Вам также может понравиться
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (344)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (399)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (120)
- tmp4017 TMPДокумент7 страницtmp4017 TMPFrontiersОценок пока нет
- Vitiligo - Pathogenesis, Clinical Features, and Diagnosis - UpToDateДокумент38 страницVitiligo - Pathogenesis, Clinical Features, and Diagnosis - UpToDateInna MeratiОценок пока нет
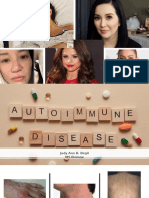
- Autoimmune DiseasesДокумент26 страницAutoimmune DiseasesCherry Reyes-PrincipeОценок пока нет
- Rheumatoid ArthritisДокумент33 страницыRheumatoid Arthritisdtpmaharaja100% (1)
- Therapeutic Apheresis in VeterinaryДокумент5 страницTherapeutic Apheresis in VeterinaryEliDavidОценок пока нет
- Autoimmune DiseasesДокумент27 страницAutoimmune DiseasesJudy BegilОценок пока нет
- Mold and Mycotoxins. Effects On The Neurological and Immune SystemsДокумент32 страницыMold and Mycotoxins. Effects On The Neurological and Immune Systemsjsenterprises100% (1)
- Chronic UrticariaДокумент40 страницChronic UrticariaeeeeewwwwwОценок пока нет
- Disorders of The Immune System ImmunityДокумент7 страницDisorders of The Immune System ImmunityMarinelle TumanguilОценок пока нет
- SclerademaДокумент5 страницSclerademaMichael SponslerОценок пока нет
- Curriculum Vitae Prof. Francesco Ria Biographic InformationДокумент9 страницCurriculum Vitae Prof. Francesco Ria Biographic InformationnoncanimussurdisОценок пока нет
- Systemic Lupus ErythematosusДокумент9 страницSystemic Lupus ErythematosusTheeya QuigaoОценок пока нет
- 5 Benefits of BoswelliaДокумент6 страниц5 Benefits of BoswelliaPaulОценок пока нет
- Vitiligo Cures BookДокумент98 страницVitiligo Cures BookShah NoorОценок пока нет
- Vaccines-2013 Book FinalДокумент164 страницыVaccines-2013 Book FinalChitra Sekar100% (1)
- A Gut Feeling For Immune Dysregulation & Neuroinflammation in Autism by Aristo Vojdani, PHD, MSC, MT and Jama LambertДокумент9 страницA Gut Feeling For Immune Dysregulation & Neuroinflammation in Autism by Aristo Vojdani, PHD, MSC, MT and Jama LambertautismoneОценок пока нет
- UrticarieДокумент13 страницUrticarieCocea MihaiОценок пока нет
- DM Type 1Документ14 страницDM Type 1Yogi SetiawanОценок пока нет
- The Thyroid SolutionДокумент21 страницаThe Thyroid SolutionJosh Bill100% (1)
- Gel Formulation of Drug X Drug and Evaluate Its EfficacyДокумент26 страницGel Formulation of Drug X Drug and Evaluate Its EfficacyPriyanka YadavОценок пока нет
- APECED FactsheetДокумент6 страницAPECED FactsheetAditya Yudha PratamaОценок пока нет
- Banking Crimes and Financial Criminals - The Global and Local Impact PDFДокумент1 622 страницыBanking Crimes and Financial Criminals - The Global and Local Impact PDFkitty katОценок пока нет
- Natural Remedies To Increase Platelet Count: Swati BurungaleДокумент5 страницNatural Remedies To Increase Platelet Count: Swati BurungaleraamОценок пока нет
- Engineering A New Mouse Model For Vitiligo 2012 Journal of Investigative DermatologyДокумент4 страницыEngineering A New Mouse Model For Vitiligo 2012 Journal of Investigative DermatologyAurelian Corneliu MoraruОценок пока нет
- UntitledДокумент66 страницUntitledPhilip Edward OsborneОценок пока нет
- MCQ Immunology BasicДокумент71 страницаMCQ Immunology BasicMatthew HallОценок пока нет
- Blood Cell - An Overview of Studies in HematologyДокумент360 страницBlood Cell - An Overview of Studies in HematologyGNiqMОценок пока нет
- Chronic Gastritis Is Autoimmune or EnvironmentalДокумент4 страницыChronic Gastritis Is Autoimmune or EnvironmentalovidiuticaОценок пока нет
- Probiotic Supplements, Foods and Benefits: A Concise Guide From Epigenetic LabsДокумент29 страницProbiotic Supplements, Foods and Benefits: A Concise Guide From Epigenetic LabsJane Uymatiao0% (1)