Вам также может понравиться
- Fentanyl Preloading For Rapid-Sequence Induction AnesthesiaДокумент5 страницFentanyl Preloading For Rapid-Sequence Induction AnesthesiaAngga Munawar MahbubОценок пока нет
- Patients' Perspective On Carpal TunnelДокумент7 страницPatients' Perspective On Carpal Tunnelumer LoneОценок пока нет
- Managing Post-Surgical Pain from a Surgical Point of ViewДокумент55 страницManaging Post-Surgical Pain from a Surgical Point of ViewCox AbeeОценок пока нет
- Klinis MRIДокумент7 страницKlinis MRIraniakusmantoОценок пока нет
- Myofascial Genesis of PainДокумент11 страницMyofascial Genesis of PainMarita PalacoОценок пока нет
- NCP 1Документ1 страницаNCP 1Void LessОценок пока нет
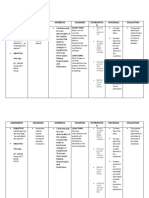
- Assessment Diagnosis Inference Planning Interventio N Rationale EvaluationДокумент9 страницAssessment Diagnosis Inference Planning Interventio N Rationale Evaluationjosh100% (1)
- Effects of Electrical Nerve Stimulation on Ischemic TissueДокумент6 страницEffects of Electrical Nerve Stimulation on Ischemic Tissuedora mantulОценок пока нет
- Subjective Cues: Independent: On The: "Nahihirapa N Ako Huminga" AsДокумент5 страницSubjective Cues: Independent: On The: "Nahihirapa N Ako Huminga" AsYessaminОценок пока нет
- Anesthetic Ointment Only Instead of Injectable Local Lidocaine in Trans-Radial Catheterization A Viable No-Needle AlternativeДокумент5 страницAnesthetic Ointment Only Instead of Injectable Local Lidocaine in Trans-Radial Catheterization A Viable No-Needle AlternativealvОценок пока нет
- General Santos Doctors' Medical School Foundation NCM: 122N Rle ExposureДокумент8 страницGeneral Santos Doctors' Medical School Foundation NCM: 122N Rle Exposurejay kusainОценок пока нет
- Tes 3Документ4 страницыTes 3wiwiОценок пока нет
- Physical Agents & Electrotherapy (Opt 2203) : Tens Physical Agents & ElectrotherapyДокумент2 страницыPhysical Agents & Electrotherapy (Opt 2203) : Tens Physical Agents & ElectrotherapyBrent SantosОценок пока нет
- viX1wMry Poenaru y ColsДокумент5 страницviX1wMry Poenaru y ColsDanii Rocha ParraОценок пока нет
- Jha Sheth 2023 2023 Neurocritical Care Updates in Cerebrovascular DiseaseДокумент5 страницJha Sheth 2023 2023 Neurocritical Care Updates in Cerebrovascular DiseaseProdi Bedah SarafОценок пока нет
- Drug Study on Anesthetics: Effects, Indications and Nursing ResponsibilitiesДокумент9 страницDrug Study on Anesthetics: Effects, Indications and Nursing ResponsibilitiesKalvinArtRazalanCelebradosОценок пока нет
- Endocardial Infarct Scar Recognition by MyocardialДокумент8 страницEndocardial Infarct Scar Recognition by MyocardialMihai-Marian RuseiОценок пока нет
- Estimation of At-Risk and Salvaged Myocardium at Myocardial Perfusion SPECT 1 Month After InfarctionДокумент8 страницEstimation of At-Risk and Salvaged Myocardium at Myocardial Perfusion SPECT 1 Month After InfarctiondrewantaОценок пока нет
- The Austrian Flag - Severe Carpal Tunnel Syndrome: A Case ReportДокумент3 страницыThe Austrian Flag - Severe Carpal Tunnel Syndrome: A Case ReportRansidelenta Vistaprila ElmardaОценок пока нет
- Caso ClínicoДокумент7 страницCaso ClínicoGildson RangelОценок пока нет
- Kinds of Anesthesia SurgeryДокумент12 страницKinds of Anesthesia SurgeryRocio SandersОценок пока нет
- Lignocaine Hydrochloride: Concord Repatriation General HospitalДокумент3 страницыLignocaine Hydrochloride: Concord Repatriation General HospitalLingga AlgifariОценок пока нет
- Effects of Intravenous Dexmedetomidine On Hyperbaric Bupivacaine Spinal Anesthesia: A Randomized StudyДокумент8 страницEffects of Intravenous Dexmedetomidine On Hyperbaric Bupivacaine Spinal Anesthesia: A Randomized StudyMOHAMMED IQBALОценок пока нет
- Intensive Care Ultrasound. Fluid Responsiveness and Shock Assessment - Annals of ATS 2014Документ8 страницIntensive Care Ultrasound. Fluid Responsiveness and Shock Assessment - Annals of ATS 2014Ellys Macías PeraltaОценок пока нет
- RadiologiaДокумент11 страницRadiologiaFernando TeixeiraОценок пока нет
- PDF Hosted at The Radboud Repository of The Radboud University NijmegenДокумент5 страницPDF Hosted at The Radboud Repository of The Radboud University NijmegenGazal KhanОценок пока нет
- Anesthesia For Endovascular NeurosurgeryДокумент11 страницAnesthesia For Endovascular NeurosurgeryMorteza Mazloom Farsi BafОценок пока нет
- Burn Ctu 312 - 2Документ1 страницаBurn Ctu 312 - 2Shaira Ann CalambaОценок пока нет
- Intradural Spinal Cord Tumors: UpplementДокумент1 страницаIntradural Spinal Cord Tumors: Upplementlauzark gashbellОценок пока нет
- Unconscious Pain Patients 2 Dr. RB SukmonoДокумент36 страницUnconscious Pain Patients 2 Dr. RB Sukmonoreagan setiawanОценок пока нет
- An Overview of Pathways Encoding Nociception: S.A. Woller, K.A. Eddinger, M. Corr, T.L. YakshДокумент7 страницAn Overview of Pathways Encoding Nociception: S.A. Woller, K.A. Eddinger, M. Corr, T.L. YakshRory Denny SaputraОценок пока нет
- Paper 65Документ1 страницаPaper 65abdul hamidОценок пока нет
- (19330693 - Journal of Neurosurgery) Assessment of Outcomes in Consecutive Patients Undergoing Dorsal Scapular Nerve DecompressionДокумент8 страниц(19330693 - Journal of Neurosurgery) Assessment of Outcomes in Consecutive Patients Undergoing Dorsal Scapular Nerve DecompressionGeorgios StathisОценок пока нет
- 2015 Eccentric or Concentric Exercises For The Treatment of Tendinopathies...Документ11 страниц2015 Eccentric or Concentric Exercises For The Treatment of Tendinopathies...Castro WeithОценок пока нет
- Cadence WhitepaperДокумент8 страницCadence Whitepaperbashir019Оценок пока нет
- JDattaMegheInstMedSciUniv162235-4959576 134635Документ5 страницJDattaMegheInstMedSciUniv162235-4959576 134635shyampanga2Оценок пока нет
- Survival After Surgical Excision OF Single Metastatic Brain TumorsДокумент6 страницSurvival After Surgical Excision OF Single Metastatic Brain Tumorsfira rifaОценок пока нет
- Impact of Varying Degrees of Peripheral Nerve BlockadeДокумент7 страницImpact of Varying Degrees of Peripheral Nerve BlockadeAlejandra SanchezОценок пока нет
- Electrically Elicited Quadriceps Muscle Torque - A Comparison of 3 WaveformsДокумент8 страницElectrically Elicited Quadriceps Muscle Torque - A Comparison of 3 WaveformsMarcoОценок пока нет
- NCP Impaired Physical MobilityДокумент2 страницыNCP Impaired Physical MobilityKristine Young0% (1)
- NCP Rheumatoid ArthritisДокумент3 страницыNCP Rheumatoid ArthritisJanieross Lamboso100% (1)
- Electrically Elicited Muscle Torque - Comparison Between 2500-Hz Burst-Modulated Alternating Current and Monophasic Pulsed CurrentДокумент7 страницElectrically Elicited Muscle Torque - Comparison Between 2500-Hz Burst-Modulated Alternating Current and Monophasic Pulsed CurrentMarcoОценок пока нет
- JPR 143256 Ultrasound Guided Methotrexate Injection For de Quervain Dis 092617Документ4 страницыJPR 143256 Ultrasound Guided Methotrexate Injection For de Quervain Dis 092617Naufal K. YurnadiОценок пока нет
- Forshaw 2000Документ2 страницыForshaw 2000温鴻旺awangОценок пока нет
- Diagnosis of Isodense Subdural Hematomas by Computed TomographyДокумент5 страницDiagnosis of Isodense Subdural Hematomas by Computed TomographyDessy RismayatiОценок пока нет
- NCP Post Op (Impaired and Risk For Infection)Документ4 страницыNCP Post Op (Impaired and Risk For Infection)Carl J.Оценок пока нет
- Myocardial Infarction NCPДокумент3 страницыMyocardial Infarction NCPlapistolero33% (3)
- Bloq InfraДокумент6 страницBloq InfraMaría Alejandra García QОценок пока нет
- Five Operations That Give The Best Results After Brachial Plexus InjuryДокумент12 страницFive Operations That Give The Best Results After Brachial Plexus InjuryResurg ClinicОценок пока нет
- Bezold Jarisch 2Документ11 страницBezold Jarisch 2drcarlos.romero.umichОценок пока нет
- NCP (Impaired Physical Mobility, Acute Pain)Документ8 страницNCP (Impaired Physical Mobility, Acute Pain)joshane2008100% (14)
- Examining The Efficacy of Saunders Cervical Traction Device For Alleviating Neck Pain BHARTI DANGARДокумент4 страницыExamining The Efficacy of Saunders Cervical Traction Device For Alleviating Neck Pain BHARTI DANGARbdangar677Оценок пока нет
- Neurovascular CompressionДокумент9 страницNeurovascular CompressionWorthless BoysОценок пока нет
- Cervicofacial Necrotizing Fasciitis and Drugs: Clinical ReportДокумент2 страницыCervicofacial Necrotizing Fasciitis and Drugs: Clinical ReportSadaf MohtashamiОценок пока нет
- Degenerative Mitral Stenosis: Interpreting The Meaning of Mean GradientДокумент3 страницыDegenerative Mitral Stenosis: Interpreting The Meaning of Mean GradientNasriОценок пока нет
- The Effects of Electroacupuncture at The ST36.31Документ7 страницThe Effects of Electroacupuncture at The ST36.31Arturo DíazОценок пока нет
- Dural Arteriovenous Fistulas: A Review of The Literature and A Presentation of A Single Institution's ExperienceДокумент9 страницDural Arteriovenous Fistulas: A Review of The Literature and A Presentation of A Single Institution's Experiencejan lester LaingoОценок пока нет
- Orthospec: RadialspecДокумент44 страницыOrthospec: Radialspecapi-538691317Оценок пока нет
- Effects of Dexamethasone PDFДокумент9 страницEffects of Dexamethasone PDFAndreea Livia DumitrescuОценок пока нет
- Propagation of Transient Elastic Waves in Stratified Anisotropic MediaОт EverandPropagation of Transient Elastic Waves in Stratified Anisotropic MediaОценок пока нет
- Nihms 727141Документ18 страницNihms 727141Nurul FajriОценок пока нет
- The Oncologist 1996 Packer 381 93Документ13 страницThe Oncologist 1996 Packer 381 93Nurul FajriОценок пока нет
- Seizures After Bleeding Into The Brain: Steven Karceski, MDДокумент3 страницыSeizures After Bleeding Into The Brain: Steven Karceski, MDNurul FajriОценок пока нет
- Nihms 727141Документ18 страницNihms 727141Nurul FajriОценок пока нет
- The Relationship Between Anticoagulant Therapy and Subdural HematomaДокумент5 страницThe Relationship Between Anticoagulant Therapy and Subdural HematomaNurul FajriОценок пока нет
- Best Practice & Research Clinical Endocrinology & MetabolismДокумент9 страницBest Practice & Research Clinical Endocrinology & MetabolismaldiansyahraufОценок пока нет
- UTF-8'en' (Scandinavian Journal of Pain) Reducing Risk of Spinal Haematoma From Spinal and Epidural Pain ProceduresДокумент22 страницыUTF-8'en' (Scandinavian Journal of Pain) Reducing Risk of Spinal Haematoma From Spinal and Epidural Pain ProceduresNurul FajriОценок пока нет
- C R B S: Urrent Eview in Asic CienceДокумент5 страницC R B S: Urrent Eview in Asic CienceNurul FajriОценок пока нет
- Prolonged Post-Spinal ParalysisДокумент3 страницыProlonged Post-Spinal ParalysisNurul FajriОценок пока нет
- Evaluation of Intraventricular Hemorrhage Assessment Methods For Predicting Outcome Following Intracerebral HemorrhageДокумент8 страницEvaluation of Intraventricular Hemorrhage Assessment Methods For Predicting Outcome Following Intracerebral HemorrhageNurul FajriОценок пока нет
- Ticks and Tick-Borne DiseasesДокумент3 страницыTicks and Tick-Borne DiseasesNurul FajriОценок пока нет
- Calvelli 2015Документ5 страницCalvelli 2015Nurul FajriОценок пока нет
- Best Practice & Research Clinical Endocrinology & MetabolismДокумент9 страницBest Practice & Research Clinical Endocrinology & MetabolismaldiansyahraufОценок пока нет
- 5Документ10 страниц5Nurul FajriОценок пока нет
- Ojmn 2017090615420229Документ8 страницOjmn 2017090615420229Nurul FajriОценок пока нет
- Prognostic Factors in Patients With Spinal Metastasis: A Systematic Review and Meta-AnalysisДокумент20 страницPrognostic Factors in Patients With Spinal Metastasis: A Systematic Review and Meta-AnalysisNurul FajriОценок пока нет
- 12 CR Spontaneous ResolutionДокумент2 страницы12 CR Spontaneous ResolutionNurul FajriОценок пока нет
- 1A Restarting AnticoagTx After IntracranialДокумент32 страницы1A Restarting AnticoagTx After IntracranialNurul FajriОценок пока нет
- (10920684 - Neurosurgical Focus) Acute Subdural Hematoma in Patients On Oral Anticoagulant Therapy - Management and OutcomeДокумент12 страниц(10920684 - Neurosurgical Focus) Acute Subdural Hematoma in Patients On Oral Anticoagulant Therapy - Management and OutcomeNurul FajriОценок пока нет
- 603 Full PDFДокумент4 страницы603 Full PDFNurul FajriОценок пока нет
- 12 CR Spontaneous ResolutionДокумент27 страниц12 CR Spontaneous ResolutionNurul FajriОценок пока нет
- Resumption of Antithrombotic Agents in C PDFДокумент28 страницResumption of Antithrombotic Agents in C PDFNurul FajriОценок пока нет
- The Relationship Between Anticoagulant Therapy and Subdural HematomaДокумент5 страницThe Relationship Between Anticoagulant Therapy and Subdural HematomaNurul FajriОценок пока нет
- Resuming Anticoagulation After Hemorrhage: A Practical ApproachДокумент12 страницResuming Anticoagulation After Hemorrhage: A Practical ApproachNurul FajriОценок пока нет
- 1A Restarting AnticoagTx After IntracranialДокумент32 страницы1A Restarting AnticoagTx After IntracranialNurul FajriОценок пока нет
- 12 CR Spontaneous ResolutionДокумент2 страницы12 CR Spontaneous ResolutionNurul FajriОценок пока нет
- 3a4027df0c51fcf4ad31df42139d310fДокумент9 страниц3a4027df0c51fcf4ad31df42139d310fNurul FajriОценок пока нет
- Gullo 2010Документ6 страницGullo 2010Nurul FajriОценок пока нет
- ID Model Regresi Cox Stratified Pada Data KДокумент10 страницID Model Regresi Cox Stratified Pada Data KNurul FajriОценок пока нет
- Health Benefits BrochureДокумент2 страницыHealth Benefits Brochurebhupi8182Оценок пока нет
- WL DeterminationДокумент12 страницWL Determinationdr asiyaОценок пока нет
- 6 Signs Your Body Is Screaming For HealthДокумент44 страницы6 Signs Your Body Is Screaming For HealthBlasterWorm100% (1)
- LEPROSY Visit ReportДокумент7 страницLEPROSY Visit ReportBabita Dhruw100% (1)
- Clinical Management of Binocular Vision .24Документ1 страницаClinical Management of Binocular Vision .24Ikmal ShahromОценок пока нет
- Accumate 2300-¿ ® Ç¿ë Í PDFДокумент39 страницAccumate 2300-¿ ® Ç¿ë Í PDFjhoniОценок пока нет
- Ameriplan-Health Ameriplan BrochureДокумент5 страницAmeriplan-Health Ameriplan Brochureapi-242298828Оценок пока нет
- Virgina SatirДокумент7 страницVirgina Satirali.chaves.jimenezОценок пока нет
- Gestational Trophoblastic DiseaseДокумент37 страницGestational Trophoblastic DiseaseOlisa 'phage' Onyebuchi100% (1)
- Prof DR Mark Fitzgerald What Is A Trauma System and Trauma System ComponentsДокумент36 страницProf DR Mark Fitzgerald What Is A Trauma System and Trauma System ComponentsBrunoОценок пока нет
- Europsko Istraživanje o Kvaliteti Vode Za KupanjeДокумент28 страницEuropsko Istraživanje o Kvaliteti Vode Za KupanjeIndex.hrОценок пока нет
- Carl RogersДокумент31 страницаCarl Rogerskrizziabendiola100% (3)
- Relational PsychotherapyДокумент229 страницRelational Psychotherapykhushi chopra 0050Оценок пока нет
- Asam Traneksamat Untuk KulitДокумент2 страницыAsam Traneksamat Untuk KulitmonitamiftahОценок пока нет
- 2 2 15 923 PDFДокумент4 страницы2 2 15 923 PDFwatidina100% (1)
- (FREE SAMPLE) The Performance Digest - Issue 17 (March 18)Документ45 страниц(FREE SAMPLE) The Performance Digest - Issue 17 (March 18)Giovanni SlackОценок пока нет
- Nature of NursingДокумент2 страницыNature of Nursingjulesubayubay5428100% (2)
- Oral Habits Retained Deciduous Teeth and Supernumeraries Premature LossДокумент4 страницыOral Habits Retained Deciduous Teeth and Supernumeraries Premature LossGem Hanna Callano ParaguaОценок пока нет
- Role of OT in Rett SyndromeДокумент2 страницыRole of OT in Rett SyndromeDanielle Stella N'LucaОценок пока нет
- Day Spa Treatments TariffsДокумент3 страницыDay Spa Treatments TariffsLouvern MoodleyОценок пока нет
- 12 Lead STEMI MimicsДокумент22 страницы12 Lead STEMI MimicscornondaОценок пока нет
- Acute Lung Injury and Pulmonary Edema GuideДокумент11 страницAcute Lung Injury and Pulmonary Edema GuideStevenPaulDaclesОценок пока нет
- CSA Case Scenario Eating DisordersДокумент7 страницCSA Case Scenario Eating DisordersمرتديلامرتديلاОценок пока нет
- PARAPHIMOSISДокумент3 страницыPARAPHIMOSISEmmeline Dycangchon-GarmaОценок пока нет
- 2018 TransCode Mock Test 6-Questions PDFДокумент37 страниц2018 TransCode Mock Test 6-Questions PDFJasliya Ismail100% (7)
- Bosniak ClassificationДокумент19 страницBosniak ClassificationGirish Kumar100% (1)
- EpiCancer EssayДокумент3 страницыEpiCancer EssayAnthony EngelbrechtОценок пока нет
- Resume O4 Lydm Edmonton AutosavedДокумент3 страницыResume O4 Lydm Edmonton Autosavedapi-314849412Оценок пока нет
- Approaches To Counselling: by Amala Mary JohnyДокумент22 страницыApproaches To Counselling: by Amala Mary Johnyammu2805Оценок пока нет
- Gastroenterology: Case Discussion: Pharmacological PerspectiveДокумент21 страницаGastroenterology: Case Discussion: Pharmacological PerspectivePanini PatankarОценок пока нет