Вам также может понравиться
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5795)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1091)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (345)
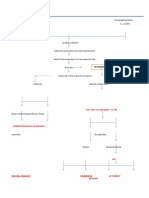
- Energy Pyramid: 0.1% Third-Level Consumers 1% Second-Level ConsumersДокумент2 страницыEnergy Pyramid: 0.1% Third-Level Consumers 1% Second-Level ConsumersAisha BasirОценок пока нет
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- Personal Development Module 8 - Grade 12Документ19 страницPersonal Development Module 8 - Grade 12Sciatzy Faye Tangelon56% (16)
- Savio v. Peterson ComplaintДокумент15 страницSavio v. Peterson ComplaintChicago TribuneОценок пока нет
- Accumulator Operation and ApplicationsДокумент4 страницыAccumulator Operation and ApplicationsChockalingam Athilingam100% (1)
- Music Heals DiseaseДокумент33 страницыMusic Heals DiseasetvmedicineОценок пока нет
- LeadershipДокумент12 страницLeadershipSergi Lee Orate0% (1)
- Cebu Institute of Technology - University College of NursingДокумент2 страницыCebu Institute of Technology - University College of NursingSergi Lee OrateОценок пока нет
- Ôn luyện cấp tốc chứng chỉ Tiếng Anh B1 B2 LH:0907.286.606Документ10 страницÔn luyện cấp tốc chứng chỉ Tiếng Anh B1 B2 LH:0907.286.606Sĩ Phong100% (1)
- NBP HR PlanДокумент38 страницNBP HR Planmuhammad qasim100% (1)
- Sloping Agricultural Land TechnologyДокумент12 страницSloping Agricultural Land TechnologyBe ChahОценок пока нет
- GentamicinДокумент1 страницаGentamicinSergi Lee OrateОценок пока нет
- Reflective Essay PediaДокумент2 страницыReflective Essay PediaSergi Lee OrateОценок пока нет
- CeftazidimeДокумент2 страницыCeftazidimeSergi Lee OrateОценок пока нет
- Reflection Essay On Related Learning Experience: N. Bacalso Avenue, Cebu City 6000, PhilippinesДокумент2 страницыReflection Essay On Related Learning Experience: N. Bacalso Avenue, Cebu City 6000, PhilippinesSergi Lee OrateОценок пока нет
- Plagiarism Checker X Originality: Similarity Found: 19%Документ2 страницыPlagiarism Checker X Originality: Similarity Found: 19%Sergi Lee OrateОценок пока нет
- PCX - Report23Документ2 страницыPCX - Report23Sergi Lee OrateОценок пока нет
- PCX - Report23Документ2 страницыPCX - Report23Sergi Lee OrateОценок пока нет
- Reflection Essay On Nursing Enrichment Course: N. Bacalso Avenue, Cebu City 6000, PhilippinesДокумент2 страницыReflection Essay On Nursing Enrichment Course: N. Bacalso Avenue, Cebu City 6000, PhilippinesSergi Lee OrateОценок пока нет
- Plagiarism Checker X Originality: Similarity Found: 58%Документ1 страницаPlagiarism Checker X Originality: Similarity Found: 58%Sergi Lee OrateОценок пока нет
- OxacillinДокумент1 страницаOxacillinSergi Lee OrateОценок пока нет
- Plagiarism Checker X Originality: Similarity Found: 85%Документ1 страницаPlagiarism Checker X Originality: Similarity Found: 85%Sergi Lee OrateОценок пока нет
- Cebu Institute of Technology - University College of NursingДокумент2 страницыCebu Institute of Technology - University College of NursingSergi Lee OrateОценок пока нет
- Plagiarism Checker X Originality: Similarity Found: 78%Документ1 страницаPlagiarism Checker X Originality: Similarity Found: 78%Sergi Lee OrateОценок пока нет
- Drug StudyДокумент2 страницыDrug StudySergi Lee OrateОценок пока нет
- Neruoncp 1Документ2 страницыNeruoncp 1Sergi Lee OrateОценок пока нет
- B. PathophysiologyДокумент41 страницаB. PathophysiologySergi Lee OrateОценок пока нет
- IntroductionДокумент5 страницIntroductionSergi Lee OrateОценок пока нет
- Cebu Institute of Technology - University College of NursingДокумент2 страницыCebu Institute of Technology - University College of NursingSergi Lee OrateОценок пока нет
- Port Folio Camp Andee AstДокумент28 страницPort Folio Camp Andee AstSergi Lee OrateОценок пока нет
- Path o Physio TB EffusionДокумент2 страницыPath o Physio TB EffusionSergi Lee OrateОценок пока нет
- Notes Pathophysio Serotonin: Basal GangliaДокумент3 страницыNotes Pathophysio Serotonin: Basal GangliaSergi Lee OrateОценок пока нет
- CAMP - Cervical Radic - ColladoДокумент5 страницCAMP - Cervical Radic - ColladoSergi Lee OrateОценок пока нет
- Cebu Institute of Technology - University College of NursingДокумент2 страницыCebu Institute of Technology - University College of NursingSergi Lee OrateОценок пока нет
- CDUH TBI GosarinДокумент7 страницCDUH TBI GosarinSergi Lee OrateОценок пока нет
- Standa Modules 2022Документ39 страницStanda Modules 2022vlado_314Оценок пока нет
- Lecture 01 (Basics) ME141 PDFДокумент18 страницLecture 01 (Basics) ME141 PDFAlteaAlОценок пока нет
- Counter Affidavit SAMPLEДокумент7 страницCounter Affidavit SAMPLEChristle PMDОценок пока нет
- Scan 13 Aug 2020Документ6 страницScan 13 Aug 2020Armaan GarnayakОценок пока нет
- Abuajela Sreh - St5 Gastroenterology - Sheffield Teaching Hospitals 1 4 / 0 1 / 2 0 2 2Документ48 страницAbuajela Sreh - St5 Gastroenterology - Sheffield Teaching Hospitals 1 4 / 0 1 / 2 0 2 2sryh2012Оценок пока нет
- Chapter 3 Movement of Substances Across The Plasma MembraneДокумент45 страницChapter 3 Movement of Substances Across The Plasma MembraneNurul Husna100% (1)
- Rules For Classification: Inland Navigation VesselsДокумент42 страницыRules For Classification: Inland Navigation VesselsDmitrii PustoshkinОценок пока нет
- Internal Medicine Ethics JournalДокумент4 страницыInternal Medicine Ethics Journalzellinda kuswantoОценок пока нет
- Applications: FX-SC8XIOR34-0 Module Installation InstructionsДокумент16 страницApplications: FX-SC8XIOR34-0 Module Installation InstructionsUdo IheanachoОценок пока нет
- Kasus Ke 10 (Inggris)Документ5 страницKasus Ke 10 (Inggris)Fauzan AdvantageОценок пока нет
- Hydraulic Pump Unit 1 15Документ2 страницыHydraulic Pump Unit 1 15azry_alqadryОценок пока нет
- The Benefits of Drinking More Water Infographic - FINALДокумент1 страницаThe Benefits of Drinking More Water Infographic - FINALdanishayaz794Оценок пока нет
- JCS Complete Issue Volume 70 No 6Документ50 страницJCS Complete Issue Volume 70 No 6DanielleRuthPradoHipolitoОценок пока нет
- Project Report On Plastic Ban1Документ15 страницProject Report On Plastic Ban1Silas Wilson67% (3)
- Performance of Fracture MaterialsДокумент26 страницPerformance of Fracture MaterialsMedaculoОценок пока нет
- National Service Training Program 2 OrientationДокумент8 страницNational Service Training Program 2 OrientationAngelica SorianoОценок пока нет
- Nov Radiagreen MSDSДокумент4 страницыNov Radiagreen MSDSArifin IsawisemanОценок пока нет
- Familyresourcepage MiddleschoolДокумент2 страницыFamilyresourcepage Middleschoolapi-521845594Оценок пока нет
- SSCC1003 1617Документ6 страницSSCC1003 1617alyaa nishaОценок пока нет
- WestvirginiaДокумент6 страницWestvirginiaapi-280868990Оценок пока нет
- IT Projection ToolДокумент7 страницIT Projection ToolsaurabhmanitОценок пока нет
- Introduction EM Waves WorksheetДокумент3 страницыIntroduction EM Waves WorksheetUmer AbdullahОценок пока нет