Вам также может понравиться
- The Qi of Taking a Medical History and Performing a Physical ExaminationОт EverandThe Qi of Taking a Medical History and Performing a Physical ExaminationОценок пока нет
- Make Your Move: A Physician's Guide to Clinical and Non-Clinical Alternatives to Medical PracticeОт EverandMake Your Move: A Physician's Guide to Clinical and Non-Clinical Alternatives to Medical PracticeОценок пока нет
- History ComparisonДокумент3 страницыHistory Comparisonbaileyschaefer28Оценок пока нет
- Stress Tools: An 8 Week Guide to Relieve Stress and Regain ResilienceОт EverandStress Tools: An 8 Week Guide to Relieve Stress and Regain ResilienceОценок пока нет
- Communication in Medicine: A Guide for Students and Physicians on Interacting With Patients, Colleagues, and Everyone ElseОт EverandCommunication in Medicine: A Guide for Students and Physicians on Interacting With Patients, Colleagues, and Everyone ElseОценок пока нет
- Health Backwards: An Original Look from a Different PerspectiveОт EverandHealth Backwards: An Original Look from a Different PerspectiveОценок пока нет
- 4 Tips For Passing PACES: PreparationДокумент10 страниц4 Tips For Passing PACES: PreparationAhmed AbdelgelilОценок пока нет
- Final ReflectionДокумент4 страницыFinal Reflectionapi-546226145Оценок пока нет
- Running Head: CLINICAL REFLECTION 1Документ6 страницRunning Head: CLINICAL REFLECTION 1api-382642757Оценок пока нет
- FCPS Exam GuidanceДокумент7 страницFCPS Exam GuidancesafiОценок пока нет
- Final OutputДокумент35 страницFinal Outputaryana14_19906273Оценок пока нет
- The Hidden Messages in Food: Use Your Relationship with Food to Unlock Your True PotentialОт EverandThe Hidden Messages in Food: Use Your Relationship with Food to Unlock Your True PotentialОценок пока нет
- Christopher Kolar, MD: Emergency Medicine (Elective)Документ10 страницChristopher Kolar, MD: Emergency Medicine (Elective)Shaz ChindhyОценок пока нет
- Metastatic Breast Cancer: from Diagnosis to Complete Remission: An Intentional JourneyОт EverandMetastatic Breast Cancer: from Diagnosis to Complete Remission: An Intentional JourneyРейтинг: 5 из 5 звезд5/5 (1)
- Becoming a Surgeon: Life in a Surgical Residency and Timeless Lessons Learned ThereinОт EverandBecoming a Surgeon: Life in a Surgical Residency and Timeless Lessons Learned ThereinРейтинг: 5 из 5 звезд5/5 (1)
- Clinical Insights and Examination Techniques in OphthalmologyОт EverandClinical Insights and Examination Techniques in OphthalmologyОценок пока нет
- PTH 634 Reflection 3Документ2 страницыPTH 634 Reflection 3api-689349871Оценок пока нет
- How to Break Free from Anxiety: A Transformational Guide to WellnessОт EverandHow to Break Free from Anxiety: A Transformational Guide to WellnessОценок пока нет
- One Step: An Informative Introspection on the J-Pouch SurgeriesОт EverandOne Step: An Informative Introspection on the J-Pouch SurgeriesОценок пока нет
- Endocrine Fatigue: Discover the Role of Your Thyroid, Adrenals, Low Blood Sugar, and More.От EverandEndocrine Fatigue: Discover the Role of Your Thyroid, Adrenals, Low Blood Sugar, and More.Оценок пока нет
- Elective ReportДокумент10 страницElective ReportTootsie67% (3)
- How To Treat Palmoplantar Pustulosis Naturally: Put Your PPP In Remission And Get Your Life Back in 90 daysОт EverandHow To Treat Palmoplantar Pustulosis Naturally: Put Your PPP In Remission And Get Your Life Back in 90 daysОценок пока нет
- Mistakes Others Made:: Diagnoses and Very Minimal Evidence For SupportДокумент11 страницMistakes Others Made:: Diagnoses and Very Minimal Evidence For Supportkabal321Оценок пока нет
- The Challenge of Epilepsy: Complementary and Alternative SolutionsОт EverandThe Challenge of Epilepsy: Complementary and Alternative SolutionsОценок пока нет
- CLNC 2050 Review of Clinical SkillsДокумент4 страницыCLNC 2050 Review of Clinical Skillsapi-354751775Оценок пока нет
- PrintinternshipportfolioДокумент28 страницPrintinternshipportfolioapi-318339169Оценок пока нет
- Clinical Exposure Reflection PaperДокумент4 страницыClinical Exposure Reflection Paperapi-232621381Оценок пока нет
- Journal of Learning InsightsДокумент12 страницJournal of Learning InsightsJisel-Apple Bulan100% (2)
- The Fall and The Rise: A Teacher's Own Journey Following A Traumatic Brain InjuryОт EverandThe Fall and The Rise: A Teacher's Own Journey Following A Traumatic Brain InjuryОценок пока нет
- Phone Interview Questions ExampleДокумент3 страницыPhone Interview Questions ExamplePORTUGUES2014Оценок пока нет
- The Doctor Is In: 7 Easy, Positive Steps to Take Right Now to Transform Your HealthОт EverandThe Doctor Is In: 7 Easy, Positive Steps to Take Right Now to Transform Your HealthРейтинг: 2 из 5 звезд2/5 (1)
- Abstract 5Документ5 страницAbstract 5api-488383880100% (1)
- Predictably Irrational, Revised and Expanded Edition: The Hidden Forces That Shape Our DecisionsОт EverandPredictably Irrational, Revised and Expanded Edition: The Hidden Forces That Shape Our DecisionsРейтинг: 4.5 из 5 звезд4.5/5 (195)
- Qigong for Self-Refinement: Total Health with the 5 ElementsОт EverandQigong for Self-Refinement: Total Health with the 5 ElementsРейтинг: 5 из 5 звезд5/5 (2)
- When Bad Backs Happen to Good People: It’S Not All in Your HeadОт EverandWhen Bad Backs Happen to Good People: It’S Not All in Your HeadОценок пока нет
- Unified Integrative Medicine: A New Holistic Model for Personal Growth and Spiritual EvolutionОт EverandUnified Integrative Medicine: A New Holistic Model for Personal Growth and Spiritual EvolutionОценок пока нет
- GradereportДокумент1 страницаGradereportapi-371785797Оценок пока нет
- Exit Interview QuestionsДокумент3 страницыExit Interview Questionsapi-371785797Оценок пока нет
- Gradereport 5Документ1 страницаGradereport 5api-371785797Оценок пока нет
- Gradereport 1Документ1 страницаGradereport 1api-371785797Оценок пока нет
- Gradereport 2019-20 SummerДокумент1 страницаGradereport 2019-20 Summerapi-468018392Оценок пока нет
- Apta Membership CertificateДокумент1 страницаApta Membership Certificateapi-371785797Оценок пока нет
- Interdisciplinary Project - OsantowskiДокумент6 страницInterdisciplinary Project - Osantowskiapi-371785797Оценок пока нет
- Case Report 1 Final Draft 12Документ65 страницCase Report 1 Final Draft 12api-371785797Оценок пока нет
- Post Print Score ReportДокумент1 страницаPost Print Score Reportapi-371785797Оценок пока нет
- Group PresentationДокумент13 страницGroup Presentationapi-371785797Оценок пока нет
- Mental Health Conference Series Cognitive and Behavioral Sequelae of Covid-19 InfectionДокумент1 страницаMental Health Conference Series Cognitive and Behavioral Sequelae of Covid-19 Infectionapi-371785797Оценок пока нет
- Osantowski Rolling-Teaching Activity Paper 1Документ11 страницOsantowski Rolling-Teaching Activity Paper 1api-371785797Оценок пока нет
- Esophageal Cancer InserviceДокумент18 страницEsophageal Cancer Inserviceapi-371785797Оценок пока нет
- Part 1 Task A Field Observation - OsantowskiДокумент6 страницPart 1 Task A Field Observation - Osantowskiapi-371785797Оценок пока нет
- Jennifer Exercise ListДокумент1 страницаJennifer Exercise Listapi-371785797Оценок пока нет
- Self Assessment - Second Year 2019-2020Документ4 страницыSelf Assessment - Second Year 2019-2020api-371785797Оценок пока нет
- Community Resource ProjectДокумент9 страницCommunity Resource Projectapi-371785797Оценок пока нет
- Gradereport 2Документ1 страницаGradereport 2api-371785797Оценок пока нет
- Greatest Moment Slide - Osantowski and SlocumДокумент1 страницаGreatest Moment Slide - Osantowski and Slocumapi-371785797Оценок пока нет
- Final Ethics Paper - OsantowskiДокумент10 страницFinal Ethics Paper - Osantowskiapi-371785797Оценок пока нет
- Updated Game PlanДокумент3 страницыUpdated Game Planapi-371785797Оценок пока нет
- Case Report - Osantowski and AyacheДокумент14 страницCase Report - Osantowski and Ayacheapi-371785797Оценок пока нет
- GradereportДокумент1 страницаGradereportapi-467445554Оценок пока нет
- Gradereport 3Документ1 страницаGradereport 3api-371785797Оценок пока нет
- Citi - OsantowskiДокумент1 страницаCiti - Osantowskiapi-371785797Оценок пока нет
- Ptso Leadership 2018-2019Документ1 страницаPtso Leadership 2018-2019api-371785797Оценок пока нет
- Ptso Certification 2018-2019Документ1 страницаPtso Certification 2018-2019api-371785797Оценок пока нет
- Exam 4 Study Guide - Eo JTZДокумент16 страницExam 4 Study Guide - Eo JTZapi-371785797Оценок пока нет
- Osantowski Pre 2019 2Документ7 страницOsantowski Pre 2019 2api-371785797Оценок пока нет
- MiraДокумент1 страницаMiraJulian Ross EpetiaОценок пока нет
- CMS-855B - 04052021Документ49 страницCMS-855B - 04052021Sheldon GunbyОценок пока нет
- Negotiating A Managed Care ContractДокумент1 страницаNegotiating A Managed Care ContractPremium GeeksОценок пока нет
- DDS Pre-Hearing Performance Oversight Questions and AnswersДокумент37 страницDDS Pre-Hearing Performance Oversight Questions and AnswersOffice of Councilmember Brianne K. NadeauОценок пока нет
- HCS-341-Human Resource Management RolesДокумент4 страницыHCS-341-Human Resource Management RolesJulia A. SkahanОценок пока нет
- Edge 4030 Press ReleaseДокумент1 страницаEdge 4030 Press Releaseapi-432243790Оценок пока нет
- Charge Nurse Resume Example PDFДокумент2 страницыCharge Nurse Resume Example PDFJett VillablancaОценок пока нет
- DHCP Sodiumchlorided BaxterДокумент3 страницыDHCP Sodiumchlorided Baxterjraz141Оценок пока нет
- Princess Ercka B. Galapon: Contact ObjectiveДокумент2 страницыPrincess Ercka B. Galapon: Contact ObjectiveEmpress PОценок пока нет
- Roshni Issue 26: Sep 6 - Sep 20Документ16 страницRoshni Issue 26: Sep 6 - Sep 20Anonymous ZjF6TYbОценок пока нет
- WARFARIN Prescribing Guidelines For The Management of Patients On Anticoagulant Therapy WIRRAL NHSДокумент14 страницWARFARIN Prescribing Guidelines For The Management of Patients On Anticoagulant Therapy WIRRAL NHSNavojit ChowdhuryОценок пока нет
- Risk PDFДокумент18 страницRisk PDFantehenОценок пока нет
- Prevention of Catheter Associated Urinary Tract InfectionsДокумент61 страницаPrevention of Catheter Associated Urinary Tract Infectionsdex99Оценок пока нет
- NYS Dept. of Health: NY State of Health PresentationДокумент39 страницNYS Dept. of Health: NY State of Health PresentationState Senator Liz KruegerОценок пока нет
- Marier - ST Onge 510essayДокумент7 страницMarier - ST Onge 510essayGenevieveMarierSt-OngeОценок пока нет
- Moa Template For Adopt A HospitalДокумент5 страницMoa Template For Adopt A HospitalLou Annabelle GanacОценок пока нет
- PolicyBazaar Health Insurance - Cover Rs.5 Lac @rs. 10 - DayДокумент3 страницыPolicyBazaar Health Insurance - Cover Rs.5 Lac @rs. 10 - DayAshish PatelОценок пока нет
- Community Resource List 15-16Документ2 страницыCommunity Resource List 15-16Sergio Hidalgo BronfmanОценок пока нет
- Pennsylvania Insurance Department Complaint Form 2015A Re Allstate Insurance Claim October 14, 2016Документ134 страницыPennsylvania Insurance Department Complaint Form 2015A Re Allstate Insurance Claim October 14, 2016Stan J. CaterboneОценок пока нет
- Carnival Fun Job OfferДокумент4 страницыCarnival Fun Job OfferChristous PkОценок пока нет
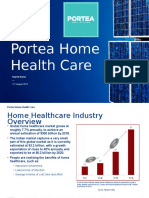
- Portea Home Health CareДокумент17 страницPortea Home Health CareAbhai Pratap SinghОценок пока нет
- GLP DetailsДокумент2 страницыGLP DetailsRajeev DominicОценок пока нет
- Curriculum VitaeДокумент3 страницыCurriculum Vitaeakurita738Оценок пока нет
- Pharmacy Practice Prof. Yahya: ContinueДокумент23 страницыPharmacy Practice Prof. Yahya: Continueكسلان اكتب اسميОценок пока нет
- October 2019Документ64 страницыOctober 2019Eric Santiago100% (1)
- New Hci ResumeДокумент2 страницыNew Hci Resumeapi-397532577Оценок пока нет
- PDR - 03072014 Philhealth Form PDFДокумент1 страницаPDR - 03072014 Philhealth Form PDFMARY ANGELIE G. MANALANGОценок пока нет
- Bumrungrad HospitalДокумент3 страницыBumrungrad HospitalAhmadnur kholilОценок пока нет
- Il444 2378BДокумент14 страницIl444 2378BKevin MccullumОценок пока нет
- Health Insurance: Awareness, Utilization, and Its Determinants Among The Urban Poor in Delhi, IndiaДокумент8 страницHealth Insurance: Awareness, Utilization, and Its Determinants Among The Urban Poor in Delhi, IndiaY S KusumaОценок пока нет