Вам также может понравиться
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- JBC 12 36Документ4 страницыJBC 12 36cut normaya putriОценок пока нет
- MTPC I4 21 - e CertificateДокумент1 страницаMTPC I4 21 - e Certificatecut normaya putriОценок пока нет
- 19-11 Pneumonia, WPD, Online PDFДокумент62 страницы19-11 Pneumonia, WPD, Online PDFcut normaya putriОценок пока нет
- Infodatin Pengelolaan Vaksin Di IndonesiaДокумент12 страницInfodatin Pengelolaan Vaksin Di IndonesiaChristina AgustinОценок пока нет
- 19-11 Pneumonia, WPD, Online PDFДокумент62 страницы19-11 Pneumonia, WPD, Online PDFcut normaya putriОценок пока нет
- ACLS NotesДокумент45 страницACLS Notescut normaya putriОценок пока нет
- Journal of Clinical Gastroenterology and Treatment JCGT 3 042Документ9 страницJournal of Clinical Gastroenterology and Treatment JCGT 3 042Loise MayasariОценок пока нет
- Sala Vast Ru 2017Документ6 страницSala Vast Ru 2017Muhammad AmrullahОценок пока нет
- 19-11 Pneumonia, WPD, Online PDFДокумент62 страницы19-11 Pneumonia, WPD, Online PDFcut normaya putriОценок пока нет
- Scabies Treatment in Children: A Narrative ReviewДокумент8 страницScabies Treatment in Children: A Narrative Reviewcut normaya putriОценок пока нет
- Journal of Clinical Gastroenterology and Treatment JCGT 3 042Документ9 страницJournal of Clinical Gastroenterology and Treatment JCGT 3 042cut normaya putriОценок пока нет
- Ca MammeДокумент5 страницCa MammeI Nengah Aditya PramanaОценок пока нет
- Prevalence and Risk Factors of Hemorrhoids: A Study in A Semi-Urban CentreДокумент4 страницыPrevalence and Risk Factors of Hemorrhoids: A Study in A Semi-Urban CentreNaily Nuzulur RohmahОценок пока нет
- Prevalence and Risk Factors of Hemorrhoids: A Study in A Semi-Urban CentreДокумент4 страницыPrevalence and Risk Factors of Hemorrhoids: A Study in A Semi-Urban CentreNaily Nuzulur RohmahОценок пока нет
- Jurnal Hernia PDFДокумент8 страницJurnal Hernia PDFagungratihsdОценок пока нет
- Sala Vast Ru 2017Документ6 страницSala Vast Ru 2017Muhammad AmrullahОценок пока нет
- KJCCM 2016 00969Документ13 страницKJCCM 2016 00969nurulanisa0703Оценок пока нет
- Spinal Chordoma: Radiologic Features: in 14 CasesДокумент3 страницыSpinal Chordoma: Radiologic Features: in 14 Casescut normaya putriОценок пока нет
- Sala Vast Ru 2017Документ6 страницSala Vast Ru 2017Muhammad AmrullahОценок пока нет
- Scabies Treatment in Children: A Narrative ReviewДокумент8 страницScabies Treatment in Children: A Narrative Reviewcut normaya putriОценок пока нет
- Ca MammeДокумент5 страницCa MammeI Nengah Aditya PramanaОценок пока нет
- Heart Attack MedicationДокумент24 страницыHeart Attack Medicationcut normaya putriОценок пока нет
- AJR.06.0651) Choudhary, Arabinda K. Donnelly, Lane F. Racadio, Judy M. STR - Diseases Associated With Childhood Obesity PDFДокумент13 страницAJR.06.0651) Choudhary, Arabinda K. Donnelly, Lane F. Racadio, Judy M. STR - Diseases Associated With Childhood Obesity PDFcut normaya putriОценок пока нет
- Calcagno 2018Документ10 страницCalcagno 2018cut normaya putriОценок пока нет
- s13017 018 0179 0Документ10 страницs13017 018 0179 0cut normaya putriОценок пока нет
- KJCCM 2016 00969Документ13 страницKJCCM 2016 00969nurulanisa0703Оценок пока нет
- Prevalence and Risk Factors of Hemorrhoids: A Study in A Semi-Urban CentreДокумент4 страницыPrevalence and Risk Factors of Hemorrhoids: A Study in A Semi-Urban CentreNaily Nuzulur RohmahОценок пока нет
- Journal of Clinical Gastroenterology and Treatment JCGT 3 042Документ9 страницJournal of Clinical Gastroenterology and Treatment JCGT 3 042Loise MayasariОценок пока нет
- Journal of Clinical Gastroenterology and Treatment JCGT 3 042Документ9 страницJournal of Clinical Gastroenterology and Treatment JCGT 3 042cut normaya putriОценок пока нет
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (344)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (399)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (120)
- Full Download Test Bank For Cognitive Psychology 6th Edition Sternberg PDF Full ChapterДокумент31 страницаFull Download Test Bank For Cognitive Psychology 6th Edition Sternberg PDF Full Chaptercadie.tutressrwwsn100% (15)
- Intro To Lockpicking and Key Bumping WWДокумент72 страницыIntro To Lockpicking and Key Bumping WWapi-3777781100% (8)
- Configuration of VIO On Power6 PDFДокумент39 страницConfiguration of VIO On Power6 PDFchengabОценок пока нет
- An Expert Guide To SQL Server Performance Tuning PDFДокумент10 страницAn Expert Guide To SQL Server Performance Tuning PDFMarioОценок пока нет
- TRUE OR FALSE. Write TRUE If The Statement Is True and Write FALSE If The Statement Is FalseДокумент2 страницыTRUE OR FALSE. Write TRUE If The Statement Is True and Write FALSE If The Statement Is FalseBea Clarence IgnacioОценок пока нет
- Facts:: Villarosa, Joan Cristine 2015-1635Документ3 страницыFacts:: Villarosa, Joan Cristine 2015-1635Tin VillarosaОценок пока нет
- Ami Aptio Afu User Guide NdaДокумент32 страницыAmi Aptio Afu User Guide NdaMarcoОценок пока нет
- Squatting Problem and Its Social Ills in MANILAДокумент10 страницSquatting Problem and Its Social Ills in MANILARonstar Molina TanateОценок пока нет
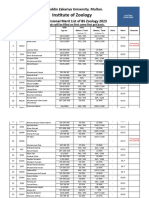
- 5953-6th Merit List BS Zool 31-8-2023Документ22 страницы5953-6th Merit List BS Zool 31-8-2023Muhammad AttiqОценок пока нет
- Historical Background of The PNPДокумент1 страницаHistorical Background of The PNPGloria AsuncionОценок пока нет
- Ikyase & Olisah (2014)Документ8 страницIkyase & Olisah (2014)Dina FitrianiОценок пока нет
- National Police Commission: Interior and Local Government Act of 1990" As Amended by Republic Act No. 8551Документ44 страницыNational Police Commission: Interior and Local Government Act of 1990" As Amended by Republic Act No. 8551April Elenor Juco100% (1)
- 3.1 Geographical Extent of The Foreign Exchange MarketДокумент8 страниц3.1 Geographical Extent of The Foreign Exchange MarketSharad BhorОценок пока нет
- Original PDF Accounting For Corporate Combinations and Associations 8th PDFДокумент42 страницыOriginal PDF Accounting For Corporate Combinations and Associations 8th PDFmarth.fuller529100% (41)
- Demand Letter WiwiДокумент1 страницаDemand Letter WiwiflippinturtleОценок пока нет
- Motor Insurance - Proposal Form Cum Transcript Letter For Miscellaneous Carrying ComprehensiveДокумент2 страницыMotor Insurance - Proposal Form Cum Transcript Letter For Miscellaneous Carrying ComprehensiveSantosh JaiswalОценок пока нет
- Concept Note ALACДокумент4 страницыConcept Note ALACdheereshkdwivediОценок пока нет
- Pulseelectronicsnetwork Jk08001nl Pcndesignspecification 2926Документ3 страницыPulseelectronicsnetwork Jk08001nl Pcndesignspecification 2926Guilherme NevesОценок пока нет
- JIGL-Chapter5 (Administrative Law)Документ21 страницаJIGL-Chapter5 (Administrative Law)KHUSHBOO SHARMAОценок пока нет
- Platform1 Server and HIO Configuration Guide V1.01Документ40 страницPlatform1 Server and HIO Configuration Guide V1.01sirengeniusОценок пока нет
- KUK - PH D Admission Advertisement 2012Документ1 страницаKUK - PH D Admission Advertisement 2012nareshjangra397Оценок пока нет
- Sample QP 1 Jan2020Документ19 страницSample QP 1 Jan2020M Rafeeq100% (1)
- Recio Garcia V Recio (Digest)Документ3 страницыRecio Garcia V Recio (Digest)Aljenneth MicallerОценок пока нет
- Work Policy 2016Документ57 страницWork Policy 2016siddhartha bhattacharyyaОценок пока нет
- 2021 TaxReturnДокумент11 страниц2021 TaxReturnHa AlОценок пока нет
- Mr. Saxena - Reply To DV MatterДокумент11 страницMr. Saxena - Reply To DV MatterYash SampatОценок пока нет
- Villareal vs. PeopleДокумент11 страницVillareal vs. PeopleJan Carlo SanchezОценок пока нет
- Bookkeeping Exercises 2022Документ6 страницBookkeeping Exercises 2022Anne de GuzmanОценок пока нет
- Chordu Piano Chords Ede Lobas Chordsheet Id - JBQiUlO0NDU PDFДокумент3 страницыChordu Piano Chords Ede Lobas Chordsheet Id - JBQiUlO0NDU PDFKaren RochaОценок пока нет