Вам также может понравиться
- FxClavícula PDFДокумент7 страницFxClavícula PDFPenélope CrespoОценок пока нет
- FX Pelvic Rim Injury17Документ8 страницFX Pelvic Rim Injury17Antonio PáezОценок пока нет
- Complex Elbow InstabilityДокумент9 страницComplex Elbow InstabilityAristoteles Plato SocratesОценок пока нет
- Midshaft Clavicle Fractures AДокумент9 страницMidshaft Clavicle Fractures AFreddyChandraNainggolanОценок пока нет
- Current Concepts Tibial Plateau FXДокумент14 страницCurrent Concepts Tibial Plateau FXOrtho 20172100% (1)
- Current Concepts in Elbow Fracture Dislocation: Adam C Watts, Jagwant Singh, Michael Elvey and Zaid HamoodiДокумент8 страницCurrent Concepts in Elbow Fracture Dislocation: Adam C Watts, Jagwant Singh, Michael Elvey and Zaid HamoodiJoão Artur BonadimanОценок пока нет
- 2008 - Elbow Dislocation - OCNAДокумент7 страниц2008 - Elbow Dislocation - OCNAharpreet singhОценок пока нет
- Elbow Fractures: Distal Humerus: The American Society For Surgery of The Hand.)Документ15 страницElbow Fractures: Distal Humerus: The American Society For Surgery of The Hand.)Radu UrcanОценок пока нет
- Common Pediatric Elbow Fractures: Erin S. Hart Allison Turner Maurice Albright Brian E. GrottkauДокумент7 страницCommon Pediatric Elbow Fractures: Erin S. Hart Allison Turner Maurice Albright Brian E. GrottkauFino SopianОценок пока нет
- Managementofdistal Femurfracturesinadults: An Overview of OptionsДокумент12 страницManagementofdistal Femurfracturesinadults: An Overview of OptionsDoctor's BettaОценок пока нет
- 2001 - Cartilage Substitutes - Overview of Basic Science and Treatment OptionsДокумент16 страниц2001 - Cartilage Substitutes - Overview of Basic Science and Treatment Optionsgrofecbio1Оценок пока нет
- Fractures of The Radial Head (2013)Документ9 страницFractures of The Radial Head (2013)Say MamenОценок пока нет
- Calcaneal Fractures Where Are We NowДокумент11 страницCalcaneal Fractures Where Are We NowfunmugОценок пока нет
- Hombro Inlges PDFДокумент6 страницHombro Inlges PDFOscar Segun DoОценок пока нет
- Hand Clin 2007 23 (2) 165Документ13 страницHand Clin 2007 23 (2) 165Juan Del rosalОценок пока нет
- Clavicula FractureДокумент6 страницClavicula Fracturedrian pamungkasОценок пока нет
- Fractures of The Cervical Spine: ReviewДокумент7 страницFractures of The Cervical Spine: ReviewMeri Fitria HandayaniОценок пока нет
- Fraser MoodieДокумент11 страницFraser MoodieWiindaОценок пока нет
- Tompkins, JPOSNA ARTICLE 172 - FINAL UPDATEDДокумент13 страницTompkins, JPOSNA ARTICLE 172 - FINAL UPDATEDTania RahamanОценок пока нет
- Toorthj 7 329 PDFДокумент5 страницToorthj 7 329 PDFmuhammad robyОценок пока нет
- Femoral Neck Fractures in Young Patients State Of.3Документ5 страницFemoral Neck Fractures in Young Patients State Of.3Rizwan Ahamed T AОценок пока нет
- Complex Elbow Instability: Matthew Dipaola, MD, William B. Geissler, MD, A. Lee Osterman, MDДокумент14 страницComplex Elbow Instability: Matthew Dipaola, MD, William B. Geissler, MD, A. Lee Osterman, MDAndrea Z MilanoОценок пока нет
- Fractures of The Condylar ProcessДокумент15 страницFractures of The Condylar Processmargarita mogollonОценок пока нет
- Distal Radius FractureДокумент16 страницDistal Radius FractureDeneishMuruОценок пока нет
- Anexo 01 Clase 04 Unidad IiДокумент9 страницAnexo 01 Clase 04 Unidad IiSebastiánCandiaОценок пока нет
- Perioperative Management of Distal Radius Fractures: Jiang An Lim, Bryan LC Loh, George Sylvestor and Wasim KhanДокумент5 страницPerioperative Management of Distal Radius Fractures: Jiang An Lim, Bryan LC Loh, George Sylvestor and Wasim Khansuci triana putriОценок пока нет
- Pediatric Supracondylar Fractures of The Distal Humerus: Provided by Springer - Publisher ConnectorДокумент7 страницPediatric Supracondylar Fractures of The Distal Humerus: Provided by Springer - Publisher ConnectorBison_sonОценок пока нет
- Humeral Non UnionДокумент12 страницHumeral Non Unionmmqk122Оценок пока нет
- Art 1Документ10 страницArt 1Danilo LlumitasigОценок пока нет
- Fractura Cadera 1Документ22 страницыFractura Cadera 1Júlia LedesmaОценок пока нет
- Sacral Alae S1 and S2Документ11 страницSacral Alae S1 and S2Aysiah AzhariОценок пока нет
- Monteggia Fractures - Pearls and PitfallsДокумент9 страницMonteggia Fractures - Pearls and PitfallsdrdabielmaderacОценок пока нет
- 17 - Distal Radius FracturesДокумент78 страниц17 - Distal Radius FracturesFlorin PanduruОценок пока нет
- Occlusal Schemes in FPDДокумент6 страницOcclusal Schemes in FPDPadmini ReddyОценок пока нет
- Humerus FractureДокумент5 страницHumerus FracturecyahiminОценок пока нет
- Sarver PDFДокумент8 страницSarver PDFanon_768201406Оценок пока нет
- GaleazziДокумент11 страницGaleazzijuanitiusОценок пока нет
- 11.clavicle Fractures REVДокумент11 страниц11.clavicle Fractures REVRika Yulizah GobelОценок пока нет
- Currentmanagementof Metacarpalfractures: Rafael Diaz-Garcia,, Jennifer F. WaljeeДокумент12 страницCurrentmanagementof Metacarpalfractures: Rafael Diaz-Garcia,, Jennifer F. WaljeeHarry CenОценок пока нет
- Reconstruction of Posttraumatic Disorders of The ForearmДокумент12 страницReconstruction of Posttraumatic Disorders of The Forearmsinung bawonoОценок пока нет
- Manejo de Fracturas Mediales de Cadera 2015 Femoral Neck Fractures - Current ManagementДокумент9 страницManejo de Fracturas Mediales de Cadera 2015 Femoral Neck Fractures - Current ManagementSergio Tomas Cortés MoralesОценок пока нет
- 2022 Fracturas Mandibulares de CondiloДокумент14 страниц2022 Fracturas Mandibulares de CondiloPaola AlcocerОценок пока нет
- Distal Clavicle Fracture Radiography and Treatment: A Pictorial EssayДокумент9 страницDistal Clavicle Fracture Radiography and Treatment: A Pictorial EssayAdella Maharani SОценок пока нет
- Stav SoucasnyДокумент14 страницStav SoucasnyTommysОценок пока нет
- Subtrochanteric Femur Fractures: Asheesh Bedi, MD, T. Toan Le, MDДокумент11 страницSubtrochanteric Femur Fractures: Asheesh Bedi, MD, T. Toan Le, MDMd.Shafiul EzazОценок пока нет
- Cia 5 337Документ9 страницCia 5 337Shahid HussainОценок пока нет
- Classification of Pelvic Fractures and Its Clinical RelevanceДокумент6 страницClassification of Pelvic Fractures and Its Clinical RelevanceMohamed AzeemОценок пока нет
- Fractures of Clavicle AserДокумент44 страницыFractures of Clavicle AserHeba ElgoharyОценок пока нет
- Spinal Cord Injury: Causation & PathophysiologyДокумент10 страницSpinal Cord Injury: Causation & Pathophysiologycpradheep100% (3)
- Ac Joint Seperation Clavicle FractureДокумент5 страницAc Joint Seperation Clavicle Fractureapi-356829966Оценок пока нет
- Evidence-Based Review of Distal Radius Fractures: Benjamin M. Mauck,, Colin W. SwiglerДокумент12 страницEvidence-Based Review of Distal Radius Fractures: Benjamin M. Mauck,, Colin W. SwiglerOrtopedia HGMОценок пока нет
- Fractures Radial Head & Neck. JBJS. 2013Документ10 страницFractures Radial Head & Neck. JBJS. 2013C Martin TraumatoОценок пока нет
- Acute Distal Radioulnar Joint InstabilityДокумент13 страницAcute Distal Radioulnar Joint Instabilityyerson fernando tarazona tolozaОценок пока нет
- Misra 2019Документ3 страницыMisra 2019Jawhar DhiafОценок пока нет
- Mandibulasr Truma ManagementДокумент18 страницMandibulasr Truma Managementjoal510Оценок пока нет
- Surgery Management of Fractures, Dislocations, and Traumatic Instability of The ElbowДокумент17 страницSurgery Management of Fractures, Dislocations, and Traumatic Instability of The ElbowErvaldi IlhamОценок пока нет
- Galeazzi-Fracture 6Документ14 страницGaleazzi-Fracture 6MIGUEL ANGEL MEJIA FERNANDEZОценок пока нет
- Fractures Pathophysiology Treatment and Nursing CareДокумент9 страницFractures Pathophysiology Treatment and Nursing Careaddica0% (1)
- Acromioclavicular Joint Injury, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsОт EverandAcromioclavicular Joint Injury, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsОценок пока нет
- Acetabular Fractures in Older Patients: Assessment and ManagementОт EverandAcetabular Fractures in Older Patients: Assessment and ManagementTheodore T. MansonОценок пока нет
- Pain Therapy in Children and Adolescents: Boris Zernikow, Tanja HechlerДокумент17 страницPain Therapy in Children and Adolescents: Boris Zernikow, Tanja HechlerNUR AIDAОценок пока нет
- The Use of MRI in Evaluating Knee Pain in Patients Aged 40 Years and OlderДокумент7 страницThe Use of MRI in Evaluating Knee Pain in Patients Aged 40 Years and OlderDiana Marcela Benítez HernándezОценок пока нет
- Management of Fractures of The Proximal UlnaДокумент12 страницManagement of Fractures of The Proximal UlnaDiana Marcela Benítez HernándezОценок пока нет
- Terrible Triad Injury of He ElbowДокумент15 страницTerrible Triad Injury of He Elbowbarbara liuva chia policarpoОценок пока нет
- Trauma en Pediatria. Evaluacion. J Emerg Crit Care Med 2018 2:3Документ8 страницTrauma en Pediatria. Evaluacion. J Emerg Crit Care Med 2018 2:3Diana Marcela Benítez HernándezОценок пока нет
- Management of The Floating Knee.Документ8 страницManagement of The Floating Knee.barbara liuva chia policarpoОценок пока нет
- Treatment of Distal Radius Fractures.7 PDFДокумент10 страницTreatment of Distal Radius Fractures.7 PDFHayudhiaОценок пока нет
- Journal Orthopedi 3Документ5 страницJournal Orthopedi 3Nur SulistiyaningsihОценок пока нет
- Fractura Tercio Medio ClavíДокумент5 страницFractura Tercio Medio ClavíDiana Marcela Benítez HernándezОценок пока нет
- Metabolic Syndrome and Sistemic Inflammation in Patients With COPDДокумент5 страницMetabolic Syndrome and Sistemic Inflammation in Patients With COPDDiana Marcela Benítez HernándezОценок пока нет
- B Blockers and Their Mortality Benefits Underprescribed in Heart Failure and Chronic Obstructive Pulmonary DiseaseДокумент12 страницB Blockers and Their Mortality Benefits Underprescribed in Heart Failure and Chronic Obstructive Pulmonary DiseaseDiana Marcela Benítez HernándezОценок пока нет
- Immunologic Correlates of The AbscopalДокумент7 страницImmunologic Correlates of The AbscopalDiana Marcela Benítez HernándezОценок пока нет
- Catalogue of Unlocking Plates Suzhou Youbetter Medical Apparatus Co., LTDДокумент9 страницCatalogue of Unlocking Plates Suzhou Youbetter Medical Apparatus Co., LTDazisaaiОценок пока нет
- How To Take and Read Hip Joint Radiographs in A Structured WayДокумент2 страницыHow To Take and Read Hip Joint Radiographs in A Structured WaySamantha Orozco PinedaОценок пока нет
- Bone TumorsДокумент15 страницBone Tumorssarguss1450% (2)
- IARC Technical Report No10-9 PDFДокумент89 страницIARC Technical Report No10-9 PDFTanОценок пока нет
- Gr6 Revision - PPT Ete 1Документ30 страницGr6 Revision - PPT Ete 1Doaa AlhussienyОценок пока нет
- II - 4.anterior Cranial FossaДокумент2 страницыII - 4.anterior Cranial FossaalllexissssОценок пока нет
- Anaphy GRAPHIC - ORGANIZERДокумент6 страницAnaphy GRAPHIC - ORGANIZERLuna ScorpiusОценок пока нет
- Muscles That Move The Pectoral GirdleДокумент65 страницMuscles That Move The Pectoral GirdleJennifer FirestoneОценок пока нет
- Lower Extremity Anatomy: Sari Tri Yulianti, S.FT., M.BiomedДокумент73 страницыLower Extremity Anatomy: Sari Tri Yulianti, S.FT., M.BiomedDindaОценок пока нет
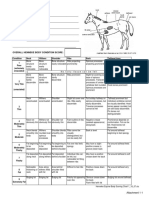
- Henneke BCS ChartДокумент1 страницаHenneke BCS ChartLaviniaMenicucciОценок пока нет
- EMG Analysis of Latissimus Dorsi Erector Spinae and Middle TrapДокумент68 страницEMG Analysis of Latissimus Dorsi Erector Spinae and Middle TrapYuОценок пока нет
- Veterinary AcupunctureДокумент19 страницVeterinary AcupuncturekinezildiОценок пока нет
- Lumbarization of First Sacral VertebraДокумент4 страницыLumbarization of First Sacral VertebraangellisimalОценок пока нет
- 2009.10.09 Legg Calve Perthes Disease 2Документ43 страницы2009.10.09 Legg Calve Perthes Disease 2AnItaОценок пока нет
- TMJ Anatomy and Biomechanics-14Документ67 страницTMJ Anatomy and Biomechanics-14erfan mohammadiОценок пока нет
- Kütük Cubuk Uyum StandartlariДокумент2 страницыKütük Cubuk Uyum StandartlariÖZGÜRОценок пока нет
- Can Trendelenburg'S Sign Be Positive If The Hip Is Normal?Документ5 страницCan Trendelenburg'S Sign Be Positive If The Hip Is Normal?Juniarto PangestuОценок пока нет
- The Use of Locking Plates in Complex Midfoot Fractures: Orthopaedic SurgeryДокумент4 страницыThe Use of Locking Plates in Complex Midfoot Fractures: Orthopaedic Surgeryfebyan yohanesОценок пока нет
- Rachel Scott - Anatomy of Bone Joints Jan 2019Документ7 страницRachel Scott - Anatomy of Bone Joints Jan 2019idyogaОценок пока нет
- ANTRIAN OPERASI SPINE Update 29 MeiДокумент21 страницаANTRIAN OPERASI SPINE Update 29 MeiIbnu ImadudinОценок пока нет
- Jurnal Oa Pak Harto Dan Bu Suriani MWD & Rhytmical StabilisasiДокумент6 страницJurnal Oa Pak Harto Dan Bu Suriani MWD & Rhytmical StabilisasiErwynk EriantoОценок пока нет
- CSEC - Form 4 Human and Social Biology NotesДокумент4 страницыCSEC - Form 4 Human and Social Biology NotesLeon Abel80% (5)
- Back and Spine AnatomyДокумент7 страницBack and Spine AnatomyCarmela Beatriz Suelan100% (1)
- MCQ Ortho 1Документ18 страницMCQ Ortho 1Pradeep Kumar100% (3)
- Frog SkeletonДокумент2 страницыFrog SkeletonJermaine Joyce Arvesu-Lugada0% (2)
- 1.2.2.A SkeletonHuntДокумент3 страницы1.2.2.A SkeletonHuntHBSrocksОценок пока нет
- Extraoral RadiograhyДокумент7 страницExtraoral RadiograhyKanish AggarwalОценок пока нет
- 2.bones of Trunk & LimbsДокумент19 страниц2.bones of Trunk & LimbsRioОценок пока нет
- C 06 Bradford II Faunal AnalysisДокумент14 страницC 06 Bradford II Faunal AnalysisCraig ChartierОценок пока нет
- Upper Extremities Rad PosiДокумент12 страницUpper Extremities Rad PosiJoan GemotoОценок пока нет