Вам также может понравиться
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- Tokyo Ghoul Zakki Helvetica ScansДокумент86 страницTokyo Ghoul Zakki Helvetica ScansReza Ishak Estiko50% (4)
- CONSORT 2010 ChecklistДокумент2 страницыCONSORT 2010 ChecklistReza Ishak EstikoОценок пока нет
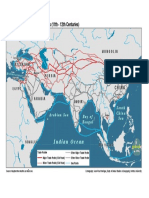
- The Silk Road and Arab Sea Routes (11th - 12th Centuries) : Indian OceanДокумент1 страницаThe Silk Road and Arab Sea Routes (11th - 12th Centuries) : Indian OceanReza Ishak EstikoОценок пока нет
- Treatment of Coronary In-Stent Restenosis With A Paclitaxel-Coated Balloon CatheterДокумент12 страницTreatment of Coronary In-Stent Restenosis With A Paclitaxel-Coated Balloon CatheterReza Ishak EstikoОценок пока нет
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (400)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- Eu GMP Annex 15 PDFДокумент2 страницыEu GMP Annex 15 PDFBrian0% (1)
- Yesenia Jimenez: ObjectiveДокумент3 страницыYesenia Jimenez: Objectivetyson chavezОценок пока нет
- Case Summaries - Contract Law Unit 1Документ10 страницCase Summaries - Contract Law Unit 1Laura HawkinsОценок пока нет
- Complete Products ListДокумент13 страницComplete Products ListHina TinaОценок пока нет
- Administering An Intramuscular InjectionДокумент3 страницыAdministering An Intramuscular Injectionapi-26570979100% (4)
- 1.e. Bronchiolitis Treatment & Management - Approach Considerations, Initial Management, Admission CriteriaДокумент12 страниц1.e. Bronchiolitis Treatment & Management - Approach Considerations, Initial Management, Admission CriteriaDavid CraigОценок пока нет
- Microencapsulation PDFДокумент21 страницаMicroencapsulation PDFSwati SharmaОценок пока нет
- PN M189 Pharma Analyzer EN PDFДокумент2 страницыPN M189 Pharma Analyzer EN PDFSerhiyОценок пока нет
- BD of Medicines PDFДокумент9 страницBD of Medicines PDFgauharОценок пока нет
- Research Journal of Pharmaceutical, Biological and Chemical SciencesДокумент5 страницResearch Journal of Pharmaceutical, Biological and Chemical SciencesDessy Erlyani Mugita SariОценок пока нет
- 1.normal Parameters For Pediatric AnesthesiaДокумент5 страниц1.normal Parameters For Pediatric AnesthesiaismailcemОценок пока нет
- Paediatric Emergency Drug DosesДокумент1 страницаPaediatric Emergency Drug DosesGloriaaaОценок пока нет
- Pharmacological Rationale For The Treatment of Chronic UrticariaДокумент10 страницPharmacological Rationale For The Treatment of Chronic Urticariaseptian88_cahyoОценок пока нет
- Manual of Pediatric Emergency MedicineДокумент28 страницManual of Pediatric Emergency MedicineRabi Dhakal100% (2)
- Phenylbutazone Review-Dr. Lawrence R. SomaДокумент12 страницPhenylbutazone Review-Dr. Lawrence R. SomaAndi Ade NurqalbiОценок пока нет
- Mesna: Mesna, Sold Under The BrandДокумент17 страницMesna: Mesna, Sold Under The BrandAndry HamdaniОценок пока нет
- Actinomicetos PDFДокумент15 страницActinomicetos PDFFredy AscuntarОценок пока нет
- A Systematic Review of Recently Reported Marine Derived Natural Product Kinase InhibitorsДокумент38 страницA Systematic Review of Recently Reported Marine Derived Natural Product Kinase InhibitorsIgnacio Pérez-VictoriaОценок пока нет
- List Harga Quantum UpdateДокумент1 страницаList Harga Quantum UpdateAde IrawanОценок пока нет
- Group3 ElementsДокумент7 страницGroup3 ElementsPeter JimenezОценок пока нет
- JPM 2018 Biotech OutlookДокумент92 страницыJPM 2018 Biotech Outlookaaquibnasir100% (1)
- 27 3 2014 - MWDДокумент26 страниц27 3 2014 - MWDTheMyawadyDailyОценок пока нет
- DDS LEC - Tablets Part 2Документ5 страницDDS LEC - Tablets Part 2kapeОценок пока нет
- A Review On Ethnopharmacolgy, Phytochemistry and Bioactivity of LeonotisДокумент4 страницыA Review On Ethnopharmacolgy, Phytochemistry and Bioactivity of LeonotisAnonymous HBRjaTX5YFОценок пока нет
- Role of Salvestrols in The Treatment of CancerДокумент10 страницRole of Salvestrols in The Treatment of CancerRaghu RamanОценок пока нет
- 1.2.1.1 - Overview of Clinical Trials in Canada - Tanya Ramsamy - eДокумент25 страниц1.2.1.1 - Overview of Clinical Trials in Canada - Tanya Ramsamy - ecristofer BellidoОценок пока нет
- Thesis - Shellac Film StabilityДокумент181 страницаThesis - Shellac Film StabilitySatish VaidyaОценок пока нет
- Chemotherapeutic Agents and AntiinfectivesДокумент64 страницыChemotherapeutic Agents and AntiinfectivesAnthony RiggsОценок пока нет
- Management of Severe Hyperkalemia PDFДокумент6 страницManagement of Severe Hyperkalemia PDFCarlos Navarro YslaОценок пока нет
- Close Loop Medication ManagementДокумент25 страницClose Loop Medication Managementfathul jannahОценок пока нет