Вам также может понравиться
- Canine LamenessДокумент442 страницыCanine LamenessClarice Gonring100% (1)
- Zibu SymbolsДокумент4 страницыZibu SymbolsNagarajan86% (7)
- Cytology in Practice Veterinary Medicine PDFДокумент57 страницCytology in Practice Veterinary Medicine PDFCarla Victoria Vejar DíazОценок пока нет
- Basic Avian Bone Growth and HealingДокумент8 страницBasic Avian Bone Growth and HealingIban HernándezОценок пока нет
- Small Animal Spinal Disorders Diagnosis and Surgery, 2nd Edition (Vetbooks - Ir)Документ369 страницSmall Animal Spinal Disorders Diagnosis and Surgery, 2nd Edition (Vetbooks - Ir)ghimboasaОценок пока нет
- Small Animal Abdominal Ultrasonography Liver & GallBladder - Part 2Документ8 страницSmall Animal Abdominal Ultrasonography Liver & GallBladder - Part 2ludiegues752100% (1)
- Corrective Shoeing of Equine DenoixДокумент9 страницCorrective Shoeing of Equine DenoixEduardo JaraОценок пока нет
- Surgery of The Bovine Large IntestineДокумент18 страницSurgery of The Bovine Large IntestineJhon Bustamante CanoОценок пока нет
- Media Analysis For SoundДокумент32 страницыMedia Analysis For SoundJerralynDavisОценок пока нет
- Current Diagnostic Techniques in Veterinary Surgery PDFДокумент2 страницыCurrent Diagnostic Techniques in Veterinary Surgery PDFKirti JamwalОценок пока нет
- Wobblers SyndromeДокумент37 страницWobblers SyndromeSazzle CakeОценок пока нет
- Equine Castration AU Vet JournalДокумент7 страницEquine Castration AU Vet JournalYolandi Lewis StoltzОценок пока нет
- Sutures عبد الرحمن الزميليДокумент54 страницыSutures عبد الرحمن الزميليعبد الرحمن خالد الزميليОценок пока нет
- Radiographic Signs of Pulmonar DiseaseДокумент10 страницRadiographic Signs of Pulmonar DiseaseMarleeng CáceresОценок пока нет
- Amputation of Tail in AnimalsДокумент8 страницAmputation of Tail in AnimalsSabreen khattakОценок пока нет
- ACKD in DogsДокумент9 страницACKD in DogsGreomary Cristina MalaverОценок пока нет
- Accd e BookДокумент154 страницыAccd e BookAchmad Nur MmadОценок пока нет
- Ovariectomia Vs OvariohisterectomiaДокумент5 страницOvariectomia Vs OvariohisterectomiaRicardo CaveroОценок пока нет
- Cattle Uterine ProlapseДокумент3 страницыCattle Uterine ProlapseElena M. TilibaşaОценок пока нет
- Outcomes of Dogs Undergoing Limb Amputation, Owner Satisfaction With Limb Amputation Procedures, and Owner Perceptions Regarding Postsurgical Adaptation: 64 Cases (2005-2012)Документ7 страницOutcomes of Dogs Undergoing Limb Amputation, Owner Satisfaction With Limb Amputation Procedures, and Owner Perceptions Regarding Postsurgical Adaptation: 64 Cases (2005-2012)William ChandlerОценок пока нет
- Harvard Tools For Small Animal SurgeryДокумент7 страницHarvard Tools For Small Animal SurgeryJoel GoodmanОценок пока нет
- M.C. Muhlbauer, S.K. Kneller - Radiography of The Dog and Cat - Guide To Making and Interpreting Radiographs-Wiley-Blackwell (2024)Документ579 страницM.C. Muhlbauer, S.K. Kneller - Radiography of The Dog and Cat - Guide To Making and Interpreting Radiographs-Wiley-Blackwell (2024)dpcamposhОценок пока нет
- CANINE-Fractures of The Proximal Femoral Physis in DogsДокумент11 страницCANINE-Fractures of The Proximal Femoral Physis in Dogstaner_soysurenОценок пока нет
- ANAT.301 3 (1-2) : Veterinary Anatomy - I Theory One Class/ Week 20 Mrks Practical Two Classes/ WeekДокумент34 страницыANAT.301 3 (1-2) : Veterinary Anatomy - I Theory One Class/ Week 20 Mrks Practical Two Classes/ WeekIftikhar hussainОценок пока нет
- Veterinary Gynaecology ObstetricsДокумент8 страницVeterinary Gynaecology ObstetricsSuryakantaRoulTuntunОценок пока нет
- Ecg in DogsДокумент107 страницEcg in DogsPLABITA GOSWAMI100% (2)
- Suspensory Ligament Rupture Tech During Small Animal OH PDFДокумент8 страницSuspensory Ligament Rupture Tech During Small Animal OH PDFRiesky NudialestariОценок пока нет
- Gastrointestinal Surgical Techniques in Small AnimalsДокумент354 страницыGastrointestinal Surgical Techniques in Small AnimalsLuh SmithОценок пока нет
- Lameness - GeneralДокумент34 страницыLameness - GeneralS. Bala DahiyaОценок пока нет
- EXOTİC-Urinary Badder Eversion in Rabbit DoesДокумент5 страницEXOTİC-Urinary Badder Eversion in Rabbit Doestaner_soysurenОценок пока нет
- Hints On Veterinary Ophthalmology: By/Sara Ahmed Hassouna BVSC, MSC Surgery Dept. Vet. Med. Alex. UniДокумент39 страницHints On Veterinary Ophthalmology: By/Sara Ahmed Hassouna BVSC, MSC Surgery Dept. Vet. Med. Alex. UniBibek SutradharОценок пока нет
- Avian Medicine and Surgery in Practice: Bob DoneleyДокумент6 страницAvian Medicine and Surgery in Practice: Bob DoneleyAurey NedhifaОценок пока нет
- Dystocia in Mare: - By: Dr. Dhiren BhoiДокумент50 страницDystocia in Mare: - By: Dr. Dhiren BhoidrdhirenvetОценок пока нет
- Veterinary Forensic ToxicologyДокумент11 страницVeterinary Forensic ToxicologyCarlos Alberto Chaves VelasquezОценок пока нет
- Veterinary Virology at A Glance by Sukdeb Nandi PDFДокумент149 страницVeterinary Virology at A Glance by Sukdeb Nandi PDFPublic InterestОценок пока нет
- FELINE-Clinical Forms of Acquired Myasthenia Gravis in CatsДокумент7 страницFELINE-Clinical Forms of Acquired Myasthenia Gravis in Catstaner_soysurenОценок пока нет
- Surgery B PracticalДокумент12 страницSurgery B PracticalMohamed KhaledОценок пока нет
- Special Veterinary Pathology: The Canadian Veterinary Journal. La Revue Veterinaire Canadienne February 1990Документ2 страницыSpecial Veterinary Pathology: The Canadian Veterinary Journal. La Revue Veterinaire Canadienne February 1990Alonso Guardado100% (1)
- Canine and Feline Endocrinology and ReproductionДокумент1 095 страницCanine and Feline Endocrinology and ReproductionmarparolaОценок пока нет
- Veterinary Anatomy of Domestic Mammals 3rd EditionДокумент646 страницVeterinary Anatomy of Domestic Mammals 3rd Editionmaria da matosОценок пока нет
- BCF Small Animal Exposure Charts Digital Radiography DR 100cm Distance 0412Документ3 страницыBCF Small Animal Exposure Charts Digital Radiography DR 100cm Distance 0412Denise Gomes de MeloОценок пока нет
- Farm Animal Ultrasonography1PDFДокумент315 страницFarm Animal Ultrasonography1PDFMaria Elaine SumoОценок пока нет
- Canine Ehrlichiosis With Uveitis in A Pug Breed Dog: Case StudДокумент2 страницыCanine Ehrlichiosis With Uveitis in A Pug Breed Dog: Case StudDR HAMESH RATREОценок пока нет
- Veterinary Physiology Course Structure - at A GlanceДокумент13 страницVeterinary Physiology Course Structure - at A Glancemohit jainОценок пока нет
- Tumor Pathology AtlasДокумент1 353 страницыTumor Pathology AtlaskaterenchukigorОценок пока нет
- Equine Protozoal MyeloencephalitisДокумент4 страницыEquine Protozoal Myeloencephalitisfreak009Оценок пока нет
- Horse Feeding PDFДокумент28 страницHorse Feeding PDFGigiPetreaОценок пока нет
- Birds and Exotics - MCannon PDFДокумент42 страницыBirds and Exotics - MCannon PDFAl OyОценок пока нет
- Factsheet - Livestock - ReproductiveDiseases in Cattle v2Документ3 страницыFactsheet - Livestock - ReproductiveDiseases in Cattle v2lenn chandОценок пока нет
- Canine InsulinomaДокумент5 страницCanine Insulinomasoff4ikaОценок пока нет
- Equine Gastric Ulcers / A Presentation by Wendy Harless Mollat, DVM, DACVIM, Pilchuck Veterinary HospitalДокумент47 страницEquine Gastric Ulcers / A Presentation by Wendy Harless Mollat, DVM, DACVIM, Pilchuck Veterinary HospitalPilchuck Veterinary HospitalОценок пока нет
- Canine Radiographs: Click Skeleton To EnterДокумент456 страницCanine Radiographs: Click Skeleton To EnterAndres Luna Mendez100% (2)
- Female Rat Reproductive Cycle PDFДокумент10 страницFemale Rat Reproductive Cycle PDFogheeluvОценок пока нет
- Complete Ophtho VM555 CoursepackДокумент189 страницComplete Ophtho VM555 Coursepacknandhus2227Оценок пока нет
- Links For Video Lectures at YouTube On Veterinary Obstetrics by Prof G.N.PurohitДокумент1 страницаLinks For Video Lectures at YouTube On Veterinary Obstetrics by Prof G.N.PurohitgnpobsОценок пока нет
- Presentation OsteotomyДокумент20 страницPresentation OsteotomyArijit ChowdhuryОценок пока нет
- Topic Top Dewormers and Rearing Models in Pakistan 1 - Ten Dewormers With Their PropertiesДокумент4 страницыTopic Top Dewormers and Rearing Models in Pakistan 1 - Ten Dewormers With Their PropertiesjghhjОценок пока нет
- Clinical Examination of The Abdomen in Adult CattleДокумент15 страницClinical Examination of The Abdomen in Adult CattleStefanySalasОценок пока нет
- (Mónica V. Cunha, João Inácio) Veterinary Infec PDFДокумент557 страниц(Mónica V. Cunha, João Inácio) Veterinary Infec PDFNa KhanОценок пока нет
- Animal Birth ControlДокумент15 страницAnimal Birth Controlvenku07484435Оценок пока нет
- Small Animal Abdominal Ultrasonography - The SpleenДокумент9 страницSmall Animal Abdominal Ultrasonography - The Spleenludiegues752Оценок пока нет
- US Artifacts - University of ChicagoДокумент101 страницаUS Artifacts - University of Chicagoludiegues752Оценок пока нет
- Top 5 Causes of Splenomegaly in Dogs - Clinicians BriefДокумент5 страницTop 5 Causes of Splenomegaly in Dogs - Clinicians Briefludiegues752Оценок пока нет
- Formulation of A Standardized Protocol and Determination of The Size and Appearance of The Spleen in Healthy CatsДокумент8 страницFormulation of A Standardized Protocol and Determination of The Size and Appearance of The Spleen in Healthy Catsludiegues752Оценок пока нет
- (2004) Ultrasonographic Evaluation of Abdominal Organs in Veterinary MedicineДокумент3 страницы(2004) Ultrasonographic Evaluation of Abdominal Organs in Veterinary Medicineludiegues752Оценок пока нет
- Radiology Packet 7 Congenital Cardiac DiseaseДокумент27 страницRadiology Packet 7 Congenital Cardiac Diseaseludiegues752Оценок пока нет
- (2012) Investigation and Management of Splenic Disease in DogsДокумент8 страниц(2012) Investigation and Management of Splenic Disease in Dogsludiegues752Оценок пока нет
- Imaging Intestinal ObstructionДокумент5 страницImaging Intestinal Obstructionludiegues752Оценок пока нет
- Radiology Packet 3 Normal Vs Enlarged HeartДокумент11 страницRadiology Packet 3 Normal Vs Enlarged Heartludiegues752Оценок пока нет
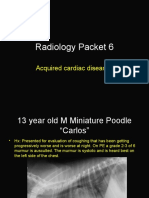
- Radiology Packet 6 Acquired Cardiac DiseasesДокумент25 страницRadiology Packet 6 Acquired Cardiac Diseasesludiegues752Оценок пока нет
- Radiology Packet 5 Heart FailureДокумент25 страницRadiology Packet 5 Heart Failureludiegues752Оценок пока нет
- Radiology Packet 4 Cardiac EnlargementДокумент28 страницRadiology Packet 4 Cardiac Enlargementludiegues752Оценок пока нет
- (2004) Ultrasonographic Evaluation of Abdominal Organs in Veterinary MedicineДокумент3 страницы(2004) Ultrasonographic Evaluation of Abdominal Organs in Veterinary Medicineludiegues752Оценок пока нет
- (2012) Investigation and Management of Splenic Disease in DogsДокумент8 страниц(2012) Investigation and Management of Splenic Disease in Dogsludiegues752Оценок пока нет
- (2016) Retrospective Study of Adrenal Gland US in Dogs With Normal and Abnormal ACTH Stimulation Test - Eric Lindquist PDFДокумент6 страниц(2016) Retrospective Study of Adrenal Gland US in Dogs With Normal and Abnormal ACTH Stimulation Test - Eric Lindquist PDFludiegues752Оценок пока нет
- (2016) Prevalence of Adrenal Gland Masses As Incidental Findings During Abdominal Computed Tomography in DogsДокумент5 страниц(2016) Prevalence of Adrenal Gland Masses As Incidental Findings During Abdominal Computed Tomography in Dogsludiegues752Оценок пока нет
- (2016) Ultrasonographic Features of Adrenal Gland Lesions in Dogs Can Aid in DiagnosisДокумент9 страниц(2016) Ultrasonographic Features of Adrenal Gland Lesions in Dogs Can Aid in Diagnosisludiegues752Оценок пока нет
- (2016) Associations Between Sex, Body Weight, Age, and US Determined Adrenal Thickness in Dogs With Non-Adrenal Gland IllnessДокумент9 страниц(2016) Associations Between Sex, Body Weight, Age, and US Determined Adrenal Thickness in Dogs With Non-Adrenal Gland Illnessludiegues752Оценок пока нет
- Ultrasonographic Evaluation of Adrenal Gland Size Compared To Body Weight in Normal DogsДокумент10 страницUltrasonographic Evaluation of Adrenal Gland Size Compared To Body Weight in Normal Dogsludiegues752Оценок пока нет
- (2017) Repetitive Ultrasonographic Assessment of Adrenal Size and Shape Changes - A Clue For An Asymptomatic Sex Hormone-Secreting AdenomaДокумент5 страниц(2017) Repetitive Ultrasonographic Assessment of Adrenal Size and Shape Changes - A Clue For An Asymptomatic Sex Hormone-Secreting Adenomaludiegues752Оценок пока нет
- The IntegumentДокумент15 страницThe Integumentludiegues752Оценок пока нет
- (2010) Ultrasonographic Evaluation of Adrenal Glands in Dogs With Primary Hypoadrenocorticism or Mimicking DiseasesДокумент5 страниц(2010) Ultrasonographic Evaluation of Adrenal Glands in Dogs With Primary Hypoadrenocorticism or Mimicking Diseasesludiegues752Оценок пока нет
- Case Report: Rapport de CasДокумент4 страницыCase Report: Rapport de Casludiegues752Оценок пока нет
- Alterations in The SkinДокумент9 страницAlterations in The Skinludiegues752Оценок пока нет
- (2012) Emerging Skin Conditions in CattleДокумент9 страниц(2012) Emerging Skin Conditions in Cattleludiegues752Оценок пока нет
- (1997) Ultrasonographic Adrenal Gland Measurements in Dogs Without Evidence of Adrenal DiseaseДокумент7 страниц(1997) Ultrasonographic Adrenal Gland Measurements in Dogs Without Evidence of Adrenal Diseaseludiegues752Оценок пока нет
- Derm History FormДокумент1 страницаDerm History Formludiegues752Оценок пока нет
- (2015) Basics of Equine DermatologyДокумент10 страниц(2015) Basics of Equine Dermatologyludiegues752Оценок пока нет
- Spleen Evaluation Using Contrast Enhanced Ultrasonography and Doppler in Dogs With Subclinical EhrlichiosisДокумент5 страницSpleen Evaluation Using Contrast Enhanced Ultrasonography and Doppler in Dogs With Subclinical Ehrlichiosisludiegues752Оценок пока нет
- Chest MobilityДокумент25 страницChest Mobilitywahyuni pelita sariОценок пока нет
- ANAPHY Respiratory SystemДокумент30 страницANAPHY Respiratory SystemAshley Franceska CansanayОценок пока нет
- Respiratory System - AnatomyДокумент28 страницRespiratory System - AnatomyDinesh KumarОценок пока нет
- PEDIДокумент280 страницPEDIMiraf MesfinОценок пока нет
- Surgery Viva QuestionsДокумент16 страницSurgery Viva QuestionsChris Lam Cui ShanОценок пока нет
- PREP E-Med 2017Документ93 страницыPREP E-Med 2017Imran A. Isaac100% (1)
- Journal of Chinese Medicine Number 42 May 1993Документ7 страницJournal of Chinese Medicine Number 42 May 1993FERTIL CONEXIONОценок пока нет
- Pediatric RadiographyДокумент10 страницPediatric RadiographyRachelle Danya Dela RosaОценок пока нет
- MasonДокумент208 страницMasongdvfwqeguewguqfgОценок пока нет
- Blunt Chest TraumaДокумент105 страницBlunt Chest TraumasunliesОценок пока нет
- Nursing Care PlanДокумент22 страницыNursing Care PlanjamОценок пока нет
- IdentifyДокумент40 страницIdentifyLeonard Kenshin LianzaОценок пока нет
- Medical Ready Reckoner For BhavasДокумент2 страницыMedical Ready Reckoner For Bhavascoolnidhi134558Оценок пока нет
- Drawing ChildrenДокумент94 страницыDrawing Childrenaleah100% (2)
- William Boericke - Pocket Manual of Homeopathic Materia MedicaДокумент702 страницыWilliam Boericke - Pocket Manual of Homeopathic Materia Medicaadityaupasani100% (4)
- Chest Physiotherapy BPTДокумент20 страницChest Physiotherapy BPTWraith GAMINGОценок пока нет
- Nursing Care PlanДокумент14 страницNursing Care PlanVin Landicho100% (1)
- Check List of Chest PhysiotherapyДокумент3 страницыCheck List of Chest PhysiotherapySuyesh ShresthaОценок пока нет
- Intra Abdominal HypertensionДокумент22 страницыIntra Abdominal HypertensionFernando MorenoОценок пока нет
- Respi-Nclex QuestionsДокумент160 страницRespi-Nclex QuestionsSophia Rose Delos Santos100% (3)
- Acute Disorders by Kiran PhalkeДокумент63 страницыAcute Disorders by Kiran PhalkeKiran PhalkeОценок пока нет
- 21 Marathon Materia Medica Ebook by Dr. Amit Gohel & Team ShaДокумент707 страниц21 Marathon Materia Medica Ebook by Dr. Amit Gohel & Team ShaSaiujwal PasupuletiОценок пока нет
- Script MiloДокумент3 страницыScript Miloapi-449138717Оценок пока нет
- Chest TraumaДокумент28 страницChest TraumaGitaAmeliaTurnipОценок пока нет
- GarlicДокумент7 страницGarlicMaharshi ShrimaliОценок пока нет
- History TakingДокумент15 страницHistory TakingacildevilОценок пока нет
- G.R. No. L-44096Документ8 страницG.R. No. L-44096Nor-Alissa M DisoОценок пока нет
- Trauma ATACC Manual 2014 PDFДокумент460 страницTrauma ATACC Manual 2014 PDFBenjamin Ng100% (1)
- Tips and Tools To Vocal FreedomДокумент10 страницTips and Tools To Vocal FreedomasifОценок пока нет