Академический Документы
Профессиональный Документы
Культура Документы
Dual-Energy CT of The Brain and Intracranial Vessels
Загружено:
Muhammad Rafiee SukmaОригинальное название
Авторское право
Доступные форматы
Поделиться этим документом
Поделиться или встроить документ
Этот документ был вам полезен?
Это неприемлемый материал?
Пожаловаться на этот документАвторское право:
Доступные форматы
Dual-Energy CT of The Brain and Intracranial Vessels
Загружено:
Muhammad Rafiee SukmaАвторское право:
Доступные форматы
D u a l - E n e r g y C T • R ev i ew
Postma et al.
Dual-Energy CT of the Brain and Intracranial Vessels
Dual-Energy CT
Review
Downloaded from www.ajronline.org by 36.73.159.237 on 05/14/19 from IP address 36.73.159.237. Copyright ARRS. For personal use only; all rights reserved
Dual-Energy CT of the Brain
and Intracranial Vessels
Alida A. Postma1 OBJECTIVE. The purpose of this review is to summarize the principles and applications
Paul A. M. Hofman1 of dual-energy CT in evaluation of the brain and the intracranial blood vessels.
Annika A. R. Stadler 1 CONCLUSION. One major advantage of dual-energy CT is the capability of material
Robert J. van Oostenbrugge2 differentiation. In general, this property can be applied to bone removal in CT angiography
Maud P. M. Tijssen1 for easier and faster postprocessing. In neuroradiology, material decomposition allows detec-
tion of hemorrhage on contrast-enhanced CT scans and facilitates the search for the underly-
Joachim E. Wildberger 1
ing pathologic mechanism of hematomas. The combination of low radiation dose and advan-
Postma AA, Hofman PAM, Stadler AAR, van tageous spectral information (blood vs contrast) from these datasets justifies broad clinical
Oostenbrugge RJ, Tijssen MPM, Wildberger JE implementation of dual-energy CT in neuroradiology.
B
etween the discovery of x-rays in clinical implementation [3–5]. Since the ear-
1895 and the introduction of CT ly 2000s, the evolution of DECT led to a re-
in 1971, neuroradiology entailed vival in modern MDCT scanners through the
radiography, myelography, pneu- use of two simultaneous working x-ray tubes
moencephalography, and angiography as indi- (Siemens Healthcare), fast peak kilovoltage
rect tools for imaging of the brain and spinal switching (GE Healthcare), and dual-layer de-
cord. CT marked the beginning of a revolu- tection systems (Philips Healthcare). Since the
Keywords: brain hemorrhage, dual-energy CT (DECT),
dual-energy CT angiography, material differentiation
tionary era. The internal structure of the brain implementation of DECT, the number of indi-
could be visualized without invasive exami- cations has increased, especially in abdominal
DOI:10.2214/AJR.12.9115 nations [1]. Brain, blood vessels, and osseous and cardiac imaging [6–15]. Neuroradiologic
structures were directly evaluated. Adminis- application lags behind the other uses, how-
Received April 24, 2012; accepted after revision
tration of contrast material enabled better vis- ever [16]. The advantage of DECT is the abil-
May 8, 2012.
ualization of the vessels and the breakdown of ity to characterize material-specific and non–
Publication of this supplement to the American Journal of the blood-brain barrier. In the next decades, material-specific image fusion by combining
Roentgenology is made possible by an unrestricted grant CT had substantial developments, including low and high peak voltage acquisitions [17–19].
from Siemens Healthcare. helical acquisition and MDCT in the late For imaging of the brain and intracrani-
J. E. Wildberger is a member of the speakers’ bureau of
1990s, which enabled faster data acquisition al blood vessels, material decomposition can
Bayer Healthcare, Boston Scientific, GE Healthcare, and and isotropy of datasets and, last but not least, be applied for bone removal in CT angiogra-
Siemens Healthcare and is affiliated with an institution dual-energy scanning. phy (CTA). In addition, iodine can be virtually
that has received research grants from Bayer MRI was introduced in the late 1970s and subtracted from the images, resulting in cal-
Healthcare, GE Healthcare, Philips Healthcare, and
to a large extent has replaced CT in neuro- culated virtual unenhanced images. The latter
Siemens Healthcare.
radiology in clinical routine. However, there can be used to identify the underlying patho-
1
Department of Radiology, Maastricht University Medical are still indications for CT: imaging of acute- logic mechanism in patients with brain hemor-
Centre, PO Box 5800, 6202 AZ Maastricht, The ly ill patients, diagnosis of acute (subarach- rhage [20, 21] and after previous delivery of
Netherlands. Address correspondence to A. A. Postma noid) hemorrhage, and imaging of patients contrast medium, as after intraarterial recana-
(l.jacobi@mumc.nl).
with contraindications to MRI. These indica- lization in patients with stroke to differentiate
2
Department of Neurology, Maastricht University tions necessitate ongoing development of CT iodine and hemorrhage [22, 23]. Calculation
Medical Centre, Maastricht, The Netherlands. as, for example, dual-energy CT (DECT). of single-energy images can be useful because
The first publications on DECT appeared of the increased vascular opacification at low
AJR 2012; 199:S26–S33
in the late 1970s [2]. At that time, however, kilovoltage. With higher kilovoltage, visuali-
0361–803X/12/1995–S26 owing to technical shortcomings (e.g., insuf- zation of structures near the skull base is less
ficient spatial resolution, long scan duration, affected by beam-hardening artifacts than it is
© American Roentgen Ray Society and misregistration), it did not receive broad at low kilovoltage [24].
S26 AJR:199, November 2012
Dual-Energy CT of the Brain and Intracranial Vessels
Background Physics DSA being the actual reference standard. Over dual-energy bone removal were shorter.
X-ray attenuation of materials is based on the last decade, CTA has gained its place in They noticed better vessel delineation at the
the photoelectric effect and Compton scat- evaluation of stenosis and aneurysm detection skull base but similar vessel visualization of
tering. The photoelectric effect is responsi- [29, 30]. Improvements in MDCT, including the intracranial vessels. They found that cal-
ble for the largest part of the attenuation and shorter scanning times, led to improved arterial cified plaques could be differentiated from
depends on the energy of the x-ray beam and phase imaging without interfering with venous the lumen and were automatically removed
Downloaded from www.ajronline.org by 36.73.159.237 on 05/14/19 from IP address 36.73.159.237. Copyright ARRS. For personal use only; all rights reserved
on the atomic number (Z) of the material. In contrast enhancement. Moreover, bone sub- in dual-energy bone removal.
materials with a higher atomic number, the traction techniques such as matched mask bone Mühlenbruch et al. [35] investigated the
photoelectric effect prevails, whereas in ma- elimination were developed to improve delin- carotid and intracranial vessels in 16 patients
terials with a lower atomic number, Comp- eation of vasculature adjacent to bony struc- with symptomatic carotid artery stenosis.
ton scatter occurs most. Thus the higher the tures, such as the skull base [31–33]. The lim- They concluded that dual-energy CTA for
atomic number, the greater is the photoelec- itations of these bone removal techniques are extracranial vessels was as good as MR angi-
tric effect and the greater is the attenuation possible misregistration due to patient motion ography (MRA) but yielded additional mor-
of the x-ray beam [25]. When the photon en- between and during the enhanced and the un- phologic information, for example, on calci-
ergy exceeds the binding energy of the K- enhanced acquisitions. In addition, the require- fications. The investigators found, however,
shell electron of the material, the attenuation ment for double scanning increases the radia- that smaller intracranial arteries were better
coefficient suddenly increases in an effect tion dose. Postprocessing is not automatic and depicted with 3-T MRA.
called K edge. is user dependent, making it time-consuming Hegde et al. [36] found that DECT angi-
The closer the energy level of the x-ray and difficult to standardize. These problems ne- ography was a robust and efficient technique
beam is to the K edge of a substance such as cessitate multiplanar reformation and addition- in their clinical practice. They found 30–50%
iodine, the more the beam attenuates. Thus al postprocessing to avoid misdiagnosis. radiation dose reduction compared with sin-
the energy dependency of the photoelectric With the development of DECT, material gle-energy CTA on the same scanner while
effect and the variability of K edges form differentiation becomes feasible, and the two still generating images of diagnostic qual-
the basis of DECT and can be used to detect consecutive scans can be replaced by one ity. Maximum-intensity-projection images
substances such as iodine and calcium [26]. scan. Use of this technique reduces the radi- obtained with dual-energy software allowed
DECT can be used for material differentia- ation dose, eliminates possible misregistra- a quick overview for detection of stenosis
tion based on atomic number. Differences be- tion artifacts, and saves postprocessing time. and aneurysms. However, the techniques
tween the K edge of iodine and that of calci- There have been few studies evaluating were prone to pitfalls in false-positive an-
um are used in the bone removal algorithm in DECT angiography of cranial and transcra- eurysm detection due to infundibuli and ve-
CTA. In comparison with calcium (Z = 20), nial vessels. To the best of our knowledge, all nous enhancement, as is in digital subtrac-
iodine has a higher atomic number (Z = 53) have been based on first-generation DECT. tion CTA. Stenoses tended to be overrated in
and therefore a greater K edge. Ma et al. [34] assessed the feasibility of du- DECT angiography. Hegde et al. concluded
Material quantification allows reconstruc- al-energy bone subtraction in cranial CTA in that the source images (mixed 140/80 kV)
tion of virtual unenhanced images in which a phantom model and in imaging of 36 pa- and triplanar reconstructions should be used
the iodine content is subtracted from the con- tients. They focused on image quality, time to confirm pathologic findings. With DECT
trast-enhanced images [27]. In three-material consumption, and radiation dose. Conven- angiography, misregistration artifacts due to
decomposition, concentrations of the ele- tional CTA was used as the standard of ref- patient motion between the unenhanced and
ments in the brain can be determined. Iodine erence. The investigators concluded that the enhanced phases of CTA cannot happen. The
has a high atomic number, whereas most postprocessing time and reading time with investigators noticed that most surgical clips
other tissues in the brain consist of elements
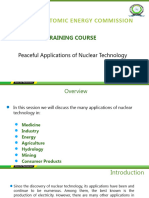
with a low atomic number. When two ma-
terials with low atomic numbers (e.g., brain Fig. 1—Diagram shows
that when two materials Iodine
parenchyma and blood) and different attenu- with low atomic
ation in a single energy spectrum are placed numbers, such as brain
in a diagram with one material with a high parenchyma and blood
from hemorrhage, and
atomic number (iodine), the algorithm can
Tube A Low Kilovoltage
different attenuation in
decompose a single voxel in a mixture of single energy spectrum Mixed
these three elements, and it becomes possible are placed in diagram
el
to calculate the contributions of iodine and with one material with
ox
high atomic number, for
tv
the tissue to the attenuation of the voxel (Fig.
en
example, iodine, algorithm
nt
1). This algorithm thus allows identification can decompose single
co
Hemorrhage
ne
and its quantification of the element with the voxel (mixed) in mixture
di
of these three elements.
Io
higher atomic number (iodine) [20, 28]. It then becomes possible
Hemorrhage content voxel
to calculate contribution
Parenchyma content voxel
Applications in Intracranial Vessels of iodine and tissue to
attenuation of this mixed Brain parenchyma
The standard of reference for the evaluation
voxel. (Modified with
of intracranial and transcranial blood vessels permission from Kim et Tube B High Kilovoltage
is digital subtraction angiography (DSA), 3D al. [21])
AJR:199, November 2012 S27
Postma et al.
were eliminated during DECT angiography beam-hardening artifacts around metallic ob- with suspected cerebrovascular disease and
subtraction, as in subtraction CTA. However, jects can hinder depiction of nearby vessels. compared the degree of stenosis found with
a few clips remained intact during bone re- Buerke et al. [37] performed DECT angi- DECT angiography and that found with time-
moval subtraction. As in conventional CTA, ography with a DSCT scanner for 50 patients of-flight MRA and conventional CTA in trans
cranial arteries. They found that the conven-
tional CTA and time-of-flight MRA findings
Downloaded from www.ajronline.org by 36.73.159.237 on 05/14/19 from IP address 36.73.159.237. Copyright ARRS. For personal use only; all rights reserved
were similar. However, with bone removal
DECT angiography, stenosis in close relation
to the skull base was overestimated, specif-
ically in the carotid canal (C2 segment), as
was calcified stenosis. This finding is partly
explained by the generation of blooming ar-
tifacts from the calcified plaques. These ar-
tifacts cause ill-defined borders, the conse-
quence of which is overestimation of stenosis.
Buerke et al. concluded that in DECT angiog-
raphy there is a risk of a false-positive finding
of stenosis in cases of close relation to bone or
calcification. They suggested that optimization
Fig. 2—55-year-old previously healthy woman with
confusion and drowsiness, left-sided hemorrhagic
lesion at brainstem, and obstructive hydrocephalus.
(All dual-source CT [DSCT] scans in this review
obtained with second-generation scanner [Somatom
Definition Flash, Siemens Healthcare]: tube A,
80 kV and 310 mAs; tube B, 140 kV and 155 mAs;
acquisition, 32 × 0.6 mm; collimation, 0.6 mm; pitch,
0.7; reconstruction slice thickness, 1 mm; increment,
0.7; D26 kernel; contrast administration of 110 mL
iopromide 300 [Ultravist, Bayer Schering Pharma]
with dual-head injector [Stellant, Medrad] at flow
rate of 7 mL/s followed by 50-mL saline flush at
same rate.) Lesion at mesencephalon at thinner
reconstructions is less pronounced compared with
true native image (B), having increased noise, but
is still of diagnostic quality at lower dose. Virtual
unenhanced image (F) shows residual attenuation in
veins, whereas enhancement from arterial vessels is
removed. With half dose of true native scan (effective
dose, 2.48 mSv), single dual-energy CT (DECT)
angiography (effective dose 0.97 mSv) provides
information about brain parenchyma, lesion, and
vessels with possibility of bone removal.
A, Single-energy reconstructions from circle of Willis
show that at lower reconstructed kilovoltage, there
is increased attenuation of vessels accompanied
by increase in noise. At higher reconstructed
kilovoltage, vessels nearly disappear. Conspicuity
of hemorrhagic lesion does not change in range of
60–150 kV. At lowest kilovoltage, decreased visibility
is probably due to noise.
B, True native CT image from referring hospital with
6-mm slice thickness shows high-attenuation lesion
at posterior left mesencephalon with obstructive
hydrocephalus. DECT angiography was performed to
identify underlying vascular pathologic mechanism.
C, DECT angiographic reconstruction of mixed image
with head kernel, 3-mm slice.
D, DECT angiographic reconstruction of mixed image
with soft head kernel, 3-mm slice.
E, Bone removal DECT angiographic reconstruction.
F, Virtual unenhanced DECT angiographic
reconstruction, 3-mm slice.
G, T2-weighted MR image shows hypointense
blooming at mesencephalon. Lesion was suspected
of being cavernoma.
S28 AJR:199, November 2012
Dual-Energy CT of the Brain and Intracranial Vessels
of demarcation algorithms and reconstruction
kernels could resolve this problem.
Watanabe et al. [38] compared DECT an-
giography and DSA of 12 patients with intra-
cranial aneurysms or internal carotid artery
stenosis. They concluded that DECT angi-
Downloaded from www.ajronline.org by 36.73.159.237 on 05/14/19 from IP address 36.73.159.237. Copyright ARRS. For personal use only; all rights reserved
ography was successful for evaluation of an-
eurysms and internal carotid artery stenosis
with a short calculation time and was com-
parable to DSA. They found that three aneu-
rysms near the skull base were fully visible
with DECT angiography but that only partial
visualization was achieved with convention-
al CTA. The stenoses tended to be overesti- Fig. 3—80-year-old man with dysarthria and right-sided paralysis but no stenosis or occlusion of middle
cerebral artery. Example of bone removal dual-energy CT (DECT) angiography without removal of calcified
mated with bone removal DECT angiogra- plaques.
phy compared with DSA, partially because A, DECT angiographic source image shows carotid arteries at cavernous sinus and calcified plaque at left
of the aforementioned blooming effect of carotid artery.
calcifications. Watanabe et al. concluded that B, Bone removal CT image shows that although bone has been removed, calcified plaque is still visible.
C, Volume-rendered bone removal DECT angiogram shows calcifications along carotid artery. Irregularities at
dual-energy bone removal CTA eliminated right-sided carotid artery suggest overestimation of bone of skull base.
bone and calcifications from CTA images
with only a single contrast-enhanced acqui-
sition and was a useful tool for evaluating in- DECT angiography was not statistically dif- tivity, 95.7%; specificity, 95%; positive pre-
tracranial aneurysms and stenosis. ferent from that of digital subtraction CTA, dictive value, 97.8%; negative predictive val-
Zhang et al. [39, 40] published two articles although the quality of vessel depiction near ue, 90.5%; accuracy, 95.5%) compared with
concentrating on detection of aneurysms in a the skull base seemed to decrease. This simi- the results for 3D DSA and not statistically
group of 80 patients. They compared DECT lar quality was conceived at a lower radiation different from those for conventional CTA.
angiography and digital subtraction CTA with dose with DECT angiography, being reduced As expected, these numbers increased in the
3D DSA and evaluated image quality, ra- 60% compared with the quality of digital sub- detection of aneurysms larger than 5 mm (all
diation dose, and the diagnostic accuracy of traction CTA. These investigators found high values, 100%). The authors concluded that
DECT angiography in the detection of intra- sensitivity and specificity in the detection of DECT angiography is comparable to conven-
cranial aneurysms. The image quality of the intracranial aneurysms (per-aneurysm sensi- tional CTA in the detection of intracranial an-
eurysms but at lower radiation cost.
With postprocessing of DECT angiogra-
phy, next to bone removal, single-energy im-
ages can be generated for better delineation
of the iodine content in a vessel because at
lower kilovoltage, iodine attenuation is high-
er than at higher kilovoltage (Fig. 2A). This
feature can be useful in CTA with lower dos-
es of contrast material [24]. To our knowl-
edge, no results concerning these applica-
tions have been published.
Fig. 4—72-year-old man with subarachnoid
hemorrhage due to ruptured aneurysm of anterior
communicating artery (ACoA). Surgical treatment
with clipping of aneurysm was performed. Dual-
energy CT (DECT) angiography was performed for
evaluation of treated aneurysm.
A, Source images at level of skull base show calcified
plaque at left-sided carotid artery.
B, Bone removal DECT angiogram, including plaque
removal, shows overestimation of calcified plaques at
both carotid arteries due to blooming of calcification.
C, Volume-rendered non–bone removal CT angiogram
shows presence of clip at ACoA.
D, Volume-rendered bone removal CT angiogram
clearly shows position of aneurysm clip at ACoA and
allows 360° inspection of region. Irregular borders of
carotid arteries are signs of excess removal of bone.
AJR:199, November 2012 S29
Postma et al.
dual-energy scan, as when a patient presents
with subarachnoid hemorrhage, unenhanced
CT can be omitted because of the possibility
of calculating a virtual unenhanced image. A
third application is identification of iodine in
an area of hemorrhage because it can be a clue
Downloaded from www.ajronline.org by 36.73.159.237 on 05/14/19 from IP address 36.73.159.237. Copyright ARRS. For personal use only; all rights reserved
to an underlying pathologic condition in pa-
tients with intracranial hemorrhage.
Hemorrhagic transformation is one of the
major complications after intraarterial re-
canalization in stroke patients. Identification
of hemorrhage after intraarterial recanaliza-
tion therefore is important, but it is difficult
with conventional CT, as found by Kim et al.
[41]. Some authors [42, 43] have advocated
measuring attenuation to predict hemorrhag-
ic transformation. The higher the attenuation
of lesions at conventional CT immediately
after intraarterial recanalization, the great-
er is the probability of hemorrhagic transfor-
mation at follow-up. Yoon et al. [43] found
that areas with attenuation greater than 90
HU may be associated with parenchymal
hemorrhage. However, predicting hemor-
rhagic foci or hemorrhagic transformation
Fig. 5—53-year-old woman with sudden onset of headache due to subarachnoid hemorrhage.
A, True native CT image shows subarachnoid hemorrhage in basal cisterns. Mild hydrocephalus with dilated solely based on attenuation is nearly impos-
temporal horns is evident. sible [41]. DECT has been introduced for dif-
B, Bone removal dual-energy CT (DECT) angiogram shows small aneurysm of anterior communicating artery ferentiation of contrast material and blood in
(ACoA).
C, Volume-rendered bone removal DECT angiogram shows small aneurysm of ACoA and irregularity of carotid the brain [20, 22, 23].
arteries at segments at level of skull base suggestive of overestimation of surrounding bone. Gupta et al. [22] analyzed 28 intraparen-
D, Virtual unenhanced image reconstructed from DECT angiogram shows subarachnoid hemorrhage in basal chymal areas of high attenuation at CT af-
cisterns at slightly increased noise level compared with A.
E, Iodine overlay image shows enhancing vessels without density of surrounding hemorrhage.
ter administration of an iodinated contrast
F, Volume-rendered 3D digital subtraction angiogram shows ACoA aneurysm with exact outlines and agent to 15 patients. Twelve of these pa-
relationship to parent vessel. tients received the contrast agent soon after
they underwent intraarterial recanalization,
In summary, studies have shown good im- there being some benefit for DECT angiog- one patient after carotid stent placement,
age quality for DECT angiography of intra- raphy in the detection of aneurysms adjacent and two for further evaluation of intracra-
cranial vessels, but imaging of arteries at the to the skull base (Fig. 5). A major advantage nial hemorrhage. Twenty lesions were clas-
level of the skull base remains problemat- of DECT angiography is the substantial radi- sified at DECT as contrast material, five as
ic for selective visualization and is prone to ation dose reduction compared with the dose blood, and three as both contrast material
overestimation of the grade of stenosis. Cal- for conventional (subtraction) CTA. This fac- and blood. The sensitivity for identification
cified plaques can also cause problems in tor is especially important with the increasing of hemorrhage, compared with 24-hour fol-
grading of stenosis. Dual-energy software, awareness of radiation burden. low-up CT, was 100%, the specificity was
however, has the advantage of allowing op- 91%, and the accuracy was 93%.
tional subtraction of calcified plaques and Applications in the Brain Phan et al. [23] reported on the use of
thus optimal assessment of the vascular lu- Next to bone removal algorithms, differ- DECT in a group of 40 patients. Eighteen of
men (Figs. 3 and 4). entiation between blood present from hemor- the patients had undergone intraarterial recan-
The dual-energy software allows fast pro- rhage and iodine is a potential application of alization, and the others were evaluated for
cessing in the way that maximum-intensity- DECT (Figs. 2B–2G, 6, and 7). Whereas in carotid stenosis, trauma, or tumors. The in-
projection reconstructions of the vessels allow conventional CT, iodine and blood typically vestigators evaluated a total of 148 foci of in-
quick overview and identification of segments have similar attenuation, these substances can tracranial high attenuation. Of these, 142 foci
with possible stenosis. As in conventional be differentiated with dual-energy algorithms. were correctly classified as hemorrhage with
(subtraction) CTA, the source images should This capability can be useful for imaging of DECT and confirmed with follow-up CT or
by all means be taken into account with mul- patients who have received iodinated contrast MRI. The sensitivity, specificity, and accura-
tiplanar reformation and volume-rendered re- material before admission for CT, such as pa- cy in identification of hemorrhage, depending
construction as additional options. tients who have undergone coronary angiog- on the parenchymal, intraventricular, or sub-
Detection of aneurysms with DECT angi- raphy or intraarterial recanalization. For im- arachnoid compartment, were 100%, 84.4–
ography is as good as with conventional CTA, mediate acquisition of a contrast-enhanced 100%, and 87.2–100%.
S30 AJR:199, November 2012
Dual-Energy CT of the Brain and Intracranial Vessels
Ferda et al. [20] assessed the use of DECT includes virtual unenhanced reconstruction, nial hemorrhage without a definite underlying
angiography in the detection of intracranial radiation burden to the patient can be reduced cause. They calculated virtual unenhanced im-
hemorrhage on the virtual unenhanced images and diagnostic efficacy retained. ages, iodine overlay images, and fusion imag-
of 25 patients with subarachnoid hemorrhage Analysis of the underlying pathologic mech- es (Fig. 8). The sensitivity and specificity for
diagnosed on the basis of the finding of intra- anism in patients with intracranial hemor- the detection of underlying brain tumor were
cranial bleeding on unenhanced CT images. rhage is performed with contrast-enhanced 94.4% and 97.4%. These values are signifi-
Downloaded from www.ajronline.org by 36.73.159.237 on 05/14/19 from IP address 36.73.159.237. Copyright ARRS. For personal use only; all rights reserved
They rated the quality of the virtual unenhanced CT or MRI. Both techniques have limita- cantly higher than for conventional unenhanced
images as excellent for 13 patients and suffi- tions. The high signal intensity of areas of imaging (66.7%, 89.7%) and combined con-
cient for 12 patients. Although the image qual- hemorrhage on T1-weighted MR images trast-enhanced and conventional unenhanced
ity was slightly lower than that of conventional makes it difficult to differentiate blood from imaging (61.1%, 92.3%). The areas under the
CT, all images were of diagnostic quality. The gadolinium contrast material. On CT imag- receiver operating characteristic curves were
agreement between virtual unenhanced images es, hematomas and areas of iodine enhance- 0.964, 0.786, and 0.842. Image noise was high-
and conventional CT images in the detection of ment have high attenuation. er on virtual unenhanced images than on true
intracranial hemorrhage was 96% in per-lesion Kim et al. [21] used DECT in the evaluation unenhanced images, with lower attenuation of
and 100% in per-patient analysis. The investi- of intracerebral hemorrhage of unknown origin. the hematomas, but was not rated differently at
gators concluded that by replacing convention- They used arterial and venous phase DECT to visual assessment. All hematomas were identi-
al CT and CTA with DECT angiography that analyze the cases of 56 patients with intracra- fied on virtual unenhanced images.
Fig. 6—44-year-old man with right-sided paralysis due to occlusion of left middle Fig. 7—63-year-old man found unresponsive with dilated pupils and referred
cerebral artery. Dual-energy CT was performed immediately after successful to hospital. CT angiography showed basilar artery occlusion, and patient was
intraarterial thrombectomy of left middle cerebral artery. transferred to intervention unit. Immediately after successful recanalization, dual-
A, Mixed image (comparable to conventional CT image) shows area of high energy CT was performed.
attenuation in lentiform nucleus. A, Mixed image (comparable to conventional CT) shows bilateral areas of high
B, Iodine overlay image suggests high attenuation is caused by iodinated contrast attenuation in medial thalami corresponding to distribution area of artery of
material. Calcifications, in this case calcification of choroid plexus, are visible on Percheron.
iodine overlay images. B, Iodine overlay image suggests area of high attenuation is iodinated contrast
C, Virtual unenhanced image shows absence of attenuation, with lower material. Pineal gland calcification also is evident.
attenuation in lentiform nucleus, suggestive of ischemia without hemorrhagic C, Virtual unenhanced image suggests absence of hemorrhage.
focus. D, Follow-up conventional CT image 24 hours after A–C shows small left-
D, Follow-up conventional CT image 24 hours after A–C confirms absence of sided hemorrhagic focus in bilateral thalamic infarcts just lateral to area of
hemorrhage and presence of small infarct. enhancement on first scan, suggestive of hemorrhagic transformation.
AJR:199, November 2012 S31
Postma et al.
Fig. 8—42-year-old previously healthy man who had
transient dysphasia at referring hospital.
A, True native CT scan shows high-attenuation lesion
with small surrounding border of low attenuation.
B, T2-weighted MR image shows susceptibility
artifacts in and around lesion.
C and D, T1-weighted images without (C) and with
(D) gadolinium enhancement do not show underlying
Downloaded from www.ajronline.org by 36.73.159.237 on 05/14/19 from IP address 36.73.159.237. Copyright ARRS. For personal use only; all rights reserved
enhancing pathologic features. Cavernoma was
suspected because of demographic features and
absence of visible lesion. DECT angiography was
offered when patient arrived at our hospital.
E–H, Reconstructed mixed (E), virtual unenhanced
(F), iodine overlay (G), and volume-rendered bone
removal (H) CT angiograms 2 weeks after initial
presentation show increasing surrounding edema
and partially resolving hematoma in E and F. Small
focus of enhancement is evident at lateral side of
lesion without obvious vessel abnormality.
I–L, Reconstructed mixed (I), virtual unenhanced
(J), iodine overlay (K), and fusion images (virtual
unenhanced and iodine overlay) (L) DECT images
obtained at 90 seconds show ring-enhancing lesion
with signet ring appearance. Underlying malignancy
was expected. At workup, melanoma of foot was
found and was considered primary tumor. Arterial
and late phase virtual unenhanced images show
comparable density of resorbing blood. Dose for
dual-energy CT (DECT) angiography and late DECT
together was estimated to be 2.27 mSv, slightly
higher than for conventional CT (2.2 mSv) but with
increased amount of information. DECT in venous
phase with single-energy reconstruction of arterial
vessels might have eliminated need for DECT
angiography, further reducing dose.
Kim et al. [21] concluded that DECT with velopment of better reconstruction algorithms 2. Brooks RA. A quantitative theory of the Houns-
CTA seems an ideal tool in the evaluation and dedicated dual-energy kernels may offer a field unit and its application to dual energy scan-
of patients with intracranial hemorrhage in solution. Detection and follow-up of treated ning. J Comput Assist Tomogr 1977; 1:487–493
the acute stage. Through DECT angiograph- aneurysms are reliable. The role of DECT in 3. Flohr TG, McCollough CH, Bruder H, et al. First
ic bone removal evaluation of the vessels and detection of hemorrhage on contrast-enhanced performance evaluation of a dual-source CT
calculation of virtual unenhanced images, io- CT scans and analysis of the underlying patho- (DSCT) system. Eur Radiol 2006; 16:256–268
dine overlay and fusion images for tumor eval- logic mechanism of hematomas is promising. 4. Matsumoto K, Jinzaki M, Tanami Y, Ueno A, Yamada
uation can be obtained from the same source Instead of waiting for resolution of the hemato- M, Kuribayashi S. Virtual monochromatic spec-
images. Kim et al. suggest replacing true un- ma, early diagnosis of the underlying patholog- tral imaging with fast kilovoltage switching: im-
enhanced CT of patients with known intracra- ic changes may be possible, and treatment can proved image quality as compared with that ob-
nial hemorrhage with virtual unenhanced CT be started earlier. In stroke patients, early dif- tained with conventional 120-kVp CT. Radiology
to reduce the radiation dose. In their patient ferentiation between iodine and blood allows 2011; 259:257–262
group, the dose for DECT was 1 mSv, compa- identification of the risk of hemorrhagic trans- 5. Roessl E, Herrmann C, Kraft E, Proksa R. A com-
rable to that of conventional CTA. formation and gives further insight into this parative study of a dual-energy-like imaging tech-
The results of these studies suggest a useful phenomenon. The low radiation dose in DECT nique based on counting-integrating readout. Med
contribution of DECT for both the detection and the large range of possible reconstructions Phys 2011; 38:6416–6428
of hemorrhage with contrast-enhanced CT and from one dataset justify further investigation of 6. Vrtiska TJ, Takahashi N, Fletcher JG, Hartman RP,
for the detection of the underlying pathologic DECT in neuroradiology and the development Yu L, Kawashima A. Genitourinary applications of
condition. Use of DECT may resolve impor- of dedicated algorithms. If DECT is available dual-energy CT. AJR 2010; 194:1434–1442
tant diagnostic problems in neuroradiology. at a hospital, the use of this technique should 7. Takahashi N, Vrtiska TJ, Kawashima A, et al. De-
be expanded, not only for cardiac, skeletal, ab- tectability of urinary stones on virtual nonen-
Conclusion dominal, and thoracic applications but also for hanced images generated at pyelographic-phase
Although DECT of the brain and intracra- neuroradiologic practice, because it may play dual-energy CT. Radiology 2010; 256:184–190
nial vessels has not been widely implemented an important role in solving diagnostic chal- 8. Chae EJ, Song JW, Krauss B, et al. Dual-energy
and studied, it has great potential in neurora- lenges in neuroradiology. computed tomography characterization of soli-
diology. Bone removal in DECT angiography tary pulmonary nodules. J Thorac Imaging 2010;
allows easier and faster acquisition and post- References 25:301–310
processing compared with conventional (sub- 1. Leeds NE, Kieffer SA. Evolution of diagnostic 9. Kim BH, Seo JB, Chae EJ, Lee HJ, Hwang HJ,
traction) CTA. Removal of bone at the skull neuroradiology from 1904 to 1999. Radiology Lim C. Analysis of perfusion defects by causes
base remains a matter of concern, but the de- 2000; 217:309–318 other than acute pulmonary thromboembolism on
S32 AJR:199, November 2012
Dual-Energy CT of the Brain and Intracranial Vessels
contrast-enhanced dual-energy CT in consecutive phy. Eur Radiol 2009; 19:2518–2522 33. Romijn M, Gratama van Andel HA, van
537 patients. Eur J Radiol 2012; 81:e647–e652 21. Kim SJ, Lim HK, Lee HY, et al. Dual-energy CT Walderveen MA, et al. Diagnostic accuracy of CT
10. Kim JE, Lee JM, Baek JH, Han JK, Choi BI. Ini- in the evaluation of intracerebral hemorrhage of angiography with matched mask bone elimination
tial assessment of dual-energy CT in patients with unknown origin: differentiation between tumor for detection of intracranial aneurysms: compari-
gallstones or bile duct stones: can virtual nonen- bleeding and pure hemorrhage. AJNR 2012; son with digital subtraction angiography and 3D
hanced images replace true nonenhanced images? 33:865–872 rotational angiography. AJNR 2008; 29:134–139
Downloaded from www.ajronline.org by 36.73.159.237 on 05/14/19 from IP address 36.73.159.237. Copyright ARRS. For personal use only; all rights reserved
AJR 2012; 198:817–824 22. Gupta R, Phan CM, Leidecker C, et al. Evaluation 34. Ma R, Liu C, Deng K, Song SJ, Wang DP, Huang
11. Kang DK, Schoepf UJ, Bastarrika G, Nance JW Jr, of dual-energy CT for differentiating intracere- L. Cerebral artery evaluation of dual energy CT
Abro JA, Ruzsics B. Dual-energy computed to- bral hemorrhage from iodinated contrast material angiography with dual source CT. Chin Med J
mography for integrative imaging of coronary ar- staining. Radiology 2010; 257:205–211 (Engl) 2010; 123:1139–1144
tery disease: principles and clinical applications. 23. Phan CM, Yoo AJ, Hirsch JA, Nogueira RG, 35. Mühlenbruch G, Das M, Mommertz G, et al.
Semin Ultrasound CT MR 2010; 31:276–291 Gupta R. Differentiation of hemorrhage from io- Comparison of dual-source CT angiography and
12. Kaza RK, Caoili EM, Cohan RH, Platt JF. Distin- dinated contrast in different intracranial compart- MR angiography in preoperative evaluation of in-
guishing enhancing from nonenhancing renal le- ments using dual-energy head CT. AJNR 2012; tra- and extracranial vessels: a pilot study. Eur
sions with fast kilovoltage-switching dual-energy 33:1088–1094 Radiol 2010; 20:469–476
CT. AJR 2011; 197:1375–1381 24. Rapalino OK, Gupta R, Phan C, et al. Neurological 36. Hegde A, Chan LL, Tan L, Illyyas M, Lim WE.
13. Ko SM, Choi JW, Song MG, et al. Myocardial applications. In: Johnson T, Fink C, Schönberg SO, Dual energy CT and its use in neuroangiography.
perfusion imaging using adenosine-induced stress Reiser MF, eds. Dual energy CT in clinical practice. Ann Acad Med Singapore 2009; 38:817–820
dual-energy computed tomography of the heart: Berlin, Germany: Springer-Verlag, 2011:127–142 37. Buerke B, Wittkamp G, Seifarth H, Heindel W,
comparison with cardiac magnetic resonance im- 25. Huda WS. Review of radiological physics. Phila- Kloska SP. Dual-energy CTA with bone removal
aging and conventional coronary angiography. delphia, PA: Lippincott Williams & Wilkins, for transcranial arteries: intraindividual compari-
Eur Radiol 2011; 21:26–35 2003 son with standard CTA without bone removal and
14. Nance JW Jr, Bastarrika G, Kang DK, et al. High- 26. Coursey CA, Nelson RC, Boll DT, et al. Dual-en- TOF-MRA. Acad Radiol 2009; 16:1348–1355
temporal resolution dual-energy computed to- ergy multidetector CT: how does it work, what can 38. Watanabe Y, Uotani K, Nakazawa T, et al. Dual-
mography of the heart using a novel hybrid image it tell us, and when can we use it in abdominopel- energy direct bone removal CT angiography for
reconstruction algorithm: initial experience. J vic imaging? RadioGraphics 2010; 30:1037–1055 evaluation of intracranial aneurysm or stenosis:
Comput Assist Tomogr 2011; 35:119–125 27. Mahgerefteh S, Blachar A, Fraifeld S, Sosna J. comparison with conventional digital subtraction
15. Schenzle JC, Sommer WH, Neumaier K, et al. Dual-energy derived virtual nonenhanced com- angiography. Eur Radiol 2009; 19:1019–1024
Dual energy CT of the chest: how about the dose? puted tomography imaging: current status and ap- 39. Zhang LJ, Wu SY, Niu JB, et al. Dual-energy CT
Invest Radiol 2010; 45:347–353 plications. Semin Ultrasound CT MR 2010; angiography in the evaluation of intracranial an-
16. Karçaaltıncaba M, Aktaş A. Dual-energy CT re- 31:321–327 eurysms: image quality, radiation dose, and com-
visited with multidetector CT: review of princi- 28. Fornaro J, Leschka S, Hibbeln D, et al. Dual- and parison with 3D rotational digital subtraction an-
ples and clinical applications. Diagn Interv Radi- multi-energy CT: approach to functional imaging. giography. AJR 2010; 194:23–30
ol 2011; 17:181–194 Insights Imaging 2011; 2:149–159 40. Zhang LJ, Wu SY, Poon CS, et al. Automatic bone
17. Johnson TR, Krauss B, Sedlmair M, et al. Mate- 29. Forsting M. CTA of the ICA bifurcation and intra- removal dual-energy CT angiography for the eval-
rial differentiation by dual energy CT: initial ex- cranial vessels. Eur Radiol 2005; 15(suppl 4):D25– uation of intracranial aneurysms. J Comput Assist
perience. Eur Radiol 2007; 17:1510–1517 D27 Tomogr 2010; 34:816–824
18. Paul J, Bauer RW, Maentele W, Vogl TJ. Image 30. Westerlaan HE, Gravendeel J, Fiore D, et al. Multi- 41. Kim JT, Heo SH, Cho BH, et al. Hyperdensity on
fusion in dual energy computed tomography for slice CT angiography in the selection of patients with non-contrast CT immediately after intra-arterial
detection of various anatomic structures: effect on ruptured intracranial aneurysms suitable for clipping revascularization. J Neurol 2012; 259:936–943
contrast enhancement, contrast-to-noise ratio, or coiling. Neuroradiology 2007; 49:997–1007 42. Jang YM, Lee DH, Kim HS, et al. The fate of
signal-to-noise ratio and image quality. Eur J Ra- 31. Lell MM, Ruehm SG, Kramer M, et al. Cranial high-density lesions on the non-contrast CT ob-
diol 2011; 80:612–619 computed tomography angiography with auto- tained immediately after intra-arterial thromboly-
19. Tawfik AM, Kerl JM, Razek AA, et al. Image mated bone subtraction: a feasibility study. Invest sis in ischemic stroke patients. Korean J Radiol
quality and radiation dose of dual-energy CT of Radiol 2009; 44:38–43 2006; 7:221–228
the head and neck compared with a standard 120- 32. Morhard D, Fink C, Becker C, Reiser MF, Nikolaou 43. Yoon W, Seo JJ, Kim JK, Cho KH, Park JG, Kang
kVp acquisition. AJNR 2011; 32:1994–1999 K. Value of automatic bone subtraction in cranial HK. Contrast enhancement and contrast extrava-
20. Ferda J, Novak M, Mirka H, et al. The assessment CT angiography: comparison of bone-subtracted sation on computed tomography after intra-arteri-
of intracranial bleeding with virtual unenhanced vs. standard CT angiography in 100 patients. Eur al thrombolysis in patients with acute ischemic
imaging by means of dual-energy CT angiogra- Radiol 2008; 18:974–982 stroke. Stroke 2004; 35:876–881
AJR:199, November 2012 S33
Вам также может понравиться
- Lung Nodule Detection by Microdose CT Versus Chest RadiographyДокумент9 страницLung Nodule Detection by Microdose CT Versus Chest RadiographyTatiana RecinosОценок пока нет
- Pediatric Cardiac-Gated CT Angiography: Assessment of Radiation DoseДокумент7 страницPediatric Cardiac-Gated CT Angiography: Assessment of Radiation DoseDimas PramujaОценок пока нет
- Ajr Dect PDFДокумент11 страницAjr Dect PDFTom PatrickОценок пока нет
- Radiology of Chest Wall MassesДокумент11 страницRadiology of Chest Wall MassesDevina BumiОценок пока нет
- Ehjci Jeu155Документ1 страницаEhjci Jeu155adssaОценок пока нет
- Christensen Et Al 2012 Characterization of The Solitary Pulmonary Nodule 18f FDG Pet Versus Nodule Enhancement CTДокумент7 страницChristensen Et Al 2012 Characterization of The Solitary Pulmonary Nodule 18f FDG Pet Versus Nodule Enhancement CTLeticia PortilloОценок пока нет
- Eye Lens Dose During CT ExamДокумент7 страницEye Lens Dose During CT ExamSamu SimamesaОценок пока нет
- CTA ExtremityДокумент8 страницCTA Extremityrio trisonaОценок пока нет
- Clear Cell Renal Cell Carcinoma: Associations Between CT Features and Patient SurvivalДокумент8 страницClear Cell Renal Cell Carcinoma: Associations Between CT Features and Patient SurvivalBastian VizcarraОценок пока нет
- Rahayuddin 2019 J. Phys. Conf. Ser. 1341 082030Документ7 страницRahayuddin 2019 J. Phys. Conf. Ser. 1341 082030Saikat NandyОценок пока нет
- Cap 4Документ23 страницыCap 4Said UstaranОценок пока нет
- Comparative Analysis of Radiation Dose and Image Quality BetweenДокумент5 страницComparative Analysis of Radiation Dose and Image Quality BetweenIshani Anushika JayakodyОценок пока нет
- Pyakillya 2017 J. Phys. Conf. Ser. 913 012004Документ6 страницPyakillya 2017 J. Phys. Conf. Ser. 913 012004Mhd rdbОценок пока нет
- Intracranial NeoplasiaДокумент12 страницIntracranial NeoplasiaJamille OliveiraОценок пока нет
- El Valor Diagnostico de La Neuroimagen en DemenciaДокумент22 страницыEl Valor Diagnostico de La Neuroimagen en Demenciajhoel cruzОценок пока нет
- 2015-Accuracy of Subthalamic Nucleus Targeting by T2, FLAIRДокумент8 страниц2015-Accuracy of Subthalamic Nucleus Targeting by T2, FLAIRPaul RodrigoОценок пока нет
- JNMT-2004-Seibert-X-ray Part 1Документ10 страницJNMT-2004-Seibert-X-ray Part 1Martin HaarbyeОценок пока нет
- Johnson Et Al 2017 MDCT Angiography With 3d Rendering A Novel Cinematic Rendering Algorithm For Enhanced Anatomic DetailДокумент8 страницJohnson Et Al 2017 MDCT Angiography With 3d Rendering A Novel Cinematic Rendering Algorithm For Enhanced Anatomic Detailtituandreescu6810Оценок пока нет
- Matulanya - Applications of Nuclear TechnologyДокумент75 страницMatulanya - Applications of Nuclear TechnologyFlavioMuhaleОценок пока нет
- Breast CancerДокумент11 страницBreast CancerAnonymous 8vwJIhUy4Оценок пока нет
- Resonancia Magnetica en Animales de CompañíaДокумент11 страницResonancia Magnetica en Animales de CompañíaEnrique A. Vega NuñezОценок пока нет
- PSY115 - Activity 2.1Документ1 страницаPSY115 - Activity 2.1Darren Daniel InfanteОценок пока нет
- Radiotherapy and Oncology: EPTN ConsensusДокумент7 страницRadiotherapy and Oncology: EPTN ConsensusnotallowedОценок пока нет
- C P P C P P: Ardiology Atient AGE Ardiology Atient AGEДокумент3 страницыC P P C P P: Ardiology Atient AGE Ardiology Atient AGEBBA MaryamОценок пока нет
- nnm.10.104Документ8 страницnnm.10.104biswarupmandal0104Оценок пока нет
- Introduction To Radiology IIДокумент5 страницIntroduction To Radiology IIYousif AhmedОценок пока нет
- Subchondroplasty What TheДокумент6 страницSubchondroplasty What TheikhsanОценок пока нет
- The Role Nuclear Medicine Diagnostics in Brain DiseaseДокумент33 страницыThe Role Nuclear Medicine Diagnostics in Brain DiseaseMasryani Sylviana ManurungОценок пока нет
- Assignment 2: Mri MachineДокумент6 страницAssignment 2: Mri MachineMuhammad WajahatОценок пока нет
- Fusion 9.2.3.1 PDFДокумент6 страницFusion 9.2.3.1 PDFGowri ShankarОценок пока нет
- IMRT: A Review and Preview: Physics in Medicine & BiologyДокумент18 страницIMRT: A Review and Preview: Physics in Medicine & BiologychatsashОценок пока нет
- Ajr 2Документ10 страницAjr 2Fika FathiaОценок пока нет
- Pulmonary Embolism in Children: Paul G. Thacker Edward Y. LeeДокумент11 страницPulmonary Embolism in Children: Paul G. Thacker Edward Y. LeeYuriansyah Dwi Rahma PutraОценок пока нет
- 92 FullДокумент5 страниц92 FullROHITОценок пока нет
- Recent Advances in Magnetic Resonance Imaging For Stroke DiagnosisДокумент12 страницRecent Advances in Magnetic Resonance Imaging For Stroke DiagnosisMarsella Epifania SuwignyoОценок пока нет
- Intraarterial Heparin Flushing Effect On Motor Evoked Potentials in Chronic Ischemic Stroke PatientsДокумент5 страницIntraarterial Heparin Flushing Effect On Motor Evoked Potentials in Chronic Ischemic Stroke PatientstranОценок пока нет
- Lens Dose in Routine Head CTДокумент8 страницLens Dose in Routine Head CTAglaia T.Оценок пока нет
- OTO NOVEMBER 2018 Value of SPECT CT For Sentinel LymphДокумент5 страницOTO NOVEMBER 2018 Value of SPECT CT For Sentinel LymphГаянэ АллахвердянОценок пока нет
- Intra-Axial Brain TumorsДокумент18 страницIntra-Axial Brain Tumorsputu risyaОценок пока нет
- Radiol 2018172656Документ20 страницRadiol 2018172656rnjОценок пока нет
- Image SegmentationДокумент3 страницыImage SegmentationrajasekarОценок пока нет
- J Jacc 2021 06 019Документ24 страницыJ Jacc 2021 06 019Jesús MorenoОценок пока нет
- ABC of TDCS in Stroke PatientsДокумент7 страницABC of TDCS in Stroke PatientslabsoneducationОценок пока нет
- Effect of Patient Size On Radiation Dose of Abdominal MDCT With Automatic Tube Current ModulationДокумент6 страницEffect of Patient Size On Radiation Dose of Abdominal MDCT With Automatic Tube Current Modulationdestian ryanОценок пока нет
- Art. Y Souza - Correspondence of Microelectrode Mapping With Magnetic Resonance Imaging For Subthalamic Nucleus ProceduresДокумент5 страницArt. Y Souza - Correspondence of Microelectrode Mapping With Magnetic Resonance Imaging For Subthalamic Nucleus ProceduresEstereotaxia BrasilОценок пока нет
- Pet BrochureДокумент20 страницPet BrochureSheikh Hasnain AliОценок пока нет
- Deep Learning For Hemorrhagic Lesion Detection and Segmentation On Brain CT ImagesДокумент13 страницDeep Learning For Hemorrhagic Lesion Detection and Segmentation On Brain CT Imagesakib mahmudОценок пока нет
- Ajr 09 4032Документ7 страницAjr 09 4032Roshi_11Оценок пока нет
- Differentiation of True Progression From Pseudoprogression With Quantitative Dynamic Contrast-Enhanced MR ImagingДокумент11 страницDifferentiation of True Progression From Pseudoprogression With Quantitative Dynamic Contrast-Enhanced MR ImagingFernando TeixeiraОценок пока нет
- Defeito Craniano Tdcs TbiДокумент19 страницDefeito Craniano Tdcs TbiAmandavictooriaОценок пока нет
- Predicting CT Image From MRI Data Through Feature Matching With Learned Nonlinear Local DescriptorsДокумент11 страницPredicting CT Image From MRI Data Through Feature Matching With Learned Nonlinear Local DescriptorsAОценок пока нет
- Maspero 2017 Phys. Med. Biol. 62 948Документ19 страницMaspero 2017 Phys. Med. Biol. 62 948Jenna WuОценок пока нет
- 1 The Role of Computed Tomography As A Prognostic Tool in Traumatic Brain Trauma - Imaging in MedicineДокумент8 страниц1 The Role of Computed Tomography As A Prognostic Tool in Traumatic Brain Trauma - Imaging in Medicinecral1124Оценок пока нет
- Masas Cardiacas Parte 1 PMC 2015Документ13 страницMasas Cardiacas Parte 1 PMC 2015Diego Andrés Mejía VascoОценок пока нет
- Matsumoto 2016Документ7 страницMatsumoto 2016A DОценок пока нет
- Shamir 2018Документ9 страницShamir 2018Victor Hugo OrtizОценок пока нет
- Interpretasi CT ScanДокумент19 страницInterpretasi CT ScanAB KristiadiОценок пока нет
- Computed-Tomography a Powerful Tool for Diagnosis of Pediatric and Adult Congenital Heart Disease: Methodology and Interpretation GuideОт EverandComputed-Tomography a Powerful Tool for Diagnosis of Pediatric and Adult Congenital Heart Disease: Methodology and Interpretation GuideОценок пока нет
- Diagnostic Imaging Pathways Article PDFДокумент12 страницDiagnostic Imaging Pathways Article PDFchald ald smithОценок пока нет
- Bronchial and Arterial Sleeve Resection For Centrally-Located Lung CancersДокумент10 страницBronchial and Arterial Sleeve Resection For Centrally-Located Lung CancersJovelyn SagangОценок пока нет
- CT ScanДокумент4 страницыCT Scant a khanОценок пока нет
- Clinical Cases: World Journal ofДокумент16 страницClinical Cases: World Journal ofRhotmy Raúl Escobar GuzmánОценок пока нет
- Design of Prosthetic ArmДокумент8 страницDesign of Prosthetic Armranganath lollaОценок пока нет
- Uk Cancer de PanceasДокумент9 страницUk Cancer de PanceasBety Puma PauccaraОценок пока нет
- Pitfalls, Problems, and Progress in Bronchopulmonary DysplasiaДокумент14 страницPitfalls, Problems, and Progress in Bronchopulmonary Dysplasiatrixie2k7Оценок пока нет
- Pemeriksaan Radiologi Pada Trauma GinjalДокумент21 страницаPemeriksaan Radiologi Pada Trauma GinjalQotrunnada Alwi Zubaidah, S.KedОценок пока нет
- The Egyptian Journal of Radiology and Nuclear MedicineДокумент6 страницThe Egyptian Journal of Radiology and Nuclear MedicineOctavianusОценок пока нет
- Role of Radiology in Forensic Dentistry PDFДокумент3 страницыRole of Radiology in Forensic Dentistry PDFMeris JugadorОценок пока нет
- HISPEED CTE DUAL ManualДокумент10 страницHISPEED CTE DUAL ManualMOHIT PRADHANОценок пока нет
- Mai and Kantzas - 2002 - An Evaluation of The Application of Low Field NMR in The Characterization of Carbonate ReservoirsДокумент9 страницMai and Kantzas - 2002 - An Evaluation of The Application of Low Field NMR in The Characterization of Carbonate ReservoirsLorena Pastana MartinsОценок пока нет
- Elbow PainДокумент9 страницElbow PainRhomadhoni Ika PutraОценок пока нет
- Aprildhardmanresume2021 DosimetryДокумент3 страницыAprildhardmanresume2021 Dosimetryapi-529438966Оценок пока нет
- A10440681S419Документ9 страницA10440681S419Harshini MОценок пока нет
- Post-Operative Complications of Craniotomy and CraniectomyДокумент9 страницPost-Operative Complications of Craniotomy and CraniectomyLusy Octavia SaputriОценок пока нет
- Code Medical Imaging Techniques L T P CДокумент3 страницыCode Medical Imaging Techniques L T P Csridharchandrasekar100% (1)
- Accmm2 19Документ4 страницыAccmm2 19lmplmpОценок пока нет
- Surgeon-Performed Ultrasound As A Diagnostic Tool in AppendicitisДокумент6 страницSurgeon-Performed Ultrasound As A Diagnostic Tool in Appendicitisansar ahmedОценок пока нет
- Computed Tomography: Case Histories of Significant Medical AdvancesДокумент19 страницComputed Tomography: Case Histories of Significant Medical AdvancesVíctor Arturo Sipán RiveraОценок пока нет
- Lung Cancer ScreeningДокумент17 страницLung Cancer ScreeningNguyen Minh DucОценок пока нет
- Radiology Request FormДокумент2 страницыRadiology Request FormCoco Choi0% (2)
- Absolute Neurocritical Care Review 2017Документ252 страницыAbsolute Neurocritical Care Review 2017Luis Muñoz ChaccОценок пока нет
- True PDFДокумент459 страницTrue PDFAmna MmfОценок пока нет
- 10 1109@iccsp48568 2020 9182258Документ4 страницы10 1109@iccsp48568 2020 9182258mindaОценок пока нет
- European Journal of Radiology: SciencedirectДокумент7 страницEuropean Journal of Radiology: SciencedirectfhiraОценок пока нет
- IMM Feb 2023-1Документ4 страницыIMM Feb 2023-1Ahmed NadeemОценок пока нет
- Principles and Practice of Emergency NeurologyДокумент456 страницPrinciples and Practice of Emergency NeurologyElfan Winoto100% (9)
- GE128 - Revolution EVO EL Data SheetДокумент14 страницGE128 - Revolution EVO EL Data SheetDiep tuan DungОценок пока нет
- Aquilion Lightning NewДокумент2 страницыAquilion Lightning NewIan Bruno Rodriguez Centurion100% (1)