Вам также может понравиться
- Sample Write UpДокумент2 страницыSample Write UpNar Patrick Padilla100% (1)
- Acute Appendicitis: Surgical PostingДокумент8 страницAcute Appendicitis: Surgical PostingGraldoОценок пока нет
- Case Write Up 1-CholecystitisДокумент9 страницCase Write Up 1-CholecystitisAmbhi Gana100% (1)
- H&P For ScriptДокумент12 страницH&P For ScriptAlina KievskyОценок пока нет
- Otoscopy and Tympanometry Skill RefresherДокумент60 страницOtoscopy and Tympanometry Skill RefreshersmexiiloriОценок пока нет
- Unit 3 & Unit 4Документ8 страницUnit 3 & Unit 4Melania Arliana MeoОценок пока нет
- History Taking Template For StudentsДокумент14 страницHistory Taking Template For Studentsx88tydcwb2Оценок пока нет
- CPC CaseДокумент8 страницCPC CasePingky khingthongОценок пока нет
- Case-Presention FinalДокумент16 страницCase-Presention Finalkristine-ann TabernaОценок пока нет
- IVMS ICM HX Sample Write-UpДокумент4 страницыIVMS ICM HX Sample Write-UpMarc Imhotep Cray, M.D.Оценок пока нет
- Thera 1-Case 2Документ3 страницыThera 1-Case 2marih2101masrОценок пока нет
- Case Report: Tikur Anbesa Specialized HospitalДокумент11 страницCase Report: Tikur Anbesa Specialized HospitalTefera LeteboОценок пока нет
- IM Gastro FinalДокумент10 страницIM Gastro FinalIzzyMaxinoОценок пока нет
- Chronic Kidney DiseaseДокумент6 страницChronic Kidney DiseaseDharshan SivaОценок пока нет
- Case Report LanaДокумент20 страницCase Report Lanaboody257Оценок пока нет
- Hypertension Case IMДокумент5 страницHypertension Case IMPerlyn Mac Basiloy - AloОценок пока нет
- 28 Years Male with QuadriparesisДокумент52 страницы28 Years Male with Quadriparesissaleh ahmedОценок пока нет
- Obstetrics N Gynaecology MADE EASYДокумент25 страницObstetrics N Gynaecology MADE EASYAlano S. LimgasОценок пока нет
- Physical ExamДокумент6 страницPhysical ExamTroy SilverioОценок пока нет
- History and Physical Notes - Final Report: Service Date: Admit Date: Performing ServiceДокумент5 страницHistory and Physical Notes - Final Report: Service Date: Admit Date: Performing Servicestarskyhutch0000100% (1)
- Internal Medicine (II) 2011 LogbookДокумент73 страницыInternal Medicine (II) 2011 LogbookQasim HaleimiОценок пока нет
- Internal Medicine Case Write Up 1Документ16 страницInternal Medicine Case Write Up 1Shafiah Aqilah Mohd Jamal67% (3)
- Chief ComplaintДокумент7 страницChief ComplaintyohannesОценок пока нет
- Deipan Arjunan - 20UMB03886 - CWU 2 - IM Group 1Документ30 страницDeipan Arjunan - 20UMB03886 - CWU 2 - IM Group 1Deipan ArjunanОценок пока нет
- Tehnik Penyusunan StatusДокумент7 страницTehnik Penyusunan StatusShelly Stephanie BintoroОценок пока нет
- Chronic SOAP Note for 51 Year Old Female with HyperlipidemiaДокумент3 страницыChronic SOAP Note for 51 Year Old Female with HyperlipidemiaJeffrey ViernesОценок пока нет
- Case ReportДокумент9 страницCase ReportBerhanu DigamoОценок пока нет
- Cadisal MW 1ST Week RequiementsДокумент36 страницCadisal MW 1ST Week RequiementsJonathan GonzalesОценок пока нет
- Nursing Care Plans for Neurological and Cardiovascular CasesДокумент15 страницNursing Care Plans for Neurological and Cardiovascular CasesJane FlorendoОценок пока нет
- Department of Internal Medicine: Non-Hodgkin LymphomaДокумент26 страницDepartment of Internal Medicine: Non-Hodgkin LymphomaHana FauziОценок пока нет
- Protocol - IM Intermittent Fever, Epi Pain, HematuriaДокумент4 страницыProtocol - IM Intermittent Fever, Epi Pain, HematuriaTrisОценок пока нет
- CRVHD Percipitated by IEДокумент14 страницCRVHD Percipitated by IEKemotherapy LifesucksОценок пока нет
- Internal Medicine Case Write Up 1Документ14 страницInternal Medicine Case Write Up 1Roshandiep GillОценок пока нет
- Obstetric and Gynacology CasesДокумент51 страницаObstetric and Gynacology CasesElly PetroОценок пока нет
- Constitutional: General Appearance: Healthy-Appearing, Well-Nourished, and Well-Developed. Level ofДокумент10 страницConstitutional: General Appearance: Healthy-Appearing, Well-Nourished, and Well-Developed. Level ofRichard ObinwankwoОценок пока нет
- Example Write Up #1: A Patient With Diarrhea: Problem ListДокумент8 страницExample Write Up #1: A Patient With Diarrhea: Problem ListMaher AltaeeОценок пока нет
- Clinico Pathological Correlation: Sarathchandran KДокумент26 страницClinico Pathological Correlation: Sarathchandran Ksarath chandranОценок пока нет
- Lower Limb WeaknessДокумент15 страницLower Limb WeaknessA MОценок пока нет
- Cervical PolypДокумент82 страницыCervical Polypdhainey100% (1)
- CASE 3 MEDICINE JULY 10 2019 AcutePyeloДокумент15 страницCASE 3 MEDICINE JULY 10 2019 AcutePyeloTrisОценок пока нет
- Case Report III Internal MedicineДокумент12 страницCase Report III Internal MedicineGidu Said0% (1)
- History: O Identifying DataДокумент10 страницHistory: O Identifying DataJofen Ann Hisoler TangpuzОценок пока нет
- BY: Shazlin Bt. Sabaah Salwa Hanim Bt. Mohd. Saifuddin Kamarulzaman B. MuzainiДокумент61 страницаBY: Shazlin Bt. Sabaah Salwa Hanim Bt. Mohd. Saifuddin Kamarulzaman B. MuzainiJohn Christopher LucesОценок пока нет
- Assessing GI IssuesДокумент3 страницыAssessing GI IssuesNick BrianОценок пока нет
- FNP 2 ObesityДокумент24 страницыFNP 2 Obesityapi-554096544Оценок пока нет
- HC - Issac DamianДокумент10 страницHC - Issac DamianOber SánchezОценок пока нет
- Neuroblastoma Dr. Rapp 5.17.2013Документ14 страницNeuroblastoma Dr. Rapp 5.17.2013Emily EresumaОценок пока нет
- Case HistoryДокумент3 страницыCase Historyapi-3747054Оценок пока нет
- Case Report V Internal MedicineДокумент14 страницCase Report V Internal MedicineGidu SaidОценок пока нет
- IM - HX and PE TBДокумент21 страницаIM - HX and PE TBTrisОценок пока нет
- Case Presentation On OVARIAN TUMOUR - PPTMДокумент26 страницCase Presentation On OVARIAN TUMOUR - PPTMshankar guledОценок пока нет
- DPR Assignment-2 Name: Sravya Reddy Madham MD - 3: Subjective Data (S)Документ8 страницDPR Assignment-2 Name: Sravya Reddy Madham MD - 3: Subjective Data (S)sravya madhamОценок пока нет
- Clinical Presentation On AppendicectomyДокумент30 страницClinical Presentation On AppendicectomyValarmathiОценок пока нет
- Intracranial Lesion CaseДокумент5 страницIntracranial Lesion CasepriscaОценок пока нет
- EM Case Write UpДокумент11 страницEM Case Write UpRaihana Rafi100% (2)
- SOAP note 1 - Breast CAДокумент4 страницыSOAP note 1 - Breast CAacvalvarioОценок пока нет
- Chronic Diseases - Lymes, Hpv, Hsv Mis-Diagnosis and Mistreatment: A New Approach to the EpidemicОт EverandChronic Diseases - Lymes, Hpv, Hsv Mis-Diagnosis and Mistreatment: A New Approach to the EpidemicРейтинг: 5 из 5 звезд5/5 (1)
- Biographical DataДокумент7 страницBiographical DataMoneef Al-dosariОценок пока нет
- Case Report on 44-Year-Old Woman with Excessive Menstrual BleedingДокумент16 страницCase Report on 44-Year-Old Woman with Excessive Menstrual Bleedingሌናፍ ኡሉምОценок пока нет
- Case Report IV Internal MedicineДокумент11 страницCase Report IV Internal MedicineGidu Said100% (1)
- Copper Sulfate HydrateДокумент2 страницыCopper Sulfate HydratesmexiiloriОценок пока нет
- Department of Child & Adolescent Health Respiratory Care Using A Peak Flow MeterДокумент2 страницыDepartment of Child & Adolescent Health Respiratory Care Using A Peak Flow MetersmexiiloriОценок пока нет
- Administration of VaccinesДокумент24 страницыAdministration of VaccinessmexiiloriОценок пока нет
- Sample Parent Letter I FallДокумент3 страницыSample Parent Letter I FallsmexiiloriОценок пока нет
- What Is A VolcanoДокумент4 страницыWhat Is A VolcanosmexiiloriОценок пока нет
- Neck Penetrating Tra PDFДокумент52 страницыNeck Penetrating Tra PDFsmexiiloriОценок пока нет
- The Diabetic Foot PDFДокумент29 страницThe Diabetic Foot PDFsmexiiloriОценок пока нет
- Neck Penetrating Tra PDFДокумент52 страницыNeck Penetrating Tra PDFsmexiiloriОценок пока нет
- Acids and BasesДокумент9 страницAcids and BasessmexiiloriОценок пока нет
- Spacer MaskДокумент2 страницыSpacer MasksmexiiloriОценок пока нет
- Memory PuzzleДокумент1 страницаMemory PuzzlesmexiiloriОценок пока нет
- Pediatrics History Taking (My Protocol)Документ4 страницыPediatrics History Taking (My Protocol)Jason Roy Edward NathanОценок пока нет
- The Arm Bone of The Arm-The Humerus Trochlea Articulates With The Ulna Capitulum Articulates With The RadiusДокумент11 страницThe Arm Bone of The Arm-The Humerus Trochlea Articulates With The Ulna Capitulum Articulates With The RadiussmexiiloriОценок пока нет
- Alcohol FermentationДокумент7 страницAlcohol FermentationsmexiiloriОценок пока нет
- CHEM 121L Distillation LabДокумент12 страницCHEM 121L Distillation LabMukesh TiwariОценок пока нет
- Information Technology Database Management Sample Past PaperДокумент1 страницаInformation Technology Database Management Sample Past PapersmexiiloriОценок пока нет
- Cells 1Документ12 страницCells 1smexiiloriОценок пока нет
- Cells 1Документ12 страницCells 1smexiiloriОценок пока нет
- How To Make A Nav Button in FireworksДокумент1 страницаHow To Make A Nav Button in FireworkssmexiiloriОценок пока нет
- Accounts ReceiptДокумент1 страницаAccounts ReceiptsmexiiloriОценок пока нет
- Lab Reaction TimeДокумент4 страницыLab Reaction TimesmexiiloriОценок пока нет
- Increase in KnowledgeДокумент4 страницыIncrease in KnowledgesmexiiloriОценок пока нет
- Thermal ExpansionДокумент4 страницыThermal ExpansionsmexiiloriОценок пока нет
- Accounts ReceiptДокумент1 страницаAccounts ReceiptsmexiiloriОценок пока нет
- Conservationof Momentum WorksheetДокумент2 страницыConservationof Momentum WorksheetsmexiiloriОценок пока нет
- Testing For Oxidizing and Reducing AgentsДокумент1 страницаTesting For Oxidizing and Reducing AgentssmexiiloriОценок пока нет
- CrystallizationДокумент36 страницCrystallizationsmexiiloriОценок пока нет
- Disease: Lori-Ann Leach 11/52 BiologyДокумент13 страницDisease: Lori-Ann Leach 11/52 BiologysmexiiloriОценок пока нет
- IVF Basic Principles SourceДокумент3 страницыIVF Basic Principles SourcereadtometooОценок пока нет
- Trichuris TrichiuraДокумент3 страницыTrichuris TrichiuraTwish BeraldeОценок пока нет
- NCM 104 Midterm Exams - 1Документ21 страницаNCM 104 Midterm Exams - 1Bing58Оценок пока нет
- Incomplete Right Bundle-Branch Block: A Developmental Variant Rather Than Conduction AbnormalityДокумент10 страницIncomplete Right Bundle-Branch Block: A Developmental Variant Rather Than Conduction AbnormalityErol SefchiОценок пока нет
- History of Microbiology-Notes For QuizДокумент20 страницHistory of Microbiology-Notes For QuizPipay AllenaОценок пока нет
- Global Burden of Cardiovascular Disease: Cardiovascular Diseases in IndiaДокумент17 страницGlobal Burden of Cardiovascular Disease: Cardiovascular Diseases in IndiaSaurabh BhattacharyaОценок пока нет
- Heart Structure and FunctionsДокумент3 страницыHeart Structure and FunctionsChristella KateОценок пока нет
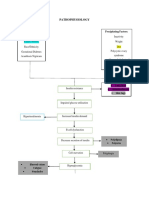
- Pathophysiology: Predisposing Factors: Precipitating FactorsДокумент2 страницыPathophysiology: Predisposing Factors: Precipitating FactorsJemsMei Comparativo MensuradoОценок пока нет
- Diastema Closure PDFДокумент5 страницDiastema Closure PDFsimon yonathanОценок пока нет
- Test Bank For Maternity and Womens Health Care 12th Edition Deitra Leonard Lowdermilk Shannon e Perry Mary Catherine Cashion Kathryn Rhodes Alden Ellen OlshanskyДокумент9 страницTest Bank For Maternity and Womens Health Care 12th Edition Deitra Leonard Lowdermilk Shannon e Perry Mary Catherine Cashion Kathryn Rhodes Alden Ellen Olshanskysubitodomesticcz70o3Оценок пока нет
- Entamoeba HistolyticaДокумент38 страницEntamoeba HistolyticaAbdul Ghafar OrakzaiiiОценок пока нет
- CPG On OmeДокумент6 страницCPG On OmeKita kitaОценок пока нет
- NCP Acute Pain Related To Tissue Ischemia As Manifested by Changes in Level of Consciousness PDFДокумент3 страницыNCP Acute Pain Related To Tissue Ischemia As Manifested by Changes in Level of Consciousness PDFOGNTVОценок пока нет
- Complete Physical Exam AbbreviationsДокумент4 страницыComplete Physical Exam Abbreviationseal772328Оценок пока нет
- Kumpulan Refarat Co-Ass Radiologi FK UntarДокумент15 страницKumpulan Refarat Co-Ass Radiologi FK UntarErwin DiprajaОценок пока нет
- Diabetes Mellitus: Anatomy, Physiology, Types, Diagnosis and ManagementДокумент66 страницDiabetes Mellitus: Anatomy, Physiology, Types, Diagnosis and ManagementyuliОценок пока нет
- Schreibman - Radiology of Joint Disease - My Practical ApproachДокумент16 страницSchreibman - Radiology of Joint Disease - My Practical ApproachborstОценок пока нет
- Norovirus 201309101051579338Документ3 страницыNorovirus 201309101051579338Jeeva maria GeorgeОценок пока нет
- 2022 SCO OneCare PM Prior Auth Table 3.1.2022-1Документ15 страниц2022 SCO OneCare PM Prior Auth Table 3.1.2022-1joshnemoОценок пока нет
- Designated Medical Event Dme List enДокумент3 страницыDesignated Medical Event Dme List enAmany HagageОценок пока нет
- Neonatal Air Leak Syndrome and The Role Of.3Документ9 страницNeonatal Air Leak Syndrome and The Role Of.3Claudia KosztelnikОценок пока нет
- Impact of Self-Management Education on Diabetes PatientsДокумент3 страницыImpact of Self-Management Education on Diabetes PatientsArief AndriyantoОценок пока нет
- Herpes Simplex I and IIДокумент50 страницHerpes Simplex I and IItummalapalli venkateswara raoОценок пока нет
- NCM109 Prelim ReviewerДокумент134 страницыNCM109 Prelim ReviewerNaomi Anne AsuntoОценок пока нет
- CA125: A Marker for Ovarian Cancer Detection and MonitoringДокумент3 страницыCA125: A Marker for Ovarian Cancer Detection and Monitoringडा. सत्यदेव त्यागी आर्यОценок пока нет
- Singkatan MedisДокумент16 страницSingkatan MedisfarizaОценок пока нет
- Enteral Nutrition Administration Inconsistent With Needs (NI-2.6)Документ2 страницыEnteral Nutrition Administration Inconsistent With Needs (NI-2.6)Hasna KhairunnisaGIZIОценок пока нет
- Number of Workers (Fill Total Number of Workers For Each Sub-Contractor at Work Daily) No - Sub-Contractor No. of Workers Suke Ca3Документ8 страницNumber of Workers (Fill Total Number of Workers For Each Sub-Contractor at Work Daily) No - Sub-Contractor No. of Workers Suke Ca3Nazulaila WitraОценок пока нет
- Cheatsheet PDFДокумент2 страницыCheatsheet PDFJudaeo SandovalОценок пока нет