Вам также может понравиться
- B. Diagram: Predisposing Factors: Precipitating Factors EtiologyДокумент3 страницыB. Diagram: Predisposing Factors: Precipitating Factors EtiologyKenneth Torres100% (1)
- Pcap - PathophysiologyДокумент4 страницыPcap - PathophysiologyAyla Mar100% (1)
- Pathophysiology of PneumoniaДокумент2 страницыPathophysiology of PneumoniaJesselle LasernaОценок пока нет
- Pathophysiology PneumoniaДокумент2 страницыPathophysiology PneumoniaSheila Mae Escalante67% (3)
- Pathophysiology of PneumoniaДокумент4 страницыPathophysiology of PneumoniaShermane Criszen F. Sallan100% (4)
- IX: Pathophysiology: Predisposing Factor Precipitating FactorsДокумент2 страницыIX: Pathophysiology: Predisposing Factor Precipitating FactorsCandace AlcarazОценок пока нет
- Patho PneumoniaДокумент2 страницыPatho Pneumoniaailyne_galicia100% (2)
- Pathophysiology of PneumoniaДокумент1 страницаPathophysiology of PneumoniaDarlene Clarice V. Labaclado67% (3)
- PP - Community-Acquired PneumoniaДокумент1 страницаPP - Community-Acquired Pneumonialpetallo100% (2)
- Cap PathophysiologyДокумент2 страницыCap PathophysiologyNoriel Henricks Acuna100% (3)
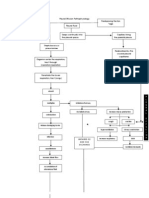
- Tuberculosis - TB - Pathophysiology - Schematic DiagramДокумент3 страницыTuberculosis - TB - Pathophysiology - Schematic DiagramCyrus De Asis90% (10)
- Pulmonary Tuberculosis Pathophysiology DiagramДокумент3 страницыPulmonary Tuberculosis Pathophysiology DiagramRisa Sol Arias80% (20)
- Pa Tho Physiology of DengueДокумент1 страницаPa Tho Physiology of Denguesinister17100% (1)
- Pathophysiology Community Aquired Pneumonia and AnemiaДокумент3 страницыPathophysiology Community Aquired Pneumonia and Anemiapa3kmedina100% (2)
- Pathophysiology of Pediatric Community Acquired PneumoniaДокумент2 страницыPathophysiology of Pediatric Community Acquired PneumoniaKeij AranetaОценок пока нет
- Pcap Pathophysiology PDFДокумент3 страницыPcap Pathophysiology PDFMikaela RamosОценок пока нет
- Pathophysiology With Anatomy and PhysiologyДокумент3 страницыPathophysiology With Anatomy and PhysiologyKaloy KamaoОценок пока нет
- Pathophysiology of PneumoniaДокумент2 страницыPathophysiology of PneumoniaAnn Wincel Nobleza82% (17)
- Pcap PathophysiologyДокумент3 страницыPcap PathophysiologyAko Gle C Mariz80% (10)
- Presentation onCAP MRДокумент92 страницыPresentation onCAP MRrouche100% (10)
- PneumoniaДокумент1 страницаPneumoniaAyen FornollesОценок пока нет
- Dengue PoathoДокумент6 страницDengue PoathoCleobebs Agustin100% (1)
- Pathophysiology of Dengue FeverДокумент1 страницаPathophysiology of Dengue FeverApple Mae100% (1)
- Pneumonia PathophysiologyДокумент1 страницаPneumonia PathophysiologyDee Sarajan100% (3)
- Munity Acquired Pneumonia PathoДокумент1 страницаMunity Acquired Pneumonia PathoJohanna Elaine Tandoc100% (1)
- Pathophysiology of TuberculosisДокумент3 страницыPathophysiology of TuberculosisFirenze Fil96% (56)
- Pathophysiology of PneumoniaДокумент4 страницыPathophysiology of PneumoniamatrixtrinityОценок пока нет
- Bronchial Asthma in Acute Exacerbation BAIAE Pathophysiology Schematic DiagramДокумент3 страницыBronchial Asthma in Acute Exacerbation BAIAE Pathophysiology Schematic DiagramVictor Angelo VeraОценок пока нет
- Pathophysiology of PneumoniaДокумент3 страницыPathophysiology of PneumoniaKylie Golindang100% (2)
- Pcap PathoДокумент2 страницыPcap PathoDiana Jean Abad Dacumos69% (13)
- Dengue Case StudyДокумент23 страницыDengue Case Studycutie_0023Оценок пока нет
- Upper Respiratory Tract InfectionДокумент26 страницUpper Respiratory Tract InfectionKylie Golindang67% (3)
- Case Presentation DengueДокумент3 страницыCase Presentation DengueLindel Assley Turqueza100% (1)
- Pathophysiology Dengue 2Документ4 страницыPathophysiology Dengue 2KatherineОценок пока нет
- Pathophysiology of PneumoniaДокумент1 страницаPathophysiology of Pneumoniaoxidalaj97% (31)
- PATHOPHYSIOLOGY-PTB - FinalДокумент1 страницаPATHOPHYSIOLOGY-PTB - FinaliamMye100% (1)
- Pathophysiology Acute Pyelonephritis: Precipitating FactorsДокумент2 страницыPathophysiology Acute Pyelonephritis: Precipitating Factorsgodwinkent888Оценок пока нет
- Pathophysiology of PneumoniaДокумент2 страницыPathophysiology of PneumoniaJeffrey Ramos100% (1)
- Pathophysiology of Koch's Disease (Tuberculosis) : Primary InfectionДокумент2 страницыPathophysiology of Koch's Disease (Tuberculosis) : Primary InfectionStephanie GapuzОценок пока нет
- Pathophysiology PneumoniaДокумент2 страницыPathophysiology Pneumoniapallavi100% (2)
- Pathophysiology of Potts DiseaseДокумент3 страницыPathophysiology of Potts DiseaseJoanna Marie M. dela Cruz100% (5)
- Pa Tho Physiology of TuberculosisДокумент3 страницыPa Tho Physiology of TuberculosisFlauros Ryu JabienОценок пока нет
- Mycobacterium Tuberculosis: Precipitating Factors: Predisposing FactorsДокумент1 страницаMycobacterium Tuberculosis: Precipitating Factors: Predisposing FactorsYoko Mae Yano100% (1)
- Book Based: Etiology: Tubercle Bacilli Precipitating Factors Predisposing FactorsДокумент7 страницBook Based: Etiology: Tubercle Bacilli Precipitating Factors Predisposing FactorsIrish EspinosaОценок пока нет
- Final PathophysiologyДокумент3 страницыFinal Pathophysiologyemely p. tangoОценок пока нет
- Patho Acute BronchiДокумент1 страницаPatho Acute BronchiMarianne Bagui DinglasanОценок пока нет
- Human Immunodeficiency Virus: LentiruvirusДокумент5 страницHuman Immunodeficiency Virus: Lentiruvirusjoyrena ochondraОценок пока нет
- Patient Based PathophysiologyДокумент2 страницыPatient Based PathophysiologyDeinielle Magdangal RomeroОценок пока нет
- San Gabriel, GMA, Cavite College of Nursing: Iv. Pathophysiology by The BookДокумент2 страницыSan Gabriel, GMA, Cavite College of Nursing: Iv. Pathophysiology by The BookSTEPHANIE LIBO-ONОценок пока нет
- TuberkulosisanakДокумент106 страницTuberkulosisanakUdin NicotinicОценок пока нет
- Bordetella: Drying - Highly Susceptible To Toxic Substance andДокумент38 страницBordetella: Drying - Highly Susceptible To Toxic Substance andkrstnkyslОценок пока нет
- Ajon Codp Web CausationДокумент3 страницыAjon Codp Web Causationapi-383804230Оценок пока нет
- Tuberculosis TB Pathophysiology Schematic DiagramДокумент3 страницыTuberculosis TB Pathophysiology Schematic Diagramkatrin anne f. carpenaОценок пока нет
- PATHOPHYSIOLOGY ShortДокумент4 страницыPATHOPHYSIOLOGY ShortBSN 2 - Sasis, Rusmaryte C.Оценок пока нет
- Patient Based PathophysiologyДокумент3 страницыPatient Based PathophysiologyJeizel IgnacioОценок пока нет
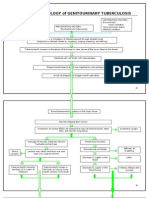
- Pathophysiology of Genitourinary TuberculosisДокумент8 страницPathophysiology of Genitourinary Tuberculosisace_51891Оценок пока нет
- Person With Silicosis, DM, Post Gastrectomy StateДокумент6 страницPerson With Silicosis, DM, Post Gastrectomy StatekhleeoОценок пока нет
- Pathophysiology of Tuberculous Peritonisis (Myobacterium Tuberculosis)Документ1 страницаPathophysiology of Tuberculous Peritonisis (Myobacterium Tuberculosis)Nathaniel SupanОценок пока нет
- QCHDДокумент1 страницаQCHDmidskiescreamzОценок пока нет
- TubercolosisДокумент7 страницTubercolosisVon LicudoОценок пока нет
- Lipsey and Chrystal Economics 11th Edition Free: Page 1 / 3Документ3 страницыLipsey and Chrystal Economics 11th Edition Free: Page 1 / 3MahmoudElbehairy100% (1)
- AVSEC Awareness Ground StaffДокумент12 страницAVSEC Awareness Ground Staffanon_823464996100% (2)
- Grounding-101 IEEE IAS PDFДокумент81 страницаGrounding-101 IEEE IAS PDFRoySnk100% (2)
- Basics of Industrial AutomationДокумент101 страницаBasics of Industrial Automationdeepak mallickОценок пока нет
- Project Wifi CrakДокумент12 страницProject Wifi CrakZain ButtОценок пока нет
- Biodiversity-2: Ramsar Convention On WetlandsДокумент9 страницBiodiversity-2: Ramsar Convention On WetlandsAhmad NawazОценок пока нет
- Part 1b - Selection and Literature Review of A CultureДокумент3 страницыPart 1b - Selection and Literature Review of A Cultureapi-535208903Оценок пока нет
- CV - Akhil AgarwalДокумент2 страницыCV - Akhil AgarwalIshan SaxenaОценок пока нет
- Air ConditionerДокумент131 страницаAir ConditionerRahul AnsariОценок пока нет
- Combustion and Flame: Victor Chernov, Qingan Zhang, Murray John Thomson, Seth Benjamin DworkinДокумент10 страницCombustion and Flame: Victor Chernov, Qingan Zhang, Murray John Thomson, Seth Benjamin DworkinVictor ChernovОценок пока нет
- Project ManagementДокумент6 страницProject ManagementVarunОценок пока нет
- Qualities of Effective Business LettersДокумент39 страницQualities of Effective Business Letterskrystel0% (1)
- Assigment On Reliance Industry: Master of Business Administration (Talentedge)Документ14 страницAssigment On Reliance Industry: Master of Business Administration (Talentedge)Mayank MalhotraОценок пока нет
- Internship Report On Deposit of Shahjalal Islami Bank LTDДокумент50 страницInternship Report On Deposit of Shahjalal Islami Bank LTDChowdhury Mahin Ahmed0% (1)
- God Only Knows Chords UkuleleДокумент3 страницыGod Only Knows Chords UkuleleMark0% (1)
- MaintGuideUSA PDFДокумент118 страницMaintGuideUSA PDFfotopredicОценок пока нет
- CSR ReportДокумент13 страницCSR Reportrishabh agarwalОценок пока нет
- Basso - 2001 - Neurobiological Relationships Between Ambient Ligh PDFДокумент11 страницBasso - 2001 - Neurobiological Relationships Between Ambient Ligh PDFVíctor MJОценок пока нет
- NCQC Answer Paper-1Документ4 страницыNCQC Answer Paper-1Shyamal KumarОценок пока нет
- 2012 Nike Football Clinic 4Документ2 страницы2012 Nike Football Clinic 4Bruno ChuОценок пока нет
- Hyperbolic FunctionsДокумент11 страницHyperbolic FunctionsShiraz NajatОценок пока нет
- Aim Efi Euro1 100 EngДокумент8 страницAim Efi Euro1 100 EngManuel RodriguezОценок пока нет
- Lino PresentationДокумент14 страницLino Presentationapi-356807903Оценок пока нет
- Crossroads #10 - Roger Zelazny's Amber - Seven No-TrumpДокумент254 страницыCrossroads #10 - Roger Zelazny's Amber - Seven No-TrumplerainlawlietОценок пока нет
- ModelsДокумент6 страницModelsUJJWALОценок пока нет
- Harsha Akka 013759 Unit 13 CRP Report PDFДокумент94 страницыHarsha Akka 013759 Unit 13 CRP Report PDFMinda RajanОценок пока нет
- How To Make VirtualBox From A Physical Partition - Ehow PDFДокумент4 страницыHow To Make VirtualBox From A Physical Partition - Ehow PDFyo_pupuОценок пока нет
- FILIPINO 2 LEARNING PLAN 3rd QuarterДокумент4 страницыFILIPINO 2 LEARNING PLAN 3rd QuarterMary Kryss DG SangleОценок пока нет
- Machine Elements in Mechanical Design Solution PDFДокумент309 страницMachine Elements in Mechanical Design Solution PDFazkonaОценок пока нет
- 3 ReviewsДокумент14 страниц3 ReviewsGabriela ZambranoОценок пока нет