Вам также может понравиться
- Anecdotal Record For RPMSДокумент3 страницыAnecdotal Record For RPMScristito inovalОценок пока нет
- AnecdotalДокумент3 страницыAnecdotalLeony CiprianoОценок пока нет
- Student Progress ReportsДокумент3 страницыStudent Progress ReportsMarvinОценок пока нет
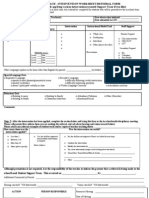
- Tiered Approach Referral SheetДокумент3 страницыTiered Approach Referral SheetUruz86100% (1)
- Department of Education: Mainaga-San Francisco Elementary SchoolДокумент2 страницыDepartment of Education: Mainaga-San Francisco Elementary SchoolFarrah Joy Aguilar NietesОценок пока нет
- SotTeam Application2014Документ7 страницSotTeam Application2014Martin SakaОценок пока нет
- Financial Literacy CaravanДокумент1 страницаFinancial Literacy CaravanJohn Aldrin ResosОценок пока нет
- Cararayan National High School: Department of Education Division of City Schools Naga CityДокумент2 страницыCararayan National High School: Department of Education Division of City Schools Naga CityMaro Mempin-TabinasОценок пока нет
- Personal Information: Guilid Community Learning CenterДокумент3 страницыPersonal Information: Guilid Community Learning CenterClemente B Cipriano Jr.Оценок пока нет
- ICT - Equipment Request Form: Schools Division Office of Alaminos CityДокумент2 страницыICT - Equipment Request Form: Schools Division Office of Alaminos CityCarlo AgustinОценок пока нет
- Learner's Basic Profile Als Enrolment Form (Af2) : Republic of The Philippines Department of EducationДокумент3 страницыLearner's Basic Profile Als Enrolment Form (Af2) : Republic of The Philippines Department of EducationMelodie TabuadaОценок пока нет
- Notice Form Case Conference FormДокумент1 страницаNotice Form Case Conference FormFarrah AndayaОценок пока нет
- ALS Form 2Документ3 страницыALS Form 2Gan CapinОценок пока нет
- Als Form 2Документ1 страницаAls Form 2miro.mantinОценок пока нет
- Modified Als Enrolment Form (Af2) Learner's Basic Profile: Republic of The Philippines Department of EducationДокумент1 страницаModified Als Enrolment Form (Af2) Learner's Basic Profile: Republic of The Philippines Department of EducationLight flamerОценок пока нет
- For BGCD Membership Form CompletionДокумент4 страницыFor BGCD Membership Form CompletionArshad AliОценок пока нет
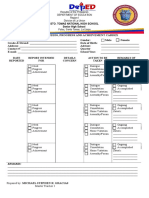
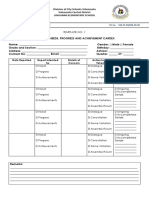
- Learner's Needs, Progress and Achievement CardexДокумент3 страницыLearner's Needs, Progress and Achievement CardexJeremie Mariano AbanОценок пока нет
- Screenshot 2023-04-26 at 1.41.06 PMДокумент1 страницаScreenshot 2023-04-26 at 1.41.06 PMJericho GonzalesОценок пока нет
- Als Enrolment Form (Af2) Learner's Basic Profile: Republic of The Philippines Department of EducationДокумент1 страницаAls Enrolment Form (Af2) Learner's Basic Profile: Republic of The Philippines Department of EducationPatricia Villate100% (1)
- INTERVIEW EVALUATIONДокумент1 страницаINTERVIEW EVALUATIONRAFI K.AОценок пока нет
- Learner Progress ReportДокумент2 страницыLearner Progress ReportRamonОценок пока нет
- Department of Education: Republic of The PhilippinesДокумент3 страницыDepartment of Education: Republic of The PhilippinesGrace VillarinОценок пока нет
- CARDEXДокумент5 страницCARDEXAIRA NINA COSICOОценок пока нет
- Membership Form PDFДокумент1 страницаMembership Form PDFexcelino bueno jrОценок пока нет
- Reference Check FormДокумент1 страницаReference Check FormMolly BakerОценок пока нет
- Annex B ALS Enrolment FormДокумент1 страницаAnnex B ALS Enrolment FormBryan GenoОценок пока нет
- AF2Документ1 страницаAF2Allena Mitzi PadernalОценок пока нет
- Learner progress trackerДокумент2 страницыLearner progress trackerLEONARD JIM DUMADANGONОценок пока нет
- CARDEXДокумент2 страницыCARDEXMichael Stephen GraciasОценок пока нет
- Modified Als Enrolment Form (Af2) Learner's Basic ProfileДокумент4 страницыModified Als Enrolment Form (Af2) Learner's Basic ProfileEspecacion TejadaОценок пока нет
- Customer SurveyДокумент12 страницCustomer SurveyGiang Lê NinhОценок пока нет
- Interviewee Info Form - Indonesia - 2019Документ1 страницаInterviewee Info Form - Indonesia - 2019Agustami SitorusОценок пока нет
- Interviewee Info Form - Indonesia - 2020Документ1 страницаInterviewee Info Form - Indonesia - 2020Agustami SitorusОценок пока нет
- Interviewee Info Form - Indonesia - 2019Документ1 страницаInterviewee Info Form - Indonesia - 2019Agustami SitorusОценок пока нет
- CardexДокумент2 страницыCardexRonnie TambalОценок пока нет
- Nabulao National High School - Cayhagan Extension: Parents/Guardians Communication CardexДокумент3 страницыNabulao National High School - Cayhagan Extension: Parents/Guardians Communication CardexChonaMarieEstellinaОценок пока нет
- Application Incoming 1st Year TCC 1Документ1 страницаApplication Incoming 1st Year TCC 1Judelyn P SarajenaОценок пока нет
- Salcedo Vocational High School: ST ND RDДокумент2 страницыSalcedo Vocational High School: ST ND RDRodolfo ObanilОценок пока нет
- Form 2 (Outreach Activity)Документ1 страницаForm 2 (Outreach Activity)Joris YapОценок пока нет
- 2013 IBDReview RegДокумент1 страница2013 IBDReview Regmartina.capozzaОценок пока нет
- Call Parent SlipДокумент1 страницаCall Parent SlipNancy CuplangОценок пока нет
- Physics Investigatory ProjectДокумент14 страницPhysics Investigatory ProjectKeerthanaa GSОценок пока нет
- Parents Guardian Communication IndexДокумент1 страницаParents Guardian Communication IndexClairenceValderasОценок пока нет
- Template No. 1: Date Reported Report Intended For Details of Concern Action To Be Taken Remarks of Action TakenДокумент2 страницыTemplate No. 1: Date Reported Report Intended For Details of Concern Action To Be Taken Remarks of Action TakenLuzviminda Morallos CamaristaОценок пока нет
- Lingunan Elementary Progress ReportsДокумент2 страницыLingunan Elementary Progress ReportsLuzviminda Morallos CamaristaОценок пока нет
- CardexДокумент2 страницыCardexLuzviminda Morallos CamaristaОценок пока нет
- Registered Financial Planners Membership ApplicationДокумент1 страницаRegistered Financial Planners Membership ApplicationElmer ZabalaОценок пока нет
- Learner Progress ReportДокумент2 страницыLearner Progress ReportMaria Manoa Gantala TomonОценок пока нет
- Feasib Survey Questionnaire StudentsДокумент1 страницаFeasib Survey Questionnaire Studentsyel5buscatoОценок пока нет
- Child Behavior Incident Report Form TemplateДокумент1 страницаChild Behavior Incident Report Form TemplaterfgzjrjbgxОценок пока нет
- English PlanДокумент2 страницыEnglish PlanGerardo LopezОценок пока нет
- Apply for Financial Aid at Alfred UniversityДокумент6 страницApply for Financial Aid at Alfred UniversityAlmogdadОценок пока нет
- Otis Brock Elementary School: February 14, 2017Документ3 страницыOtis Brock Elementary School: February 14, 2017bookwormjoeyОценок пока нет
- Among Teenagers of Rizal High SchoolДокумент1 страницаAmong Teenagers of Rizal High SchoolElyzia Marites CastilarОценок пока нет
- ANECDOTALДокумент2 страницыANECDOTALCherry Marie BudoОценок пока нет
- DepEd Isabela School ProfileДокумент5 страницDepEd Isabela School ProfileAiza CorouzОценок пока нет
- HUMSS Questionnaire MarielДокумент5 страницHUMSS Questionnaire MarielMalungkot Kapag Walang LambingОценок пока нет
- NRIHOMELOAN - Application FormДокумент9 страницNRIHOMELOAN - Application FormgrgcharyОценок пока нет
- DRR Lesson 1Документ16 страницDRR Lesson 1Nora TalagОценок пока нет
- Lesson 1: Disaster and HazardДокумент16 страницLesson 1: Disaster and HazardNora TalagОценок пока нет
- Portfolio ArrangementДокумент1 страницаPortfolio ArrangementNora TalagОценок пока нет
- DepEdfinal RPMSManual May28,2018Документ245 страницDepEdfinal RPMSManual May28,2018graxia04100% (1)
- List of MovsДокумент13 страницList of MovsNora TalagОценок пока нет
- PPST Module 7Документ10 страницPPST Module 7Nora Talag100% (2)
- Portfolio Preparation and Organzation For T I-TIIIДокумент69 страницPortfolio Preparation and Organzation For T I-TIIIchrisesteban1978100% (1)
- Grade 7-10 - Mapeh 1st QuarterДокумент54 страницыGrade 7-10 - Mapeh 1st QuarterNora TalagОценок пока нет
- PPST CalculatorДокумент27 страницPPST CalculatorNora TalagОценок пока нет
- AseanДокумент2 страницыAseanNora TalagОценок пока нет
- Grade 7-10 - Mapeh 1st QuarterДокумент54 страницыGrade 7-10 - Mapeh 1st QuarterNora TalagОценок пока нет
- Gad PoliciesДокумент1 страницаGad PoliciesNora TalagОценок пока нет
- Time Measuring DevicesДокумент9 страницTime Measuring DevicesNora Talag100% (1)
- RRR Template For MBA 3 - Shahrukh - 2000 - CorrectedДокумент8 страницRRR Template For MBA 3 - Shahrukh - 2000 - CorrectedShahrukh HasanОценок пока нет
- PRC Secondary General Education 2007 ExamДокумент48 страницPRC Secondary General Education 2007 ExamDhena H Rasul SabdulaОценок пока нет
- Lala National HS Bags 2nd Place at Sagayan Festival & Nutrition Month ReportДокумент3 страницыLala National HS Bags 2nd Place at Sagayan Festival & Nutrition Month ReportFeby ApatОценок пока нет
- Ies CollegeДокумент5 страницIes Collegeravi maheshwari100% (1)
- Irham Personal StatementДокумент2 страницыIrham Personal StatementAli YundaОценок пока нет
- UCSP Quarter 1 Module 1-6Документ9 страницUCSP Quarter 1 Module 1-6Janine Ernie CabuslayОценок пока нет
- Siddhi - Bandekar22@ibsindia - or GДокумент1 страницаSiddhi - Bandekar22@ibsindia - or Gbhagyesh taleleОценок пока нет
- MemoДокумент4 страницыMemoCindy RellaОценок пока нет
- Berkeley Response Letter 9.21.20 PDFДокумент3 страницыBerkeley Response Letter 9.21.20 PDFLive 5 NewsОценок пока нет
- Cargo Work BДокумент3 страницыCargo Work BJasonllОценок пока нет
- Frontlearn Institute Fee Structure for Culinary Arts, ICT and Business Management CoursesДокумент1 страницаFrontlearn Institute Fee Structure for Culinary Arts, ICT and Business Management CoursesNjihiaОценок пока нет
- Why Use Logic Puzzles With Students?Документ9 страницWhy Use Logic Puzzles With Students?SA Grade 3 Eagle B2Оценок пока нет
- DLL Mathematics 6 q4 w7Документ7 страницDLL Mathematics 6 q4 w7Dan Bilan100% (1)
- Communicative Language TeachingДокумент37 страницCommunicative Language TeachingAulya Ingin Bertahan80% (5)
- Murray Print Model For Curriculum DeveloДокумент8 страницMurray Print Model For Curriculum Develonawazish100% (1)
- Sharons ResumeДокумент3 страницыSharons Resumeapi-226496411Оценок пока нет
- Grad School Cover LetterДокумент5 страницGrad School Cover Letterapi-252513947Оценок пока нет
- Educational Medical, Health and Family Welfare Department, Guntur-Staff NurseQualification Medical Health Family Welfare Dept Guntur Staff Nurse PostsДокумент4 страницыEducational Medical, Health and Family Welfare Department, Guntur-Staff NurseQualification Medical Health Family Welfare Dept Guntur Staff Nurse PostsTheTubeGuruОценок пока нет
- (New Ecologies For The Twenty-First Century) Arturo Escobar - Territories of Difference - Place, Movements, Life, Redes (2008, Duke University Press Books) PDFДокумент419 страниц(New Ecologies For The Twenty-First Century) Arturo Escobar - Territories of Difference - Place, Movements, Life, Redes (2008, Duke University Press Books) PDFMara Dicenta VilkerОценок пока нет
- Grade 9 Catch Up FridayДокумент4 страницыGrade 9 Catch Up FridayRussОценок пока нет
- An Action Research I. Research ProblemДокумент3 страницыAn Action Research I. Research Problemsalve renomeronОценок пока нет
- Popcorn CylindersДокумент4 страницыPopcorn Cylindersapi-309050107Оценок пока нет
- Task 3 Assessment CommentaryДокумент9 страницTask 3 Assessment Commentaryapi-317861393Оценок пока нет
- GenMathG11 Q1 Mod4 ExponentialFunctions v3 PDFДокумент43 страницыGenMathG11 Q1 Mod4 ExponentialFunctions v3 PDFTin Galias91% (76)
- One Year Special Extended Classroom Program for IIT-JEE 2011Документ4 страницыOne Year Special Extended Classroom Program for IIT-JEE 2011AnubhavОценок пока нет
- DownloadfileДокумент7 страницDownloadfileFernanda FreitasОценок пока нет
- 7 Issues and Challenges in Popular LiteratureДокумент40 страниц7 Issues and Challenges in Popular LiteratureShekinah Louise IdoОценок пока нет
- O2 Life Skills Module 4 Work Habits Conduct Modular FINAL VERSION 8-13-2020Документ64 страницыO2 Life Skills Module 4 Work Habits Conduct Modular FINAL VERSION 8-13-2020Tata Lino100% (4)
- Travis - An Empirical Test of Maharishi's Junction Point Model of States of ConsciousnessДокумент14 страницTravis - An Empirical Test of Maharishi's Junction Point Model of States of ConsciousnessAMTRОценок пока нет