Вам также может понравиться
- SPH 481 PolicybackgroundДокумент5 страницSPH 481 Policybackgroundapi-436879680Оценок пока нет
- Curriculum Draft 1Документ9 страницCurriculum Draft 1api-436879680Оценок пока нет
- Research Proposal 1Документ4 страницыResearch Proposal 1api-436879680Оценок пока нет
- Formal Research Protocol 1Документ3 страницыFormal Research Protocol 1api-436879680Оценок пока нет
- Paper 2 3Документ8 страницPaper 2 3api-436879680Оценок пока нет
- Honors 392 FinalpaperДокумент8 страницHonors 392 Finalpaperapi-436879680Оценок пока нет
- Individual Project 2 1Документ4 страницыIndividual Project 2 1api-436879680Оценок пока нет
- Final Research ReportДокумент10 страницFinal Research Reportapi-436879680Оценок пока нет
- Individual Project 1 4Документ4 страницыIndividual Project 1 4api-436879680Оценок пока нет
- Serotonin Toxicity Planning 3Документ7 страницSerotonin Toxicity Planning 3api-436879680Оценок пока нет
- March 28thДокумент27 страницMarch 28thapi-436879680Оценок пока нет
- sph480 SurveyДокумент8 страницsph480 Surveyapi-436879680Оценок пока нет
- Lobby Day MaterialsДокумент5 страницLobby Day Materialsapi-436879680Оценок пока нет
- Campus RacismДокумент21 страницаCampus Racismapi-436879680Оценок пока нет
- Nguyenkosmanrwittylcoe 2 Report 210309Документ17 страницNguyenkosmanrwittylcoe 2 Report 210309api-436879680Оценок пока нет
- Experential Learning Reflection 1Документ1 страницаExperential Learning Reflection 1api-436879680Оценок пока нет
- Loawittylcoe1report210204 3Документ8 страницLoawittylcoe1report210204 3api-436879680Оценок пока нет
- Population Health RapeДокумент28 страницPopulation Health Rapeapi-436879680Оценок пока нет
- Reflection 2Документ2 страницыReflection 2api-436879680Оценок пока нет
- SPH 380 OpedДокумент5 страницSPH 380 Opedapi-436879680Оценок пока нет
- GametheoryfinaldraftДокумент9 страницGametheoryfinaldraftapi-436879680Оценок пока нет
- Maternal Health Honors 391Документ21 страницаMaternal Health Honors 391api-436879680Оценок пока нет
- Costa Rica Final ProjectДокумент6 страницCosta Rica Final Projectapi-436879680Оценок пока нет
- ForeignpolicymemoДокумент14 страницForeignpolicymemoapi-436879680Оценок пока нет
- Costa Rica Final ProjectДокумент6 страницCosta Rica Final Projectapi-436879680Оценок пока нет
- Autumn Reflection and PortfolioДокумент2 страницыAutumn Reflection and Portfolioapi-436879680Оценок пока нет
- Autumn Reflection and PortfolioДокумент2 страницыAutumn Reflection and Portfolioapi-436879680Оценок пока нет
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5783)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (890)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (399)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (344)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (119)
- Microbiology and Immunology Pokhara University Syllabus NOCДокумент2 страницыMicrobiology and Immunology Pokhara University Syllabus NOCDinesh SubediОценок пока нет
- Health 8 Quarter 1Документ10 страницHealth 8 Quarter 1jayaaron.reyes.cОценок пока нет
- Educational Program To Prevent Foodborne Diseases at Restaurants of Suez Canal UniversityДокумент138 страницEducational Program To Prevent Foodborne Diseases at Restaurants of Suez Canal UniversityAmalElnawasanyОценок пока нет
- What Are Koch's Postulates?Документ3 страницыWhat Are Koch's Postulates?Cacamo Rexell-anОценок пока нет
- Communicable DiseaseДокумент9 страницCommunicable DiseaseSusan HepziОценок пока нет
- GDC Inmate HandbookДокумент71 страницаGDC Inmate Handbookachey240Оценок пока нет
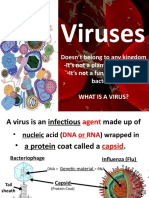
- Virus Vs Cells Notes PPT IPCДокумент33 страницыVirus Vs Cells Notes PPT IPCJulia NepoОценок пока нет
- Statement of Purpose (1) - 1Документ3 страницыStatement of Purpose (1) - 1Anitta ThomasОценок пока нет
- HLTINF006 Student Assessment Task 1Документ10 страницHLTINF006 Student Assessment Task 1Rebeca RaducuОценок пока нет
- Cp-Entomology Part 2Документ165 страницCp-Entomology Part 2RAFTITTI IncОценок пока нет
- Communicable Diseases Lecture 32 Pages Pg. 567 597Документ32 страницыCommunicable Diseases Lecture 32 Pages Pg. 567 597ShiraishiОценок пока нет
- Microbiology and ParasitologyДокумент14 страницMicrobiology and ParasitologyLleana TanОценок пока нет
- Laboratory Activity No. 2Документ10 страницLaboratory Activity No. 2neilandreiruba1011Оценок пока нет
- Microbes in Human WelfareДокумент8 страницMicrobes in Human WelfareSanjaya SahooОценок пока нет
- HandSC Level 2 Textbook Sample Chapters PDFДокумент26 страницHandSC Level 2 Textbook Sample Chapters PDFLiza GomezОценок пока нет
- Sutton Colloidal SilverДокумент44 страницыSutton Colloidal SilverJames Chapel100% (3)
- A Brief History of MicrobiologyДокумент5 страницA Brief History of MicrobiologyElaizaОценок пока нет
- E. Coli-JM101 ReportДокумент23 страницыE. Coli-JM101 ReportPosters SACОценок пока нет
- 2022病蟲害防治正課 (病害一)Документ118 страниц2022病蟲害防治正課 (病害一)Fran YОценок пока нет
- Microbial Pathogenesis: Amin - Bakir@hmu - Edu.krdДокумент16 страницMicrobial Pathogenesis: Amin - Bakir@hmu - Edu.krdAsma Muhammed majeedОценок пока нет
- Evolution and Ecology of Plant VirusesДокумент13 страницEvolution and Ecology of Plant VirusesBarakОценок пока нет
- Ch. 25 Body Defence MechanismsДокумент34 страницыCh. 25 Body Defence Mechanisms吴昊Оценок пока нет
- Evolution of Human Diseases - HO Smail PDFДокумент17 страницEvolution of Human Diseases - HO Smail PDFdoeditОценок пока нет
- Jurnal Sanitasi 2Документ9 страницJurnal Sanitasi 2herlianiОценок пока нет
- Music: Direction: Read The Questions Carefully. Write The Letters of The Correct AnswerДокумент3 страницыMusic: Direction: Read The Questions Carefully. Write The Letters of The Correct AnswerDianne S. GarciaОценок пока нет
- Microbiology Related Thesis TopicsДокумент7 страницMicrobiology Related Thesis Topicsjensantiagosyracuse100% (2)
- ATS Guidelines for Managing Community-Acquired PneumoniaДокумент25 страницATS Guidelines for Managing Community-Acquired PneumoniaMeme BuletОценок пока нет
- How To Grow Your Own SHTF PharmacyДокумент23 страницыHow To Grow Your Own SHTF PharmacyLes BennettОценок пока нет
- Practical Raptor Nutrition Neil Forbes PDFДокумент9 страницPractical Raptor Nutrition Neil Forbes PDFWisnu JuliastitoОценок пока нет