Академический Документы
Профессиональный Документы
Культура Документы
HuangNicholsonThomas2018 AJA 18 0115ImpactofTaiChionBalanceDisorders SystematicReview
Загружено:
Daniel TorresАвторское право
Доступные форматы
Поделиться этим документом
Поделиться или встроить документ
Этот документ был вам полезен?
Это неприемлемый материал?
Пожаловаться на этот документАвторское право:
Доступные форматы
HuangNicholsonThomas2018 AJA 18 0115ImpactofTaiChionBalanceDisorders SystematicReview
Загружено:
Daniel TorresАвторское право:
Доступные форматы
See discussions, stats, and author profiles for this publication at: https://www.researchgate.
net/publication/332822755
Impact of Tai Chi Exercise on Balance Disorders: A Systematic Review
Article in American Journal of Audiology · May 2019
DOI: 10.1044/2018_AJA-18-0115
CITATIONS READS
0 15
3 authors, including:
Nannette Nicholson
Nova Southeastern University
31 PUBLICATIONS 87 CITATIONS
SEE PROFILE
Some of the authors of this publication are also working on these related projects:
Full moon june View project
All content following this page was uploaded by Nannette Nicholson on 28 May 2019.
The user has requested enhancement of the downloaded file.
AJA
Review Article
Impact of Tai Chi Exercise on Balance
Disorders: A Systematic Review
Hsin-Wei Huang,a Nannette Nicholson,b and Sheila Thomasc
Purpose: Tai chi is receiving increasing research attention with Results: Four studies met the inclusion criteria and were
its benefit of improving flexibility and balance. The objective included for data analysis. Results indicate positive effect
of this review was to examine the evidence concerning the of tai chi practice on dynamic postural stability in balance
impact of tai chi as a practical therapy for vestibular rehabilitation of its practitioners.
on individuals with balance and vestibular disorders. Conclusion: Tai chi may be a useful therapy as for vestibular
Method: A systematic review using 4 electronic databases rehabilitation as it improves dynamic balance control
was conducted. Randomized clinical trials and quasi- and flexibility of individuals with balance and vestibular
experimental studies were included. disorders.
P
eople with vestibular problems often experience Balance depends on proper function of vestibular, visual,
dizziness and trouble with balance, vision, or mo- and somatosensory systems, as well as other factors: muscle
bility. Vestibular disorders are associated with dys- strength, joint mobility, and cognition (Ganança, 2015).
function and deficit, unilateral or bilateral, in peripheral Balance impairment has a significant impact on health-
(outside the brain; part of the inner ear) and/or central system related quality of life of patients, especially on their emo-
(McDonnell & Hillier, 2015). Examples of these disorders tional and physical status (Gámiz & Lopez-Escamez, 2004;
include benign paroxysmal positional vertigo, vestibular Jacob, 1988; Lopez-Escamez, Gamiz, Fernandez-Perez,
neuritis, labyrinthitis, Ménière’s disease, and acoustic neuroma/ Gomez-Fiñana, & Sanchez-Canet, 2003).
vestibular schwannoma. Benign paroxysmal positional ver- Falls are reportedly the leading cause of physical and
tigo, for instance, a sudden vertigo induced by a change psychological trauma in population of age 65 years and
in head position (Hornibrook, 2011), is the most common older (Centers for Disease Control and Prevention [CDC],
disorder of the vestibular system in the inner ear that in- 2006). The risk of falls not only increases with age but is
creases in prevalence with age (Lawson, Johnson, Bamiou, also linked with balance and vestibular dysfunction, which
& Newton, 2005). Patients who undergo canalith reposi- has raised public health concerns (Scuffham, Chaplin, &
tioning maneuvers may show dizziness, insufficient postural Legood, 2003). A number of researchers proposed that
stability control, and increased risk of falls (Bressi et al., balance control ability and flexibility are associated with
2017; Di Girolamo et al., 1998). Moreover, vertiginous symp- falls, especially in the elderly population (Chiacchiero,
toms are often accompanied by elevated levels of anxiety and Dresely, Silva, DeLosReyes, & Vorik, 2010; Li et al., 2016;
emotional disturbance (Jacob, 1988). Dizziness is one of the Tse & Bailey, 1992). Participation in balance or muscle-
most common complaints among older adults (Furman, Raz, strengthening exercises can reduce the fall rate of this pop-
& Whitney, 2010; Hanley, O’Dowd, & Considine, 2001). ulation (CDC, 2006; Li et al., 2016; Tse & Bailey, 1992).
Tai chi, originally practiced as a martial art form by
the ancient Chinese (tai chi chuan), is an exercise derived
a
Department of Audiology and Speech Pathology, University of
from the martial art form consisting of slow, continuous,
Arkansas for Medical Sciences/University of Arkansas at Little Rock fluid movements for total self-development (Chang et al.,
b
Department of Audiology, Nova Southeastern University, 2011; Kuramoto, 2006). Physically, it is a gentle exercise
Fort Lauderdale, FL appropriate for older adults; mentally, it is a study of con-
c
Department of Library Education and Reference Services, University centration; spiritually, it is a practice of meditation (Galante,
of Arkansas for Medical Sciences, Little Rock 1981). Tai chi is also a preventive and curative branch in
Correspondence to Hsin-Wei Huang: hhuang2@uams.edu Chinese medicine (Kuramoto, 2006). Tai chi facilitates a
Editor-in-Chief: Sumitrajit Dhar number of health benefits, which include balance control,
Received July 13, 2018
Revision received December 3, 2018
Accepted December 10, 2018 Disclosure: The authors have declared that no competing interests existed at the time
https://doi.org/10.1044/2018_AJA-18-0115 of publication.
American Journal of Audiology • 1–14 • Copyright © 2019 American Speech-Language-Hearing Association 1
Downloaded from: https://pubs.asha.org Nannette Nicholson on 05/03/2019, Terms of Use: https://pubs.asha.org/pubs/rights_and_permissions
flexibility, blood pressure reduction, cardiovascular fitness, balance and vestibular disorders. This review further
pain reduction, and mood and self-esteem improvement explores the benefits of practicing tai chi to improve mobil-
(Blake & Batson, 2009; Kuramoto, 2006; Lauche et al., 2016; ity and balance, thereby reducing the risk of falls and
Sun et al., 2016; Wolf, Coogler, & Xu, 1997; Yeh, Wang, injuries.
Wayne, & Phillips, 2008).
Tai chi is receiving increasing research attention,
mainly because many studies have shown already that tai Method
chi is beneficial for improving flexibility and balance (Li This systematic review was conducted at the Univer-
et al., 2005; Nguyen, Taw, & Wang, 2013; Tsang, Wong, sity of Arkansas for Medical Sciences, with approval of
Fu, & Hui-Chan, 2004; Tse & Bailey, 1992; Wayne et al., the institutional review board (Protocol 206614). This sys-
2004; Wu, 2002; Zwick, Rochelle, Choksi, & Domowicz, tematic review was conducted following guidelines pro-
2000). Western science has recently been giving attention vided in the Cochrane Handbook for Systematic Reviews
to tai chi’s benefits as a form of preventive and rehabilita- of Interventions (Higgins & Green, 2011). Search terms
tive therapy, whereas the overall effectiveness has been well were generated using the PICO framework first suggested
documented in Chinese scientific literature. Tse and Bailey by Counsell in 1997. Counsell (1997) identified four impor-
(1992) conducted the first research in the West to evaluate tant components of a well-focused clinic question where
the influence that tai chi training has on postural control in P stands for population, I stands for intervention/exposure,
which they studied on the Chinese community of the greater C stands for comparison, and O stands for outcome mea-
Boston area. They reported that tai chi practitioners per- sure. These components are used to generate search terms
formed better on postural control tests than nonpractitioners, and strategies for electronic databases (see Table 1). Specif-
suggesting a positive link between tai chi and postural con- ically, we wanted to know if individuals with balance or
trol. In addition, they suggested that the performance could vestibular disorders benefited from tai chi (with or without
have been affected by many other variables such as envi- a comparison group) according to clinical and/or behav-
ronmental factors, activity history, interests, and occupa- ioral measures of dynamic balance and stability. Use of
tion. Zeeuwe et al. (2006) designed the first randomized the PICO terms facilitated the development of a systematic
clinical trial in Europe that examines tai chi chuan and fall search strategy used in relevant and available electronic
prevention. They evaluated the effect of tai chi chuan on databases (see Appendix A).
fall prevention and physical and psychological functions in A standard reporting tool recognized by most profes-
older Dutch adults. However, further information regarding sions was used to illustrate the flow of activities during
the efficacy of tai chi chuan and fall reduction is warranted. the publication identification and selection process. This
Chan and Bartlett (2000) evaluated the methodological tool is known as the Preferred Reporting Items for Sys-
rigor and conducted a meta-analysis using seven studies tematic Reviews and Meta-Analysis (PRISMA; Moher,
published between 1992 and 1998. They concluded that Liberati, Tetzlaff, Altman, & Prisma Group, 2009). The
the research evidence supporting the practice of tai chi as PRISMA depicts the total number of publications identi-
a way to improve balance and postural control is of moder- fied, the number of duplications, the number eliminated
ate quality. Furthermore, they noted that movements during the screening process based on exclusion criteria,
within tai chi mimic the actions of daily life and that tai the number included in the full-text critical appraisal, and
chi helps to develop body awareness, knowledge of one’s the number of publications included in the study.
body in its surroundings, and body reaction to movement. The Joanna Briggs Institute (JBI) checklists were
They proposed further investigation to determine the value used to screen studies for methodological rigor to deter-
of tai chi in promoting health and wellness. mine quality for inclusion in our systematic review (Pearson,
Tai chi as therapy has been studied in populations Wiechula, Court, & Lockwood, 2005). The JBI checklists
such as traumatic head injury (Blake & Batson, 2009), chronic have been developed individually for a wide variety of
neck pain (Lauche et al., 2016), fall prevention (Liu & study types (e.g., cohort, case control, quasi-experimental)
Frank, 2010; Logghe et al., 2010), and chronic medical and are available on their website (JBI, n.d.).
conditions (Wang, Collet, & Lau, 2004). Moreover, tai chi The Grading of Recommendations, Assessment,
has been utilized as a rehabilitative technique for stroke Development, and Evaluation (GRADE) scoring system
patients (Au-Yeung, Hui-Chan, & Tang, 2009; Taylor-Piliae of four categories (Guyatt et al., 2008) was used for the
et al., 2014), Parkinson’s disease (Hackney & Earhart, 2008; critical appraisal and rating of study strength and quality.
Li et al., 2012, 2014), and arthritis (Fransen, Nairn, Although the GRADE was designed by Guyatt et al. in
Winstanley, Lam, & Edmonds, 2007; Song, Lee, Lam, 2008, Goldet and Howick (2013) later developed a simpli-
& Bae, 2003). Although tai chi is believed to have physi- fied approach regarding how to best use this instrument to
ological and psychological benefits, improving quality of ascertain study strength and quality.
life (Wang et al., 2004), it is not widely recognized as an
intervention option for balance and vestibular disorders.
The purpose of this systematic review was to examine the Data Sources
evidence regarding the potential use of tai chi as a practical Publications were identified from the following Univer-
therapy for vestibular rehabilitation on individuals with sity of Arkansas for Medical Sciences electronic databases:
2 American Journal of Audiology • 1–14
Downloaded from: https://pubs.asha.org Nannette Nicholson on 05/03/2019, Terms of Use: https://pubs.asha.org/pubs/rights_and_permissions
Table 1. PICO framework.
PICO Description of detail
Participant (P) All patients of both sexes and all age groups with balance and vestibular disorders
Intervention (I) Use of tai chi as a practical therapy for vestibular rehabilitation on individuals with balance and vestibular
disorders
All styles of tai chi trainings were considered regardless of their forms, modifications (traditional or simplified),
and numbers of movements
Comparison (C) Following control groups were considered: patients who
(a) received no intervention
(b) conventional vestibular trainings
(c) rehabilitation including education, awareness, stress reduction, and exercises
Outcome (O) Clinical and/or behavioral measures to assess body and dynamic balance, dynamic gait function, neuromuscular
function, and trunk stability
Secondary outcome measures such as subjective evaluation of the symptom severity, relief of symptoms in
dizziness, level of confidence, and the impact of vestibular disorders in activities of daily living
Note. Adapted from Counsell (1997).
PubMed, CINAHL, PsycINFO, and Web of Science on non–peer-reviewed publications, and uncontrolled studies
December 8, 2016, by an author with expertise in the devel- were also excluded.
opment of systematic search strategies (S. T.). Additional
publications were identified from the Google Scholar data- Types of Participants
base on January 31, 2017. Publication references were also Studies were not limited by age or gender of partici-
reviewed for potential study inclusion. Irrelevant publica- pants. Participants with balance and vestibular disorders
tions were excluded by scanning their titles and abstracts. were included.
Two sets of search terms were used in each database. Terms
related to tai chi such as tai chi or taiji were searched and Types of Interventions
coupled with search terms related to balance and vestibular Studies investigating the use of tai chi as a practi-
disorders such as vertigo or dizziness or falls. Date limits cal therapy for vestibular rehabilitation on individuals
were not applied. The search terms and search strategy are with balance and vestibular disorders were included. In
shown in Appendix A. this review, all styles of tai chi trainings were considered
regardless of their forms, modifications (traditional or
simplified), and numbers of movements.
Inclusion/Exclusion Criteria
A priori inclusion criteria were extended from the Types of Controls
PICO question and organized by study design, type of Studies with the following control groups were con-
intervention, and outcome measures used. Inclusion was sidered: participants who received (a) no intervention,
limited to high-quality studies meeting strong methodologi- (b) conventional vestibular trainings, or (c) rehabilitation
cal rigor requirements. The studies included in this review including education, awareness, stress reduction, and
met the following criteria: (a) study design = randomized exercises.
controlled trials (RCTs) or quasi-experimental studies;
(b) intervention = tai chi; (c) outcome = clinical and/or be- Types of Outcome Measures
havioral measures of dynamic balance and stability. The All studies included in this review used clinical and/
following criteria were considered for exclusion: (a) studies or behavioral measures to assess body and dynamic bal-
not written in English; (b) reviews, letters, or comments ance, dynamic gait function, neuromuscular function, and
of original studies; and (c) incomplete data or data not trunk stability. Some of the studies also addressed second-
available. Duplicates were excluded. Inclusion was limited ary outcome measures such as subjective evaluation of
to studies published in English. the symptom severity, relief of symptoms in dizziness, level
of confidence, and the impact of vestibular disorders in
activities of daily living.
Study Selection
Types of Studies Data Extraction and Quality Assessment
Studies included in this review were either RCTs The reviewers (H. H. and N. N.) scanned the titles
or quasi-experimental studies. Trials in which tai chi and abstracts of all studies identified in the initial search
as an intervention was performed for impairments other to locate any relevant RCTs and quasi-experimental stud-
than balance and vestibular disorders were excluded. ies. Hardcopies of all studies meeting the inclusion criteria
Case studies, case series, qualitative studies, reviews, were obtained and read in full. Each study was read and
Huang et al.: Tai Chi and Balance Disorders 3
Downloaded from: https://pubs.asha.org Nannette Nicholson on 05/03/2019, Terms of Use: https://pubs.asha.org/pubs/rights_and_permissions
appraised independently by the two reviewers. Data from studies were from the United States, and one was from Po-
the studies were extracted according to criteria defined land. Two of the included studies adopted a two-armed
by the reviewers. Discrepancies were noted and discussed parallel group design, one employed a cross-over design,
between and resolved by consensus. Data were validated and one used a quasi-experimental design with four partici-
using a data extraction form (see Appendix B) designed for pant groups.
this study. The sample size ranged from 19 to 40 subjects ran-
The JBI checklists were used to assess the methodo- domized to either vestibular rehabilitation or the control
logical quality of the studies (Pearson et al., 2005). The intervention. Participants included in these studies were
JBI checklists consisted of a list of 13 and nine questions over 55 years (middle-age and older adults) of age. The
for RCTs and quasi-experimental studies, respectively. For study participants were drawn from both genders but were
each question, “yes” indicated a low risk of bias, “no” in- predominantly females. The participant data regarding
dicated a high risk of bias, and “unclear” indicated that balance and vestibular dysfunction were variable among
the risk of bias was uncertain. For the critical appraisal studies. Participants’ most common complaint was of im-
and rating of study quality, the GRADE scoring system of balance or postural instability with dizziness or vertigo. All
four categories was used (Goldet & Howick, 2013; Guyatt the included studies used modified tai chi movements and
et al., 2008). The final GRADE scores were assigned based postures. The movements and postures were selected and
on the overall scores for each comparison: high (at least adopted from traditional tai chi training selected accord-
4 points overall), moderate (3 points), low (2 points), ing to accuracy of multijoint trajectories, positioning, and
and very low (1 or less). If different GRADE scores were whole-body coordination. The number of treatment ses-
assigned by the two independent reviewers (H. H. and sions ranged from one to five times, lasting from 3 to
N. N.), characteristics of the study were discussed until 18 weeks (see Table 3).
consensus was reached.
Quality of Evidence
Data Analysis
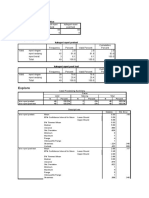
Table 4 presents a summary of the risk of bias within
Data were extracted and organized in summary ta- four studies included in this review. One of the three RCTs
bles. A summary table for study design, population, inter- included allocation concealment, whereas the other two
vention, comparison, outcome, and strength/quality rating reported poorly on the allocation sequence generation. Pa-
was developed. Data were further analyzed by develop- tients were blinded in only one of the RCTs, whereas pa-
ing a summary table to depict the intervention character- tients were not blinded in another RCT and the other one
istics and study findings. A meta-analysis could not be did not report clearly. None of the studies blinded the
performed due to the lack of homogeneity among study outcome assessor, or this feature was poorly described. The
designs, participants, intervention characteristics, and out- quasi-experimental study employed adequate methods to
come measures. clearly show reliability of data (Pearson et al., 2005).
The final GRADE scores are also shown in Table 4
Results (Goldet & Howick, 2013). One of the included studies was
rated high (4 points). One study was rated as moderate
Study Description (3 points) due to downgrading for lack of description of
The study flow was mapped in Figure 1 using the follow-up and withdrawals. Two studies were rated as low
PRISMA flow diagram (Moher et al., 2009). Following (2 points). One of the studies rated as low quality was an
execution of the search strategy, the reviewers identified RCT with incomplete reporting on blinding and allocation
a total of 1,614 publications for potential inclusion in the process; the other was the quasi-experimental study, pro-
systematic review. An initial review of titles and abstracts viding observational evidence.
resulted in identification of 45 relevant studies for full text
review. The remaining 1,569 publications were deemed
irrelevant or were duplicate studies and removed from Outcomes
further consideration (see Figure 1). The reviewers read The Timed Up and Go (Mathias, Nayak, & Isaacs,
45 studies in full and then excluded 41 of these studies. 1986; Podsiadlo & Richardson, 1991), Functional Reach
Thirty-six were excluded because interventions other than (Duncan, Weiner, Chandler, & Studenski, 1990), Single
tai chi were used or disorders other than balance and Stance Time (Fregly & Graybiel, 1966; Fregly, Smith, &
vestibular impairment were assessed. One study assessed Graybiel, 1973), and Tandem Stance Time tests (Graybiel
nonclinical and/or behavioral measures, such as quality & Fregly, 1965) are clinical measures to examine functional
of life, and four were non–peer-reviewed studies or reviews. mobility during standing up, sitting down, walking, reach-
Four studies met the criteria for methodological rigor and ing forward, standing on one leg, and tandem stance (Berg,
were included in the systematic review. Wood-Dauphinee, Williams, & Maki, 1992). In the Gatts
Four studies (three RCTs and one quasi-experimental and Woollacott (2006) study, results showed significant im-
study) were subjected to data extraction. Key features of provement ( p ≤ .0007) on all clinical/behavioral measures
these studies are presented in Table 2. Three of the four in Tai Chi Group 1 and significant improvement on five of
4 American Journal of Audiology • 1–14
Downloaded from: https://pubs.asha.org Nannette Nicholson on 05/03/2019, Terms of Use: https://pubs.asha.org/pubs/rights_and_permissions
Figure 1. Flow chart of the study selection.
the six measures (except for Stand on Left Leg, p ≤ .1641) ANOVA(H) = 5.04, p ≤ .024; maximum sway area:
in Control Group 2b with the tai chi cross-over. The ANOVA(H) = 8.86, p ≤ .002) for subjects participating
electromyography results demonstrated significant reduc- in tai chi exercise over the control group.
tion of the following outcome measures after tai chi train- Parameters assessed in the McGibbon et al. (2005)
ing: (a) tabialis anterior onset time (Group 1 by 50.25 ms, study consisted of dynamic gait function (time–distance
p ≤ .004; Group 2b by 17.36 ms, p ≤ .028) and (b) co- function), lower extremity motor control (mechanical
contraction (Group 1 from 50% to 0%, p ≤ .016). energy expenditures [MEEs]), and trunk stability (kine-
In the Lee, Jung, Abraham, Lei-Rivera, and Kim matics). The results demonstrated that tai chi and vestib-
(2012) experiment, the Activities-Specific Balance Confidence ular rehabilitation can improve gait function (gait speed:
Scale (ABC; Powell & Myers, 1995) and the Dynamic Gait p ≤ .009 in tai chi but p ≤ .060 in vestibular rehabilitation;
Index (DGI; Shumway-Cook & Woollacott, 1995) were step length: p ≤ .010 in tai chi and p ≤ .045 in vestibular
used to evaluate the utility of tai chi as an effective form rehabilitation; stance duration: p ≤ .055 in tai chi but p ≤ .044
of vestibular rehabilitation. The results revealed significant in vestibular rehabilitation). Moreover, tai chi improved
improvement (2.617, p ≤ .047) on ABC in Group 1 (nor- lower extremity motor control more than vestibular rehabil-
mal vestibular testing) and significant improvement (3.87, itation (reduced relative hip concentric MEE: p ≤ .001,
p ≤ .003) on DGI on Group 2 (abnormal vestibular testing). adjusted α = .017; and increased relative ankle concentric
However, there was no significant difference in Group 3 MEE: p ≤ .019, adjusted α = .025) by selective redistribu-
(central) and Group 4 (indeterminate). tion of joint energetics. The correlation revealed a stronger
Body balance was studied by using the 8 Foot Up gait and better trunk control.
and Go Test (Rikli & Jones, 1999) and Computer Posturo-
graphy for the limits of stability in the Maciaszek and
Osinski (2012) study. The results showed significant Discussion
improvement in four parameters (8 Foot Up and Go: Falls are the leading cause of physical and psycho-
ANOVA(H) = 8.32, p ≤ .003; forward deflection: logical trauma in the elderly population, each year affecting
ANOVA(H) = 3.70, p ≤ .050; backward deflection: approximately 30% of people of age 65 years and above
Huang et al.: Tai Chi and Balance Disorders 5
Downloaded from: https://pubs.asha.org Nannette Nicholson on 05/03/2019, Terms of Use: https://pubs.asha.org/pubs/rights_and_permissions
6
American Journal of Audiology • 1–14
Table 2. Summary of characteristics of tai chi for vestibular rehabilitation.
Population
GRADE Sample size (sex, Mean age Intervention (regimen) Control (regimen) Outcome
Study Design scoring male/female) years) (n = male/female) (n = male/female) measures
Gatts & Randomized Moderate 19 (2/17) 77.55 (TC) Simplified tai chi exercises (VT) Balance education, Clinical/behavioral:
Woollacott control (3 points) and repetition of 12 traditional awareness education, 1. Timed Up and Go
(2006) Control/ postures stress reduction, deep 2. Functional Reach
cross-over (90 min, 5 times weekly for breathing, and axial 3. Single Stance Time
3 weeks; n = 11 (1/10)) mobility exercise (90 min, 4. Tandem Stance Time
5 times weekly for Lab:
3 weeks; n = 8 (1/7)) Electromyography
1. tabialis anterior
2. medial gastrocnemius
Lee et al. Quasi- Low 37 (6/31) 72.30 (2, 3, 4) 16 Movements of Yang (1) 16 Movements of Yang 1. Activities-Specific
(2012) experimental (2 points) 1: Normal style with modification to suit style (45 min, 1 time Balance Scale
2: Vestibular each participant’s needs weekly for 8 weeks; 2. Dynamic Gait Index
Pre and post 3: Central (45 min, 1 time weekly for 8 weeks; n = 6)
4: Indeterminate n = 31)
Maciaszek & Randomized Low 40 69.70 (E) 5 sequences of movement (K) No tai chi intervention 1. 8 Foot Up and Go
Osinski control (2 points) chosen from the simplified (n = 20) 2. Computer Posturographic
(2012) 24 forms of tai chi System PE 90
(45 min, 2 times weekly for
18 weeks; n = 20)
McGibbon Randomized High 36 (16/20) 59.50 (TC) 5 movements of Yang-style (VR) eye–head coordination 1. Time–distance measure
et al. control (4 points) short form exercise, VOR training, for dynamic
(2005) (70 min, 1 time weekly for balance retraining exercise gait function
10 weeks; n = 19) (70 min, 1 time weekly 2. Mechanical energy
for 10 weeks; n = 17) expenditures for lower
extremity neuromuscular
control
3. Kinematics for trunk stability
Note. GRADE = Grading of Recommendations, Assessment, Development, and Evaluation; TC = tai chi; VT = vestibular training; E = experimental group with tai chi exercise;
K = control group; VR = vestibular rehabilitation; vestibulo-ocular reflex.
Downloaded from: https://pubs.asha.org Nannette Nicholson on 05/03/2019, Terms of Use: https://pubs.asha.org/pubs/rights_and_permissions
Table 3. Summary of tai chi intervention.
Total
Study Style session Movement Rationales of selection
Gatts & Yang 90 min, 12 Postures:commencement, white stork Traditional tai chi training
Woollacott Simplified 5 times cools its wing, brush knee, play the Tai chi chuan: the 27 forms
(2006) weekly for guitar, repulse monkey, heel kick,
3 weeks toe kick, golden cockerel, fair lady
21 hr total works the shuttles, part the wild
horses’ mane, cloud hands, cross
hands
Lee et al. Yang 45 min, 16 Movements: Traditional Yang style
(2012) Modified 1 time bow stance, bow and arrow, first tai chi
weekly for movement, gathering, polishing the
8 weeks table top, gathering energy, punching,
6 hr total stepping, stoking the fire, pitching,
turning the wheel, embrace the moon,
crane spreads wings, swimming, rooster
stands on 1 leg, repulse monkey
Maciaszek & Wuduan 45 min, 5 Sequences: 24-Form tai chi chuan
Osinski tai chi 2 times commencement, part the wild horses’ Yang style
(2012) chuan weekly for mane, white stork cools its wing,
Simplified 18 weeks brush knee, strums the lute, repulse
27 hr total monkey, grasp the bird’s tail, cloud
hands, single whip, high pat on horse,
rooster stands on 1 leg, needle to the
bottom of the sea, cross hands
McGibbon Yang 70 min, 5 Movements: Cheng Man-Ching’s
et al. Simplified 1 time rising the power, withdraw and push, Yang-style short form
(2005) weekly for cloud hands, brush knee twist step,
10 weeks separate right and left legs
11 hr total
(CDC, 2006). Research suggests that participation in bal- in this systematic review, the lack of homogeneity in terms
ance or muscle strengthening exercises can reduce the fall of outcome measures, styles, duration, and frequency of
rate of this population (Bergamaschi, Ferrari, Gallamini, the tai chi intervention among studies selected made it dif-
& Scoppa, 2011; CDC, 2006; Li et al., 2016). Tai chi is a ficult to establish the best protocol, other ideal parameters,
long-established martial art form that has been recognized or time of intervention to optimize health outcomes.
as an exercise, especially for elderly people (Chang et al., Two of the three RCTs were found to be of moder-
2011; Kuramoto, 2006; Tse & Bailey, 1992; Wolf et al., ate to low quality according to the GRADE scoring system
1996; Wolf, Coogler, et al., 1997). The literature demon- due to lack of clear reporting of allocation concealment or
strates that tai chi offers numerous cardiopulmonary, blinding of participants. None of the three RCTs blinded
musculoskeletal, and postural benefits to its practitioners the outcomes assessors or therapists, or if blinding was
(Kuramoto, 2006; Tse & Bailey, 1992; Wolf, Coogler, et al., used, it was poorly described. Lack of blinding increases
1997). Many studies have revealed that performance on the risk of biased results; thus, the strength of the evi-
balance outcome measures can be improved by practicing dence coming from these studies decreased. Although
tai chi (Kuramoto, 2006; Liu & Frank, 2010; Verhagen, the quasi-experimental study employed adequate methods
Immink, van der Meulen, & Bierma-Zeinstra, 2004; Wu, to show clearly the reliability, it was found to be of low
2002). Furthermore, tai chi has been utilized as a rehabilita- quality according to the GRADE scoring. This rating
tive technique for stroke patients (Au-Yeung et al., 2009; scale downgrades the research design because it was not
Taylor-Piliae et al., 2014), Parkinson’s disease (Hackney & an RCT and only provided observational evidence. In
Earhart, 2008; Li et al., 2012, 2014), and arthritis (Fransen addition, the sample size (ranged from 19 to 40 subjects)
et al., 2007; Song et al., 2003). may not have been sufficient to establish the validity of
Collectively, the results of the existing studies suggest the results found due to the variability in assessments and
that tai chi can be a practical complementary therapy interventions.
for vestibular rehabilitation as it is beneficial to individ- Although all studies selected (three RCTs and one
uals with symptoms, complaints, or a diagnosis of balance quasi-experimental study) reported positive significant
and vestibular impairment. Tai chi is a helpful practice findings on dynamic balance and improved gait and pos-
that can be used to improve flexibility and balance control tural performance, different parameters were used to as-
(Li et al., 2005; Nguyen et al., 2013; Tsang et al., 2004; sess body balance function. In the Gatts and Woollacott
Wayne et al., 2004; Wu, 2002; Zwick et al., 2000). However, (2006) study, functional mobility was examined using
Huang et al.: Tai Chi and Balance Disorders 7
Downloaded from: https://pubs.asha.org Nannette Nicholson on 05/03/2019, Terms of Use: https://pubs.asha.org/pubs/rights_and_permissions
Table 4. Critical appraisal and Grading of Recommendations, Assessment, Development, and Evaluation (GRADE) scoring of included
randomized controlled trials (RCTs).
Gatts &
Woollacott Lee et al. Maciaszek & McGibbon
Study (2006) (2012) Osinski (2012) et al. (2005)
Randomized controlled trails
1. Was true randomization used for assignment of participants to Y Y Y
treatment group?
2. Was allocation to treatment group concealed? U U Y
3. Were treatment groups similar at the baseline? Y Y Y
4. Were participants blind to treatment assignment? N U Y
5. Were those delivering treatment blind to treatment assignment? N N Y
6. Were outcomes assessors blind to treatment assignment? U N U
7. Were treatment groups treated identically other than the intervention Y Y Y
of interest?
8. Was follow-up complete, and if not, were differences between groups Y Y Y
in terms of their follow-up adequately described and analyzed?
9. Were participants analyzed in the groups to which they were randomized? Y Y Y
10. Were outcomes measured in the same way for treatment groups? Y Y Y
11. Were outcomes measured in a reliable way? Y Y Y
12. Was appropriate statistical analysis used? Y Y Y
13. Was the trial design appropriate, and any deviations from the standard Y U Y
RCT design accounted for in the conduct and analysis of the trial?
Quasi-experimental study
1. Is it clear in the study what is the “cause” and what is the “effect” Y
(i.e., there is no confusion about which variable comes first)?
2. Were the participants included in any comparisons similar? Y
3. Were the participants included in any comparisons receiving similar Y
treatment/care, other than the exposure or intervention of interest?
4. Was there a control group? Y
5. Were there multiple measurements of the outcome both pre and post Y
the intervention/exposure?
6. Was follow-up complete, and if not, were differences between groups Y
n terms of their follow-up adequately described and analyzed?
7. Were the outcomes of participants included in any comparisons measured Y
in the same way?
8. Were outcomes measured in a reliable way? Y
9. Was appropriate statistical analysis used? Y
GRADE scoring M (3) L (2) L (2) H (4)
Note. Questions of quality assessment are based on the Joanna Briggs Institute critical appraisal checklist. Y = yes; N = no; U = unclear;
H = high; M = moderate; L = low.
clinical/behavioral and electromyography measures. In the Some authors suggest that individuals with balance/
Lee et al. (2012) experiment, the ABC and the DGI were vestibular dysfunction and reduced memory ability may be
used to evaluate the utility of tai chi as an effective form better to start with short forms (Liu & Frank, 2010). Which
of vestibular rehabilitation. Body balance was studied by form should be selected depends on the individual tai chi
using the 8 Foot Up and Go Test and Computer Posturo- practitioner’s ability to perform particular body move-
graphy for the limits of stability in the Maciaszek and ments, which may vary extensively between forms and im-
Osinski (2012) study. Dynamic gait function, MEEs, and pact the practitioners’ ability to receive benefit from tai chi
trunk kinematics were the parameters used in the McGibbon (Liu & Frank, 2010). As Liu and Frank (2010) suggested,
et al. (2005) study. Moreover, uncertain vestibular dysfunc- shorter duration (< 12 weeks) may be better for more func-
tion limited the comparison; only the quasi-experimental tionally independent individuals, but it usually requires
study (Lee et al., 2012) demonstrated group-specific re- increased frequency and session length. On the contrary,
sponses of change attributed to tai chi therapy (Group 1: long duration with less frequency may provide supportive
normal vestibular; Group 2: abnormal vestibular; Group 3: effect on those who have a balance/vestibular deficit (Wolf
central; Group 4: indeterminate). et al., 1996). Several studies proposed that the selection
The duration and frequency of the exercise protocols of tai chi exercise parameters could have an impact on the
were variable among the studies (ranged from 6 to 27 hr outcome measures after tai chi training (Liu & Frank, 2010;
in total). As demonstrated in this review, the Yang style is Wolf et al., 1996). Additional research is needed to deter-
the most common style used for tai chi training. Numbers of mine the influence of practice frequency and intensity on
tai chi forms vary from short (five forms) to long (108 forms). balance and/or vestibular outcomes.
8 American Journal of Audiology • 1–14
Downloaded from: https://pubs.asha.org Nannette Nicholson on 05/03/2019, Terms of Use: https://pubs.asha.org/pubs/rights_and_permissions
This review has several limitations. First of all, we Blake, H., & Batson, M. (2009). Exercise intervention in brain
limited our search to publications written in English due injury: A pilot randomized study of tai chi qigong. Clinical
to difficulties in retrieving articles from databases in differ- Rehabilitation, 23(7), 589–598.
Bressi, F., Vella, P., Casale, M., Moffa, A., Sabatino, L., Lopez,
ent languages, such as Chinese and Japanese. Although
M. A., . . . Sterzi, S. (2017). Vestibular rehabilitation in benign
adherence to systematic review strategies as a method in paroxysmal positional vertigo: Reality or fiction. International
this review was observed, selective publishing and report- Journal of Immunopathology and Pharmacology, 30, 113–122.
ing may pose a potential publication bias. Results would Centers for Disease Control and Prevention. (2006). Fatalities
have been more inclusive if we had been able to include and injuries from falls among older adults—United States,
studies written in other languages; this would have required 1993–2003 and 2001–2005. MMWR: Morbidity and Mortality
additional language skills of our team members. Moreover, Weekly Report, 55(45), 1221–1224.
although we made a great effort to retrieve all the RCTs Chan, W. W., & Bartlett, D. J. (2000). Effectiveness of tai chi
on the subject, we cannot be certain that our search located as a therapeutic exercise in improving balance and postural
all the relevant trials. Further limitations include the pau- control. Physical & Occupational Therapy in Geriatrics, 17(3),
1–22.
city, homogeneity, and the frequently suboptimal methodo-
Chang, J. Y., Tsai, P. F., Beck, C., Hagen, J., Huff, D. C., Anand,
logical quality of primary data. These factors influence K. J., . . . Beuscher, L. (2011). The effect of tai chi on cognition
both quality and quantity of the research studies reviewed in elders with cognitive impairment. Medsurg Nursing, 20(2),
and limit the conclusions that we can make in the basis of 63–69.
this systematic review. Despite the limitations and varia- Chiacchiero, M., Dresely, B., Silva, U., DeLosReyes, R., &
tions between studies, according to the results of this inves- Vorik, B. (2010). The relationship between range of move-
tigation, tai chi shows to be effective in improving balance ment, flexibility, and balance in the elderly. Topics in Geri-
control as well as gait and postural performance. These atric Rehabilitation, 26(2), 148–155.
results will help guide clinical decisions regarding the use of Counsell, C. (1997). Formulating questions and locating primary
studies for inclusion in systematic reviews. Annals of Internal
tai chi as a complementary means of rehabilitation treat-
Medicine, 127(5), 380–387.
ment such as repositioning procedures for patients to cope Di Girolamo, S., Paludetti, G., Briglia, G., Cosenza, A., Santarelli,
with discomfort. Further scientific investigation is needed R., & Di Nardo, W. (1998). Postural control in benign parox-
in the future. ysmal positional vertigo before and after recovery. Acta Oto-
Laryngologica, 118(3), 289–293.
Duncan, P. W., Weiner, D. K., Chandler, J., & Studenski, S.
Conclusion (1990). Functional reach: A new clinical measure of balance.
Although tai chi is receiving growing attention, there Journals of Gerontology: Series A: Biological Sciences and
were a surprisingly limited number of high-quality studies Medical Sciences, 45(6), M192–M197.
Fransen, M., Nairn, L., Winstanley, J., Lam, P., & Edmonds, J.
regarding the benefits of tai chi as a rehabilitative strategy
(2007). Physical activity for osteoarthritis management: A
to reduce fall risk for inclusion in this study. Therefore, randomized controlled clinical trial evaluating hydrotherapy
this systematic review elucidates the need for further inves- or tai chi classes. Arthritis Care & Research, 57(3), 407–414.
tigation of tai chi as an intervention for balance/vestibular Fregly, A. R., & Graybiel, A. (1966). An ataxia test battery not
disorders using a high-quality research design. Results of requiring the use of rails (No. NAMI-985). Pensacola, FL:
this study demonstrated that tai chi improves dynamic bal- Naval Aerospace Medical Institute.
ance control and flexibility of individuals with balance and Fregly, A. R., Smith, M. J., & Graybiel, A. (1973). Revised nor-
vestibular disorders. However, the number, size, and qual- mative standards of performance of men on a quantitative
ity of the RCTs are not sufficient at this time to draw deci- ataxia test battery. Acta Oto-Laryngologica, 75(1), 10–16.
sive conclusions regarding dosage and effectiveness as an Furman, J. M., Raz, Y., & Whitney, S. L. (2010). Geriatric vesti-
bulopathy assessment and management. Current Opinion in
intervention. Additional well-designed clinical trials are
Otolaryngology & Head and Neck Surgery, 18(5), 386–391.
needed to substantiate the effects of tai chi as a vestibular Galante, L. (1981). Tai chi: The supreme ultimate. Newburyport,
rehabilitation option for certain disorders, especially ves- MA: Weiser Books.
tibular dysfunction, as well as the optimal treatment dura- Gámiz, M. J., & Lopez-Escamez, J. A. (2004). Health-related
tion necessary to avoid recurrence of symptoms. quality of life in patients over sixty years old with benign
paroxysmal positional vertigo. Gerontology, 50(2), 82–86.
Ganança, M. M. (2015). Vestibular disorders in the elderly.
References Brazilian Journal of Otorhinolaryngology, 81(1), 4–5.
Au-Yeung, S. S., Hui-Chan, C. W., & Tang, J. C. (2009). Short- Gatts, S. K., & Woollacott, M. H. (2006). Neural mechanisms under-
form tai chi improves standing balance of people with chronic lying balance improvement with short term tai chi training.
stroke. Neurorehabilitation and Neural Repair, 23(5), 515–522. Aging Clinical and Experimental Research, 18(1), 7–19.
Berg, K. O., Wood-Dauphinee, S. L., Williams, J. I., & Maki, B. Goldet, G., & Howick, J. (2013). Understanding GRADE: An in-
(1992). Measuring balance in the elderly: Validation of an troduction. Journal of Evidence-Based Medicine, 6(1), 50–54.
instrument. Canadian Journal of Public Health, 83, S7–S11. Graybiel, A., & Fregly, A. R. (1965). A new quantitative ataxia test
Bergamaschi, M., Ferrari, G., Gallamini, M., & Scoppa, F. (2011). battery [Research Report, NSAM-919]. Pensacola, FL: United
Laser acupuncture and auriculotherapy in postural instability States Naval School of Aviation Medicine.
—A preliminary report. Journal of Acupuncture and Meridian Guyatt, G. H., Oxman, A. D., Vist, G. E., Kunz, R., Falck-Ytter,
Studies, 4(1), 69–74. Y., Alonso-Coello, P., & Schünemann, H. J. (2008). GRADE:
Huang et al.: Tai Chi and Balance Disorders 9
Downloaded from: https://pubs.asha.org Nannette Nicholson on 05/03/2019, Terms of Use: https://pubs.asha.org/pubs/rights_and_permissions
An emerging consensus on rating quality of evidence and Lopez-Escamez, J. A., Gamiz, M. J., Fernandez-Perez, A., Gomez-
strength of recommendations. BMJ (Clinical Research Ed.), Fiñana, M., & Sanchez-Canet, I. (2003). Impact of treatment
336(7650), 924–926. on health-related quality of life in patients with posterior canal
Hackney, M. E., & Earhart, G. M. (2008). Tai chi improves bal- benign paroxysmal positional vertigo. Otology & Neurotology,
ance and mobility in people with Parkinson disease. Gait & 24(4), 637–641.
Posture, 28(3), 456–460. Maciaszek, J., & Osinski, W. (2012). Effect of Tai Chi on body
Hanley, K., O’Dowd, T., & Considine, N. (2001). A systematic balance: Randomized controlled trial in elderly men with
review of vertigo in primary care. The British Journal of Gen- dizziness. The American Journal of Chinese Medicine, 40(2),
eral Practice, 51(469), 666–671. 245–253.
Higgins, J. P. T., & Green, S. (Eds.). (2011). Cochrane handbook Mathias, S., Nayak, U. S., & Isaacs, B. (1986). Balance in elderly
for systematic reviews of interventions (Version 5.1.0) [updated patients: The “get-up and go” test. Archives of Physical
March 2011]. The Cochrane Collaboration. Retrieved from Medicine and Rehabilitation, 67(6), 387–389.
http://handbook.cochrane.org McDonnell, M. N., & Hillier, S. L. (2015). Vestibular rehabilita-
Hornibrook, J. (2011). Benign paroxysmal positional vertigo (BPPV): tion for unilateral peripheral vestibular dysfunction. Cochrane
History, pathophysiology, office treatment and future directions. Database of Systematic Reviews, 2015(1), Art. No. CD005397.
International Journal of Otolaryngology, 2011, 1–13. https://doi. https://doi.org/10.1002/14651858.cd005397.pub4
org/10.1155/2011/835671 McGibbon, C. A., Krebs, D. E., Parker, S. W., Scarborough,
Jacob, R. G. (1988). Panic disorder and the vestibular system. D. M., Wayne, P. M., & Wolf, S. L. (2005). Tai chi and
Psychiatric Clinics of North America, 11(2), 361–374. vestibular rehabilitation improve vestibulopathic gait via dif-
Joanna Briggs Institute. (n.d.). Critical appraisal tools. Retrieved ferent neuromuscular mechanisms: Preliminary report. BMC
from http://joannabriggs.org/research/critical-appraisal-tools. Neurology, 5(1), 3.
html Moher, D., Liberati, A., Tetzlaff, J., Altman, D. G., & Prisma
Kuramoto, A. M. (2006). Therapeutic benefits of tai chi exercise: Group. (2009). Preferred reporting items for systematic reviews
Research review. WMJ: Official Publication of the State Medi- and meta-analyses: The PRISMA statement. PLoS Medicine,
cal Society of Wisconsin, 105(7), 42–46. 6(7), e1000097.
Lauche, R., Stumpe, C., Fehr, J., Cramer, H., Cheng, Y. W., Nguyen, C. T., Taw, M. B., & Wang, M. B. (2013). Complemen-
Wayne, P. M., . . . Dobos, G. (2016). The effects of tai chi and tary and integrative treatments: Balance disorders. Otolaryngo-
neck exercises in the treatment of chronic nonspecific neck logic Clinics of North America, 46(3), 409–422.
pain: A randomized controlled trial. The Journal of Pain, Pearson, A., Wiechula, R., Court, A., & Lockwood, C. (2005). The
17(9), 1013–1027. JBI model of evidence-based healthcare. International Journal
Lawson, J., Johnson, I., Bamiou, D. E., & Newton, J. L. (2005). of Evidence-Based Healthcare, 3(8), 207–215.
Benign paroxysmal positional vertigo: Clinical characteristics Podsiadlo, D., & Richardson, S. (1991). The timed “Up & Go”:
of dizzy patients referred to a falls and syncope unit. QJM: An A test of basic functional mobility for frail elderly persons. Jour-
International Journal of Medicine, 98(5), 357–364. nal of the American Geriatrics Society, 39(2), 142–148.
Lee, P. S., Jung, M., Abraham, A., Lei-Rivera, L., & Kim, A. H. Powell, L. E., & Myers, A. M. (1995). The Activities-Specific
(2012). Efficacy of tai chi as a technique for vestibular Balance Confidence Scale (ABC). Journals of Gerontology
rehabilitation—A preliminary quasi-experimental study. Jour- Series A: Biological Sciences and Medical Sciences, 50(1),
nal of Physical Therapy, 5(1), 6–13. M28–M34.
Li, F., Harmer, P., Fisher, K. J., McAuley, E., Chaumeton, N., & Rikli, R. E., & Jones, C. J. (1999). Development and validation
Eckstrom, E. (2016). Adoption of a tai chi intervention, tai ji of a functional fitness test for community-residing older adults.
quan: Moving for better balance, for fall prevention by rural Journal of Aging and Physical Activity, 7(2), 129–161.
faith-based organizations, 2013–2014. Preventing Chronic Dis- Scuffham, P., Chaplin, S., & Legood, R. (2003). Incidence and
ease, 13, E92. costs of unintentional falls in older people in the United
Li, F., Harmer, P., Fisher, K. J., McAuley, E., Chaumeton, N., Kingdom. Journal of Epidemiology & Community Health,
Eckstrom, E., & Wilson, N. L. (2005). Tai chi and fall reduc- 57(9), 740–744.
tions in older adults: A randomized controlled trial. The Shumway-Cook, A., & Woollacott, M. H. (1995). Theories of
Journals of Gerontology Series A: Biological Sciences and motor control. Motor control theory and practical applications
Medical Sciences, 60(2), M187–M194. (pp. 3–18). Baltimore, MD: Lippincott, Williams & Wilkins.
Li, F., Harmer, P., Fitzgerald, K., Eckstrom, E., Stock, R., Galver, Song, R., Lee, E. O., Lam, P., & Bae, S. C. (2003). Effects of tai
J., . . . Batya, S. S. (2012). Tai chi and postural stability in chi exercise on pain, balance, muscle strength, and perceived
patients with Parkinson’s disease. New England Journal of difficulties in physical functioning in older women with osteo-
Medicine, 366(6), 511–519. arthritis: A randomized clinical trial. The Journal of Rheuma-
Li, F., Harmer, P., Liu, Y., Eckstrom, E., Fitzgerald, K., Stock, tology, 30(9), 2039–2044.
R., & Chou, L. S. (2014). A randomized controlled trial of Sun, W., Zhang, C., Song, Q., Li, W., Cong, Y., Chang, S., . . .
patient-reported outcomes with tai chi exercise in Parkinson’s Hong, Y. (2016). Effect of 1-year regular tai chi on neuro-
disease. Movement Disorders, 29(4), 539–545. muscular reaction in elderly women: A randomized controlled
Liu, H., & Frank, A. (2010). Tai chi as a balance improvement study. Research in Sports Medicine, 24(2), 145–156.
exercise for older adults: A systematic review. Journal of Geri- Taylor-Piliae, R. E., Hoke, T. M., Hepworth, J. T., Latt, L. D.,
atric Physical Therapy, 33(3), 103–109. Najafi, B., & Coull, B. M. (2014). Effect of tai chi on physical
Logghe, I. H., Verhagen, A. P., Rademaker, A. C., Bierma- function, fall rates and quality of life among older stroke
Zeinstra, S. M., van Rossum, E., Faber, M. J., & Koes, B. W. survivors. Archives of Physical Medicine and Rehabilitation,
(2010). The effects of tai chi on fall prevention fear of falling 95(5), 816–824.
and balance in older people: A meta-analysis. Preventive Tsang, W. W., Wong, V. S., Fu, S. N., & Hui-Chan, C. W. (2004).
Medicine, 51(3), 222–227. tai chi improves standing balance control under reduced or
10 American Journal of Audiology • 1–14
Downloaded from: https://pubs.asha.org Nannette Nicholson on 05/03/2019, Terms of Use: https://pubs.asha.org/pubs/rights_and_permissions
conflicting sensory conditions. Archives of Physical Medicine balance training. Journal of the American Geriatrics Society,
and Rehabilitation, 85(1), 129–137. 44(5), 489–497.
Tse, S. K., & Bailey, D. M. (1992). T’ai chi and postural control Wolf, S. L., Coogler, C., & Xu, T. (1997). Exploring the basis
in the well elderly. American Journal of Occupational Therapy, for tai chi chuan as a therapeutic exercise approach. Archives
46(4), 295–300. of Physical Medicine and Rehabilitation, 78(8), 886–892.
Verhagen, A. P., Immink, M., van der Meulen, A., & Bierma- Wu, G. (2002). Evaluation of the effectiveness of tai chi for im-
Zeinstra, S. M. (2004). The efficacy of tai chi chuan in proving balance and preventing falls in the older population—
older adults: A systematic review. Family Practice, 21(1), A review. Journal of the American Geriatrics Society, 50(4),
107–113. 746–754.
Wang, C., Collet, J. P., & Lau, J. (2004). The effect of tai chi Yeh, G. Y., Wang, C., Wayne, P. M., & Phillips, R. S. (2008).
on health outcomes in patients with chronic conditions: A The effect of tai chi exercise on blood pressure: A systematic
systematic review. Archives of Internal Medicine, 164(5), review. Preventive Cardiology, 11(2), 82–89.
493–501. Zeeuwe, P. E., Verhagen, A. P., Bierma-Zeinstra, S. M., van Rossum,
Wayne, P. M., Krebs, D. E., Wolf, S. L., Gill-Body, K. M., E., Faber, M. J., & Koes, B. W. (2006). The effect of tai chi chuan
Scarborough, D. M., McGibbon, C. A., . . . Parker, S. W. in reducing falls among elderly people: Design of a randomized
(2004). Can tai chi improve vestibulopathic postural con- clinical trial in the Netherlands [ISRCTN98840266]. BMC
trol. Archives of Physical Medicine and Rehabilitation, 85(1), Geriatrics, 6(1), 6.
142–152. Zwick, D., Rochelle, A., Choksi, A., & Domowicz, J. (2000). Evalua-
Wolf, S. L., Barnhart, H. X., Kutner, N. G., McNeely, E., tion and treatment of balance in the elderly: A review of the
Coogler, C., & Xu, T. (1996). Reducing frailty and falls efficacy of the Berg Balance Test and Tai Chi Quan. Neuro-
in older persons: An investigation of tai chi and computerized Rehabilitation, 15(1), 49–56.
Appendix A ( p. 1 of 2)
Search Strategies 12/08/2016
PubMed sent in .txt format
Recent queries
Search Add to builder Query Items found Time
#5 Add Search (#2 AND #3) 433 12:06:43
#4 Add Search (#1 AND #3) 387 12:04:49
#3 Add Search (vestibular diseases[mesh] OR vertigo[mesh] OR 254931 11:59:52
proprioception[mesh] OR accidental falls[mesh]
OR balance[tiab] OR dizziness[tiab] OR vertigo[tiab]
OR vestibular[tiab])
#2 Add Search (tai ji[mesh] OR “tai chi”[tiab] OR taiji[tiab] OR 1320 11:58:32
taijiquan[tiab] OR “t’ai chi”[tiab])
#1 Add Search (acupuncture therapy[mesh] OR acupuncture[tiab] 25266 11:57:28
OR meridians[tiab])
Huang et al.: Tai Chi and Balance Disorders 11
Downloaded from: https://pubs.asha.org Nannette Nicholson on 05/03/2019, Terms of Use: https://pubs.asha.org/pubs/rights_and_permissions
Appendix A ( p. 2 of 2)
Search Strategies 12/08/2016
CINAHL sent in RIS format
Search ID# Search terms Search options Last run via Results
S5 S2 AND S3 Limiters - Exclude MEDLINE records Interface - EBSCOhost Research Databases 79
Search modes - Boolean/Phrase Search Screen - Advanced Search
Database - CINAHL Complete
S4 S1 AND S3 Limiters - Exclude MEDLINE records Interface - EBSCOhost Research Databases 272
Search modes - Boolean/Phrase Search Screen - Advanced Search
Database - CINAHL Complete
S3 vestibular OR balance Search modes - Boolean/Phrase Interface - EBSCOhost Research Databases 58,857
OR vertigo OR dizzy Search Screen - Advanced Search
OR dizziness Database - CINAHL Complete
OR proprioception
OR “accidental falls”
S2 acupuncture OR meridians Search modes - Boolean/Phrase Interface - EBSCOhost Research Databases 13,166
Search Screen - Advanced Search
Database - CINAHL Complete
S1 “tai chi” OR “tai ji” OR Search modes - Boolean/Phrase Interface - EBSCOhost Research Databases 1,624
taiji OR taijiquan Search Screen - Advanced Search
Database - CINAHL Complete
PscyINFO sent in RIS format
Search ID# Search terms Search options Last run via Results
S5 S2 AND S3 Search modes - Boolean/Phrase Interface - EBSCOhost Research Databases 47
Search Screen - Advanced Search
Database - PsycINFO
S4 S1 AND S3 Search modes - Boolean/Phrase Interface - EBSCOhost Research Databases 126
Search Screen - Advanced Search
Database - PsycINFO
S3 vestibular OR balance Search modes - Boolean/Phrase Interface - EBSCOhost Research Databases 53,734
OR vertigo OR dizzy Search Screen - Advanced Search
OR dizziness OR Database - PsycINFO
proprioception OR
“accidental falls”
S2 acupuncture OR meridians Search modes - Boolean/Phrase Interface - EBSCOhost Research Databases 2,929
Search Screen - Advanced Search
Database - PsycINFO
S1 “tai chi” OR “tai ji” OR taiji Search modes - Boolean/Phrase Interface - EBSCOhost Research Databases 517
OR taijiquan Search Screen - Advanced Search
Database - PsycINFO
Web of Science
Set Results
#5 471 #3 AND #2
Indexes = SCI-EXPANDED, SSCI Timespan = All years
#4 796 #3 AND #1
Indexes = SCI-EXPANDED, SSCI Timespan = All years
#3 728,089 TOPIC: (vestibular OR vertigo OR balance OR dizzy OR dizziness
OR falls OR falling OR proprioception)
Indexes = SCI-EXPANDED, SSCI Timespan = All years
#2 19,462 TOPIC: (acupuncture OR meridians)
Indexes = SCI-EXPANDED, SSCI Timespan = All years
#1 1,914 TOPIC: (“tai chi” OR “tai ji” OR taiji OR taijiquan OR “t’ai chi”)
Indexes = SCI-EXPANDED, SSCI Timespan = All years
Sent in three files in BibTex format.
12 American Journal of Audiology • 1–14
Downloaded from: https://pubs.asha.org Nannette Nicholson on 05/03/2019, Terms of Use: https://pubs.asha.org/pubs/rights_and_permissions
Appendix B ( p. 1 of 2)
Study Review Form
Study title: ___________________________________________________________
Database: __________________Study Number______Reviewer_________________
(1) Study Screen Details
Screening Decision Screening Conclusion
Study Passes Screens ☐ Yes ☐ No Eligible for Review ☐ Yes ☐ No
(2) Study Design Details
GRADE Scores: ☐ High (at least 4) ☐ Moderate (3) ☐ Low (2) ☐ Very Low (1 or less)
Study Design: ☐ Randomized control trial ☐ One group pretest posttest design
☐ Pretest posttest design with a control group ☐ Posttest design ☐ Mixed Research
☐ Qualitative ☐ Other ________________________________________________
(3) Study Characteristics
Study Population ☐ Younger Population (< 65yo) ☐ Older Population (≥ 65yo)
Demographics Sample size_______ (M_______ F_______)
Mean Age_________
Vestibular Assessment ☐ VNG/ENG ☐ Rotary Chair ☐ MRI ☐ N/A
☐ Other: ________________________________________
Intervention Tai Chi
Duration________________________________________
Style___________________________________________
# of Movements__________________________________
☐ Modification: __________________________________
☐ Other: ________________________________________
Primary Outcome ☐ Static/Dynamic Balance ☐ Improved Mobility
☐ Improved Frequency and Severity of dizziness and vertigo
☐ Improved Gait and Postural Performance
☐ Other: ________________________________________
Secondary Outcome ☐ Gaze Stabilization ☐ Satisfaction ☐ Relaxation ☐ Calmness
☐ N/A
☐ Other: _______________________________________
Primary Outcome Measure ☐ Activities-Specific Balance Confidence Scale (ABC)
☐ Dynamic Gait Index (DGI) ☐ Clinical Exam
☐ Electromyography (EMG) ☐ Berg Balance Scale (BBS)
☐ Other: ______________________________________
Huang et al.: Tai Chi and Balance Disorders 13
Downloaded from: https://pubs.asha.org Nannette Nicholson on 05/03/2019, Terms of Use: https://pubs.asha.org/pubs/rights_and_permissions
Appendix B ( p. 2 of 2)
Study Review Form
GRADE Scoring System
Type of evidence
Initial score based on type of +4RCTs/ SR of RCTs, +/− other types of evidence
evidence +2Observational evidence (e.g., cohort, case-control)
Quality
Based on Blinding and allocation process
Follow-up and withdrawals
Sparse data
Other methodological concerns (e.g., incomplete reporting, subjective outcomes)
Score 0 No problems
−1Problem with 1 element
−2Problem with 2 elements
−3Problem with 3 or more elements
Consistency
Based on Degree of consistency of effect between or within studies
Score +1Evidence of dose response across or within studies (or inconsistency across studies is explained by a dose
response); also 1 point added if adjustment for confounders would have increased the effect size
0 All/most studies show similar results
−1Lack of agreement between studies (e.g., statistical heterogeneity between RCTs, conflicting results)
Directness
Based on The generalizability of population and outcomes from each study to our population of interest
Score 0 Population and outcomes broadly generalizable
−1Problem with 1 element
−2Problem with 2 or more elements
Effect size
Based on The reported OR/RR/HR for comparison
Score 0 Not all effect sizes > 2 or < 0.5 and significant; or if OR/RR/HR not significant
+1Effect size > 2 or < 0.5 for all studies/meta-analyses included in comparison and significant
+2Effect size > 5 or < 0.2 for all studies/meta-analyses included in comparison and significant
14 American Journal of Audiology • 1–14
Downloaded from: https://pubs.asha.org Nannette Nicholson on 05/03/2019, Terms of Use: https://pubs.asha.org/pubs/rights_and_permissions
View publication stats
Вам также может понравиться
- PRACTICAL RESEARCH 1 MIDTERM EXAM 2020 With AnswersДокумент3 страницыPRACTICAL RESEARCH 1 MIDTERM EXAM 2020 With AnswersMichelle Berme90% (39)
- Chi Square Problem With SolutionДокумент2 страницыChi Square Problem With SolutionSushant Viswakarma82% (33)
- Physiotherapy As An Initial Treatment Option For Femoroacetabular ImpingementДокумент9 страницPhysiotherapy As An Initial Treatment Option For Femoroacetabular ImpingementNicolas ParejaОценок пока нет
- E3023-15 Standard Practice For Probability of Detection Analysis For  Versus A DataДокумент12 страницE3023-15 Standard Practice For Probability of Detection Analysis For  Versus A DataAhmed Shaban KotbОценок пока нет
- The Effects of Qigong On Reducing Stress and Anxiety and Enhancing Body Mind Well BeingДокумент10 страницThe Effects of Qigong On Reducing Stress and Anxiety and Enhancing Body Mind Well BeingSamo JaОценок пока нет
- Motives To Practice Exercise in Old Age and Successful Aging - A Latent Class AnalysisДокумент7 страницMotives To Practice Exercise in Old Age and Successful Aging - A Latent Class AnalysisBryan NguyenОценок пока нет
- The Efficacy of Tai Chi Chuan in Physical Rehabilitation - A LiteДокумент25 страницThe Efficacy of Tai Chi Chuan in Physical Rehabilitation - A LiteKomang Tri Adi SuparwatiОценок пока нет
- 17 Kasimis Original 14 1Документ8 страниц17 Kasimis Original 14 1Maria Alejandra Garcia QuirogaОценок пока нет
- A Randomized Controlled Trial of 8-Form Tai Chi Improves Symptoms and Functional Mobility in Fibromyalgia PatientsДокумент10 страницA Randomized Controlled Trial of 8-Form Tai Chi Improves Symptoms and Functional Mobility in Fibromyalgia Patientsnadia kurniaОценок пока нет
- Effectiveness of Tai Chi Exercise On Overall Quality of LifeДокумент7 страницEffectiveness of Tai Chi Exercise On Overall Quality of LifeAndreRicardoCPОценок пока нет
- Dafpus 11Документ9 страницDafpus 11Cut MulianiОценок пока нет
- 1 Tai Chi and Rheumatic DiseasesДокумент14 страниц1 Tai Chi and Rheumatic DiseasescinborbОценок пока нет
- Does Tai Chi/Qi Gong Help Patients With Multiple Sclerosis?: N. Mills, J. Allen, S. Carey MorganДокумент10 страницDoes Tai Chi/Qi Gong Help Patients With Multiple Sclerosis?: N. Mills, J. Allen, S. Carey MorganZoli ZolikaОценок пока нет
- Document PDFДокумент7 страницDocument PDFPricess PoppyОценок пока нет
- S Nie Scho SCHW 2005 Psychology HealthДокумент19 страницS Nie Scho SCHW 2005 Psychology HealthJip van AmerongenОценок пока нет
- Out 175Документ7 страницOut 175Anonymous 75TDy2yОценок пока нет
- Stubbs Et Al 2014 PRIДокумент9 страницStubbs Et Al 2014 PRIHenry WijayaОценок пока нет
- Barriers To Physical Activity in Older Adult PDFДокумент26 страницBarriers To Physical Activity in Older Adult PDFJhoana Rose Joaquin SantosОценок пока нет
- Running Head: EXERCISE AND HEALTH 1Документ12 страницRunning Head: EXERCISE AND HEALTH 1api-281674546Оценок пока нет
- 18 Bicer Original 10 1Документ8 страниц18 Bicer Original 10 1Nurul HafizaОценок пока нет
- Bio Mechanics of Tai Chi - A ReviewДокумент13 страницBio Mechanics of Tai Chi - A Reviewjopepinho5796Оценок пока нет
- Journal of Bodywork & Movement TherapiesДокумент11 страницJournal of Bodywork & Movement TherapiesJorge GámezОценок пока нет
- Evidence-Based Nursing Practice For Health Promotion in Adults With Hypertension: A Literature ReviewДокумент38 страницEvidence-Based Nursing Practice For Health Promotion in Adults With Hypertension: A Literature Reviewmarisa isahОценок пока нет
- Evidence-Based Nursing Practice For Health Promotion in Adults With Hypertension: A Literature ReviewДокумент19 страницEvidence-Based Nursing Practice For Health Promotion in Adults With Hypertension: A Literature ReviewYusvita WaliaОценок пока нет
- Medi 99 E21805Документ8 страницMedi 99 E21805Ayu AnandahОценок пока нет
- Artikel 2 - Music - Movement - Theraphy - Stroke - IskemikДокумент10 страницArtikel 2 - Music - Movement - Theraphy - Stroke - Iskemikselamat parminОценок пока нет
- Treatment-Related Fatigue and Exercise in Patients With Cancer A Systematic ReviewДокумент19 страницTreatment-Related Fatigue and Exercise in Patients With Cancer A Systematic ReviewtiagobcsОценок пока нет
- Art 24832 PDFДокумент9 страницArt 24832 PDFDheaDesniaОценок пока нет
- Ansiedade Top PDFДокумент11 страницAnsiedade Top PDFPaulo AfonsoОценок пока нет
- ArtikelДокумент8 страницArtikelAmelina RistiОценок пока нет
- Ward 2017Документ9 страницWard 2017Anonymous YjjV5izD1Оценок пока нет
- J JBMT 2019 05 013Документ7 страницJ JBMT 2019 05 013ankitaghivareОценок пока нет
- 后期的心理防线Документ10 страниц后期的心理防线zyzzyzОценок пока нет
- Qi Gong Quality Life in TaiwanДокумент6 страницQi Gong Quality Life in TaiwanpenfoОценок пока нет
- Neuropsychologia: Nancy Byl, Wenlong Zhang, Sophia Coo, Masayoshi TomizukaДокумент12 страницNeuropsychologia: Nancy Byl, Wenlong Zhang, Sophia Coo, Masayoshi TomizukaMariachiaraRicciОценок пока нет
- 6 Cheng2017Документ7 страниц6 Cheng2017Sergio Machado NeurocientistaОценок пока нет
- Asian Nursing Research: Seung-Joo Lim, PHD, RN, Chunmi Kim, PHD, RNДокумент7 страницAsian Nursing Research: Seung-Joo Lim, PHD, RN, Chunmi Kim, PHD, RNmelisaОценок пока нет
- Artrite e Exercício, Revisão PDFДокумент11 страницArtrite e Exercício, Revisão PDFFabianinhoLacerdaОценок пока нет
- Choi2017 The Effects of Floor-Seated ExerciseДокумент6 страницChoi2017 The Effects of Floor-Seated ExerciseFaizul HasanОценок пока нет
- Environmental Barriers and Social Participation inДокумент19 страницEnvironmental Barriers and Social Participation inSantiago QuintanaОценок пока нет
- Tung 2009 Coping, Anxiety and Quality of Life After CABGДокумент14 страницTung 2009 Coping, Anxiety and Quality of Life After CABGandreautumn66Оценок пока нет
- Archives of Psychiatric Nursing: Guichen Li, Hua Yuan, Wei ZhangДокумент8 страницArchives of Psychiatric Nursing: Guichen Li, Hua Yuan, Wei Zhangdies setyoningsihОценок пока нет
- (ART. 5 PP DEPORTE) Tratamiento de Terapia Manual para La Escoliosis Idiopática AdolescenteДокумент5 страниц(ART. 5 PP DEPORTE) Tratamiento de Terapia Manual para La Escoliosis Idiopática AdolescenteSofia PaezОценок пока нет
- Hall Vestibular Rehab CPGJNPT2016Документ33 страницыHall Vestibular Rehab CPGJNPT2016Zoheir RamdaneОценок пока нет
- The Effects of Exercise Standards On The Quality of Life To People With Chronic DiseaseДокумент18 страницThe Effects of Exercise Standards On The Quality of Life To People With Chronic DiseaseMario LanzaОценок пока нет
- Wong Et Al-2017-European Journal of PainДокумент16 страницWong Et Al-2017-European Journal of PainEduardo BarreraОценок пока нет
- Physical Therapy in Down Syndrome: Systematic Review and Meta-AnalysisДокумент27 страницPhysical Therapy in Down Syndrome: Systematic Review and Meta-AnalysisFranciel StuelpОценок пока нет
- BMC Musculoskeletal Disorders: Fatigue in Osteoarthritis: A Qualitative StudyДокумент8 страницBMC Musculoskeletal Disorders: Fatigue in Osteoarthritis: A Qualitative StudyElvis Ponce AbarcaОценок пока нет
- Journal Pre-Proof: Clinical BiomechanicsДокумент20 страницJournal Pre-Proof: Clinical BiomechanicsAanggi JiihanОценок пока нет
- Physical Therapy in Sport: Caitlin E. George, Luke J. Heales, Robert Stanton, Sally-Anne Wintour, Crystal O. KeanДокумент11 страницPhysical Therapy in Sport: Caitlin E. George, Luke J. Heales, Robert Stanton, Sally-Anne Wintour, Crystal O. KeanDaniel GuevaraОценок пока нет
- Body Concerns Ex Behaviour PaperДокумент16 страницBody Concerns Ex Behaviour PaperMohit KharbandaОценок пока нет
- Contemporary Clinical Trials: Contents Lists Available atДокумент14 страницContemporary Clinical Trials: Contents Lists Available atChofi SaezОценок пока нет
- Yoga and AxietyДокумент14 страницYoga and AxietyLie LhianzaОценок пока нет
- Aldwin Park 2004 Coping and Physical Health OutcomesДокумент6 страницAldwin Park 2004 Coping and Physical Health OutcomespanospanОценок пока нет
- Therapeutic Benefits of Tai Chi Exercise: Research Review: Wisconsin Medical JournalДокумент6 страницTherapeutic Benefits of Tai Chi Exercise: Research Review: Wisconsin Medical JournalJuanОценок пока нет
- Aerobic ExerciseДокумент9 страницAerobic Exercisebiahonda15Оценок пока нет
- Archives of Gerontology and GeriatricsДокумент7 страницArchives of Gerontology and GeriatricssyifaОценок пока нет
- Vestibular CPG JNPT 2016 FinalДокумент33 страницыVestibular CPG JNPT 2016 FinalMairaОценок пока нет
- Effect of Whole Body Vibration On Sterotypy of Young Children WitДокумент28 страницEffect of Whole Body Vibration On Sterotypy of Young Children WitRandy RylieОценок пока нет
- Critical Appraisal - Research and Evidence: Maisie Sheahan (21215414)Документ5 страницCritical Appraisal - Research and Evidence: Maisie Sheahan (21215414)Jan MackeyОценок пока нет
- Zhang 2021Документ8 страницZhang 2021iovanelena235Оценок пока нет
- Physiotherapy For Patients With Sciatica Awaiting Lumbar Micro-Discectomy Surgery - A Nested, Qualitative Study of Patients' Views and ExperiencesДокумент10 страницPhysiotherapy For Patients With Sciatica Awaiting Lumbar Micro-Discectomy Surgery - A Nested, Qualitative Study of Patients' Views and ExperiencesLindapratama SaifuddinОценок пока нет
- Correlational Research - Definition With Examples - QuestionProДокумент5 страницCorrelational Research - Definition With Examples - QuestionProMikaela SamonteОценок пока нет
- Ismail Et Al - Pilot Study Does It Really MatterДокумент18 страницIsmail Et Al - Pilot Study Does It Really MatterRoy Morales PérezОценок пока нет
- Chapter I: The Problem and Its BackgroundДокумент3 страницыChapter I: The Problem and Its BackgroundRolando E. CaserОценок пока нет
- Meta AnalysisДокумент33 страницыMeta AnalysissiawОценок пока нет
- Chapter 1-Introduction To Non-Parametric StatisticsДокумент10 страницChapter 1-Introduction To Non-Parametric StatisticsMarben OrogoОценок пока нет
- Business Research MethodsДокумент8 страницBusiness Research MethodsAthul MukundОценок пока нет
- Week 10 - Data Analysis, Interpretation and PresentationДокумент20 страницWeek 10 - Data Analysis, Interpretation and PresentationRaymond RamirezОценок пока нет
- What Are Different Research Approaches? Comprehensive Review of Qualitative, Quantitative, and Mixed Method Research, Their Applications, Types, and LimitationsДокумент11 страницWhat Are Different Research Approaches? Comprehensive Review of Qualitative, Quantitative, and Mixed Method Research, Their Applications, Types, and LimitationsHamed TaherdoostОценок пока нет
- Doctoral Summer School 2018-IIMA-BrochureДокумент2 страницыDoctoral Summer School 2018-IIMA-BrochurerahulОценок пока нет
- Practical Research 2 Unit PlanДокумент37 страницPractical Research 2 Unit Planmichael sto domingo100% (1)
- JBI Critical Appraisal Checklist For Quasi-Experimental Studies (Non-Randomized Experimental Studies)Документ2 страницыJBI Critical Appraisal Checklist For Quasi-Experimental Studies (Non-Randomized Experimental Studies)Angga saputraОценок пока нет
- Dr. Kofi Agyarko Ababio: Math 353: StatisticsДокумент23 страницыDr. Kofi Agyarko Ababio: Math 353: StatisticsReagan TorbiОценок пока нет
- Chapter1 - Statistics For Managerial DecisionsДокумент26 страницChapter1 - Statistics For Managerial DecisionsRanjan Raj UrsОценок пока нет
- NENDHE PRAVIGA/180511625510 T-TestДокумент3 страницыNENDHE PRAVIGA/180511625510 T-TestVicky AndikaОценок пока нет
- Research Design: Presented By:-Nitul Jyoti Das. PGDM 2 Sem. Sec - A Roll No - 8Документ12 страницResearch Design: Presented By:-Nitul Jyoti Das. PGDM 2 Sem. Sec - A Roll No - 8Nitul Jyoti DasОценок пока нет
- 002 - 1203 - Ni Wayan Ari Anindita Sari - GalleyДокумент5 страниц002 - 1203 - Ni Wayan Ari Anindita Sari - GalleyHaningtyas IndahОценок пока нет
- Second Quarter Examination in Practical Research 2 - Grade 12Документ3 страницыSecond Quarter Examination in Practical Research 2 - Grade 12Christine ConlasОценок пока нет
- Augmented Dickey-Fuller Test - WikipediaДокумент4 страницыAugmented Dickey-Fuller Test - WikipediapaulicalejerОценок пока нет
- Laboratory Exercise 3Документ6 страницLaboratory Exercise 3Berna ChiiОценок пока нет
- Interpretasi Hasil SpssДокумент2 страницыInterpretasi Hasil SpssMeilia JayantiОценок пока нет
- Different Types of QuestionnaireДокумент7 страницDifferent Types of QuestionnaireAnindya Champati100% (2)
- InterviewДокумент2 страницыInterviewt3xxaОценок пока нет
- Downloadable Test Bank For Research Methods in Psychology 10th Edition ShaughnessyДокумент31 страницаDownloadable Test Bank For Research Methods in Psychology 10th Edition Shaughnessytinawatsontzrjoiqbws100% (23)
- Thesis StudyДокумент2 страницыThesis StudysariОценок пока нет
- Mann Whitney TestДокумент16 страницMann Whitney TestLayan MohammadОценок пока нет
- HHS Public Access: Characteristics of Qualitative Descriptive Studies: A Systematic ReviewДокумент24 страницыHHS Public Access: Characteristics of Qualitative Descriptive Studies: A Systematic ReviewDhiina ADrianaОценок пока нет
- ID Pengaruh Kualitas Pelayanan Terhadap Kepuasan Pelanggan Pada PT Pos Indonesia PeДокумент10 страницID Pengaruh Kualitas Pelayanan Terhadap Kepuasan Pelanggan Pada PT Pos Indonesia PeRudy Even NaibahoОценок пока нет