Вам также может понравиться
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (400)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5795)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (345)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- Cell Salts RemediesДокумент13 страницCell Salts RemediesBeyond Medicine100% (8)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- Disease and DefenceДокумент5 страницDisease and DefenceNabindra Ruwali100% (1)
- Salix Nigra.: Specific Indications.-Sexual Erethism, Irritability, and PassionДокумент39 страницSalix Nigra.: Specific Indications.-Sexual Erethism, Irritability, and PassionDr Rushen SinghОценок пока нет
- Pathophysiology of Bronchial AsthmaДокумент2 страницыPathophysiology of Bronchial AsthmaFirenze Fil100% (21)
- PathophysiologyДокумент3 страницыPathophysiologyKita kita100% (1)
- Acute SinusitisДокумент7 страницAcute SinusitisNader SmadiОценок пока нет
- Mycology TransДокумент11 страницMycology TransKita kitaОценок пока нет
- Cell SaltДокумент13 страницCell SaltDominic ShewcraftОценок пока нет
- Nursing Care Plan For Acute BronchitisДокумент6 страницNursing Care Plan For Acute BronchitisNur Panca Retnaningsih50% (2)
- Practical Test 5 CesweДокумент49 страницPractical Test 5 CesweNenbon NatividadОценок пока нет
- Essential Element RESEARCHДокумент4 страницыEssential Element RESEARCHKita kita80% (5)
- General Biology 2: Quarter 4: Week 4 - Module 1D PДокумент25 страницGeneral Biology 2: Quarter 4: Week 4 - Module 1D PSyrine Myles Sullivan100% (1)
- Vice and Drug Education and ControlДокумент118 страницVice and Drug Education and Controlcriminologyalliance0% (1)
- Ciclo Nasal RespiratorioДокумент7 страницCiclo Nasal RespiratorioManuel RaGalОценок пока нет
- CPG On OmeДокумент6 страницCPG On OmeKita kitaОценок пока нет
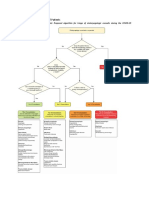
- B. Risk Classifications of ENT Patients: Tier-Based Classification SchemeДокумент2 страницыB. Risk Classifications of ENT Patients: Tier-Based Classification SchemeKita kitaОценок пока нет
- General Data:: S O C R A TДокумент9 страницGeneral Data:: S O C R A TKita kitaОценок пока нет
- Pediatric Ent MalignanciesДокумент69 страницPediatric Ent MalignanciesKita kitaОценок пока нет
- Precursor B and T CellДокумент8 страницPrecursor B and T CellKita kitaОценок пока нет
- Based On Your Possible Final Diagnosis, What Are The Treatment Plans For Our Patient?Документ63 страницыBased On Your Possible Final Diagnosis, What Are The Treatment Plans For Our Patient?Kita kitaОценок пока нет
- BIOETH - Applied EthicsДокумент3 страницыBIOETH - Applied EthicsKita kitaОценок пока нет
- Drugs Affecting The Respiratory SystemДокумент32 страницыDrugs Affecting The Respiratory SystemKita kitaОценок пока нет
- Arterial Blood Gas (Abg)Документ10 страницArterial Blood Gas (Abg)Kita kitaОценок пока нет
- History of Barangay TalebДокумент13 страницHistory of Barangay TalebKita kitaОценок пока нет
- Arthropods of Medical ImportanceДокумент82 страницыArthropods of Medical ImportanceKita kita0% (1)
- Medicine 2021: Specific Health Problems: Genetic DisordersДокумент7 страницMedicine 2021: Specific Health Problems: Genetic DisordersKita kitaОценок пока нет
- 9 Gas Exchange and SmokingДокумент5 страниц9 Gas Exchange and SmokingTala AlkhawajaОценок пока нет
- Bronchiectasis Pa Tho Physiology, Presentation and ManagementДокумент8 страницBronchiectasis Pa Tho Physiology, Presentation and ManagementCristhian MellaОценок пока нет
- Natural ImmunityДокумент34 страницыNatural ImmunitySelvaram SelvaОценок пока нет
- Study of Efficacy of Active Cycle of Breathing TechniquesДокумент89 страницStudy of Efficacy of Active Cycle of Breathing Techniquesnaga9390051055Оценок пока нет
- Cervical MucusДокумент24 страницыCervical MucusRgn McklОценок пока нет
- Case Analysis Group 9 MeaslesДокумент19 страницCase Analysis Group 9 MeaslesJob Arden EstepaОценок пока нет
- Identification of Exudates in Inflammation...Документ5 страницIdentification of Exudates in Inflammation...Ivana Aginta GintingОценок пока нет
- Defense Against Infectious Disease: Skin As A Barrier To InfectionДокумент8 страницDefense Against Infectious Disease: Skin As A Barrier To InfectionFranchesca Rosabel BudimanОценок пока нет
- L and URIДокумент30 страницL and URIlilaОценок пока нет
- YOUR Guide To Chest ClearanceДокумент2 страницыYOUR Guide To Chest ClearanceDr Abdallah BahaaОценок пока нет
- Taffix Scientific Story June 2021Документ41 страницаTaffix Scientific Story June 2021Sanja IlićОценок пока нет
- Eucalyptus Essential OilДокумент4 страницыEucalyptus Essential OilIreneRains0% (1)
- Respiratory System 1Документ186 страницRespiratory System 1Ivann Chan MunarОценок пока нет
- ICU NCP AirwayДокумент3 страницыICU NCP AirwayLisa TandogОценок пока нет
- Asma NEJMДокумент13 страницAsma NEJMAlba RОценок пока нет
- PRO TEENS ResearchДокумент24 страницыPRO TEENS ResearchWee-Weh HamjaОценок пока нет
- Drugs, Discussion On IGCSE Past PaperДокумент9 страницDrugs, Discussion On IGCSE Past PaperinadirahОценок пока нет
- Bio 132 Chapter 23 NotesДокумент8 страницBio 132 Chapter 23 NotesgilissaОценок пока нет
- Drug StudyДокумент2 страницыDrug StudyGel Marie LobatonОценок пока нет