- Why OptometryДокумент30 страницWhy OptometrysandiОценок пока нет
- Group1 - Section A - Aravind Eye CareДокумент6 страницGroup1 - Section A - Aravind Eye CareGopichand AthukuriОценок пока нет
- Equip Second ManualДокумент76 страницEquip Second ManualArjun SutharОценок пока нет
- Group 4 - Double VisionДокумент30 страницGroup 4 - Double VisionMdJahanОценок пока нет
- LCIF Comprehensive Eye CareДокумент3 страницыLCIF Comprehensive Eye CareBassam Al-HimiariОценок пока нет
- 48 Vision 2020Документ20 страниц48 Vision 2020Ngurah DwiОценок пока нет
- Technology Guidelines For A District Eye Care Programme: July 2006Документ53 страницыTechnology Guidelines For A District Eye Care Programme: July 2006Peter AbikoyeОценок пока нет
- Report of Vision 2020 IAPB Workshop IndonesiaДокумент12 страницReport of Vision 2020 IAPB Workshop IndonesiaAstidya Miranti100% (1)
- Project Arvind EyeДокумент7 страницProject Arvind EyeSahil SahniОценок пока нет
- Providing Total Eye CareДокумент23 страницыProviding Total Eye CareHarvey0% (1)
- Community OphthalmologyДокумент33 страницыCommunity OphthalmologyVarun BoddulaОценок пока нет
- 2005 PROF 018 OphthalmicPrimaryCare2005Документ7 страниц2005 PROF 018 OphthalmicPrimaryCare2005Annisa KhairunnisaОценок пока нет
- Aravind Eye Care Group 12 EPGCMM 13Документ4 страницыAravind Eye Care Group 12 EPGCMM 13NIVAS PANDIAN GUNASEKHARANОценок пока нет
- 09 Setting Up A Low Vision ProgrammeДокумент16 страниц09 Setting Up A Low Vision ProgrammeAna ŞonteaОценок пока нет
- Vasan Eye CareДокумент13 страницVasan Eye CareGokul BalajiОценок пока нет
- Deliveryof Eye Care in Developing CountriesДокумент46 страницDeliveryof Eye Care in Developing CountriesStan PletcherОценок пока нет
- Role of Ophthalmic Nurses in Prevention of Ophthalmic DiseasesДокумент4 страницыRole of Ophthalmic Nurses in Prevention of Ophthalmic DiseaseskaskwawОценок пока нет
- GUIDEBOOK To Clinical Optometry Internship 2016Документ77 страницGUIDEBOOK To Clinical Optometry Internship 2016Marjune Dimayuga100% (3)
- Case 2 Solving The Blind SpotДокумент16 страницCase 2 Solving The Blind SpotHans Markson TanОценок пока нет
- Eye Banking BookДокумент135 страницEye Banking BooknetrachikitsakОценок пока нет
- Aravind Eye HospitalДокумент6 страницAravind Eye HospitalMohit GuptaОценок пока нет
- MS Case 19Документ9 страницMS Case 19acb562Оценок пока нет
- EAOO Abstracts Dublin 22Документ40 страницEAOO Abstracts Dublin 22Cristina ÁlvarezОценок пока нет
- Public Health OphthalmologyДокумент52 страницыPublic Health OphthalmologyunonounoОценок пока нет
- Arvind Eye Hospital - Rural MarketingДокумент38 страницArvind Eye Hospital - Rural Marketingsumeetdas09Оценок пока нет
- C11 P08 NPCBДокумент20 страницC11 P08 NPCBChandana KrishnaОценок пока нет
- ManДокумент6 страницManNeko NekoОценок пока нет
- Dr. Pooja Kharbanda PPT 64th DOS Annual Conference, Appreciation Award PaperДокумент36 страницDr. Pooja Kharbanda PPT 64th DOS Annual Conference, Appreciation Award PaperdrpoojakharbandaОценок пока нет
- Aravind Eye Care SystemДокумент4 страницыAravind Eye Care SystemMohammed Hammad RizviОценок пока нет
- Eye Care ReportДокумент20 страницEye Care ReportJoeven HilarioОценок пока нет
- Shti214 0139Документ7 страницShti214 0139Camilo Diaz CerveraОценок пока нет
- GVT Training Brochure 30.09.23Документ8 страницGVT Training Brochure 30.09.23abhiОценок пока нет
- Blindness Control ProgrammeДокумент6 страницBlindness Control Programmearunjv1234Оценок пока нет
- Aravind Eye Care SystemДокумент15 страницAravind Eye Care SystemSamarth Anand100% (1)
- Blindness, Children With Special NeedДокумент23 страницыBlindness, Children With Special NeedRajesh SoniОценок пока нет
- Process Evaluation of A National Primary Eye Care Programme in RwandaДокумент12 страницProcess Evaluation of A National Primary Eye Care Programme in RwandaEvan McCartneyОценок пока нет
- Ceh 42Документ16 страницCeh 42Rashmi ChabraОценок пока нет
- Market Research Report Eye SurgeonДокумент14 страницMarket Research Report Eye SurgeonNasty GamingОценок пока нет
- Web MaterialДокумент5 страницWeb MaterialChitranjan KumarОценок пока нет
- Vision Centre Swali, Bayelsa StateДокумент25 страницVision Centre Swali, Bayelsa StateAF Dowell MirinОценок пока нет
- BlindnessДокумент26 страницBlindnessdrmeenaxiОценок пока нет
- Aravind Eye CareДокумент29 страницAravind Eye CareNiy MdОценок пока нет
- Internship Project Report On Mobile-Health Applications For The Efficient Delivery of Health Care Facility To People: - A Survey On Woodland RPGДокумент42 страницыInternship Project Report On Mobile-Health Applications For The Efficient Delivery of Health Care Facility To People: - A Survey On Woodland RPGBishal RoyОценок пока нет
- Odame GeraldДокумент20 страницOdame Geraldbhad-ass IncОценок пока нет
- Right To Sight: A Management Case Study On Aravind Eye HospitalsДокумент11 страницRight To Sight: A Management Case Study On Aravind Eye HospitalsRushit GnanaroyОценок пока нет
- ProjДокумент23 страницыProjG.D EYE HOSPITALОценок пока нет
- Aravind Eye Hospital Case StudyДокумент14 страницAravind Eye Hospital Case StudySahana GowdaОценок пока нет
- Health Systems: Aurthor (S)Документ6 страницHealth Systems: Aurthor (S)Sucheta MitraОценок пока нет
- Primary Eye Care, Community Ophthalmology and General Ophthalmology Author RCOphth - Welcome To The Royal College of OphthalmologistsДокумент17 страницPrimary Eye Care, Community Ophthalmology and General Ophthalmology Author RCOphth - Welcome To The Royal College of Ophthalmologistsshahil agazОценок пока нет
- Priyanshu - Sarkar - Project Report On Internship ProgramДокумент25 страницPriyanshu - Sarkar - Project Report On Internship ProgramLog InОценок пока нет
- Vedic Astrology InterpretationДокумент6 страницVedic Astrology InterpretationTirapath ChobchuenОценок пока нет
- 2 Fast 2 InfectiousДокумент16 страниц2 Fast 2 InfectiousManila Doctors Hospital OphthalmologyОценок пока нет
- Barriers To Use of Refractive Services in Mozambique: Original ArticleДокумент11 страницBarriers To Use of Refractive Services in Mozambique: Original ArticleAnifo Jose AntonioОценок пока нет
- Sandeep Dissertation IihmrДокумент33 страницыSandeep Dissertation IihmrAashu PrabhakarОценок пока нет
- Phacoemulsification Versus Small Incision Cataract Surgery For Treatment ofДокумент7 страницPhacoemulsification Versus Small Incision Cataract Surgery For Treatment ofRagni MishraОценок пока нет
- 75% of Global Blindness Cases in Southeast Asia: Tariq MasoodДокумент2 страницы75% of Global Blindness Cases in Southeast Asia: Tariq MasoodHeiddy Ch SumampouwОценок пока нет
- Press Release - Vision Care - World Optometry Week - Eye Screening and Educational ToolkitsДокумент2 страницыPress Release - Vision Care - World Optometry Week - Eye Screening and Educational ToolkitskwahalawaththeОценок пока нет
- Cuspid Volume 2: Clinically Useful Safety Procedures in DentistryОт EverandCuspid Volume 2: Clinically Useful Safety Procedures in DentistryРейтинг: 3 из 5 звезд3/5 (1)
- Lipoma Removal Worth It? Reviews, Cost, Pictures - RealSelfДокумент11 страницLipoma Removal Worth It? Reviews, Cost, Pictures - RealSelfXICMENОценок пока нет
- NASPGHAN Capsule Endoscopy Clinical Report.28Документ10 страницNASPGHAN Capsule Endoscopy Clinical Report.28Carlos CuadrosОценок пока нет
- NHMSFAP Surgical Safety Checklist TemplateДокумент1 страницаNHMSFAP Surgical Safety Checklist TemplatensmanarultfahmyОценок пока нет
- 190 Disc Repositioning Does It Really WorkДокумент23 страницы190 Disc Repositioning Does It Really WorkAngélica Valenzuela AndrighiОценок пока нет
- Un B.ing Sma '18Документ27 страницUn B.ing Sma '18fitrin sidneОценок пока нет
- Ocular Prosthesis PDFДокумент2 страницыOcular Prosthesis PDFBrianОценок пока нет
- Modifiers-Table 122015 2Документ25 страницModifiers-Table 122015 2khatОценок пока нет
- Abbott Letter Transgender YouthДокумент15 страницAbbott Letter Transgender YouthJulie MorenoОценок пока нет
- AAO CatalogДокумент80 страницAAO CatalogLetchumana Krishnan50% (2)
- TCI DiprivanДокумент74 страницыTCI DiprivanVan Basten ArdiansyachОценок пока нет
- 49CДокумент154 страницы49Crudolfpetersson100% (2)
- Uterine FibroidsДокумент25 страницUterine FibroidsMarie Eulie PatinoОценок пока нет
- Clubfoot A Comprehensive Approach Past Present andДокумент36 страницClubfoot A Comprehensive Approach Past Present andSIVA BHARATHIОценок пока нет
- Cerner - PATIENT JOURNEYДокумент18 страницCerner - PATIENT JOURNEYtimОценок пока нет
- Surgical Stent and C-Arm Guided Reduction andДокумент5 страницSurgical Stent and C-Arm Guided Reduction andkityamuwesiОценок пока нет
- Surgical Treatment of Orthopaedic TraumaДокумент2 страницыSurgical Treatment of Orthopaedic TraumabedadidebeliОценок пока нет
- Post-Operative Application of Lidocaine With Epinephrine Effectively Mitigates Pain in Women Who Had Caesarean SectionДокумент7 страницPost-Operative Application of Lidocaine With Epinephrine Effectively Mitigates Pain in Women Who Had Caesarean SectionInternational Journal of Innovative Science and Research Technology100% (1)
- The German Emergency and Disaster Medicine and Management Systemdhistory and PresentДокумент9 страницThe German Emergency and Disaster Medicine and Management Systemdhistory and PresentAhmet DoganОценок пока нет
- Firmin Technique For Microtia ReconstructionДокумент7 страницFirmin Technique For Microtia ReconstructionDimitris Rodriguez100% (1)
- CDC Report: "Antibiotic Resistance Threats in The United States"Документ148 страницCDC Report: "Antibiotic Resistance Threats in The United States"Patrick CrozierОценок пока нет
- Surgical Wound ClassificationДокумент1 страницаSurgical Wound Classificationgeclear323Оценок пока нет
- Pyogenic Liver AbscessДокумент10 страницPyogenic Liver AbscessFergie Erazo BeltránОценок пока нет
- Nerve Entrapment - UpdateДокумент17 страницNerve Entrapment - UpdatealobrienОценок пока нет
- From Hippo Crates To GalenДокумент26 страницFrom Hippo Crates To GalensalammiОценок пока нет
- Harpur Memorial My BookletДокумент13 страницHarpur Memorial My BookletsjvanstratenОценок пока нет
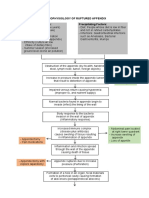
- Pathophysiology of Ruptured AppendixДокумент2 страницыPathophysiology of Ruptured AppendixAya PaquitОценок пока нет
- One Shot RevisionДокумент171 страницаOne Shot RevisionKuldip PatelОценок пока нет
- Orbital Fracture JournalДокумент11 страницOrbital Fracture JournalPramod KumarОценок пока нет
- DapusДокумент3 страницыDapusDanial AhmadОценок пока нет
- CPG Pressure UlcerДокумент104 страницыCPG Pressure Ulcerharfi100% (1)