Вам также может понравиться
- Cardiac Dysrhythmia Chart Med-Surg NUR4Документ3 страницыCardiac Dysrhythmia Chart Med-Surg NUR4ktfosterfd2096% (97)
- Advanced Cardiac Life Support Quick Study Guide 2015 Updated GuidelinesОт EverandAdvanced Cardiac Life Support Quick Study Guide 2015 Updated GuidelinesРейтинг: 4 из 5 звезд4/5 (6)
- Advance Cardiac Life Support: Short, Sweet and to the PointОт EverandAdvance Cardiac Life Support: Short, Sweet and to the PointРейтинг: 3 из 5 звезд3/5 (2)
- EKG and ECG Interpretation: Learn EKG Interpretation, Rhythms, and Arrhythmia Fast!От EverandEKG and ECG Interpretation: Learn EKG Interpretation, Rhythms, and Arrhythmia Fast!Оценок пока нет
- ECG & EKG Interpretation: How to interpret ECG & EKG, including rhythms, arrhythmias, and more!От EverandECG & EKG Interpretation: How to interpret ECG & EKG, including rhythms, arrhythmias, and more!Оценок пока нет
- Acls DrugsДокумент10 страницAcls DrugsChintami Octavia100% (1)
- ECG in Emergency MedicineДокумент228 страницECG in Emergency MedicineBobbyGustafsonОценок пока нет
- ACLS Full Lesson Plans PDFДокумент60 страницACLS Full Lesson Plans PDFVictoriano Mendez100% (1)
- Chest Tube Explanation by AllnursesДокумент3 страницыChest Tube Explanation by AllnursesYemaya84Оценок пока нет
- ACLS Advanced Cardiovascular Life Support Provider Manual 2023От EverandACLS Advanced Cardiovascular Life Support Provider Manual 2023Оценок пока нет
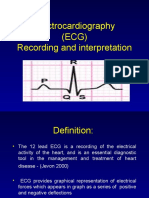
- Electrocardiography (ECG) Recording and InterpretationДокумент59 страницElectrocardiography (ECG) Recording and Interpretationkhushsandhu0% (1)
- ICU Drips: Stephanie Sanderson, RN, MSN, CNS, CCNS, CCRN Medical Cardiac ICU-UNMHДокумент32 страницыICU Drips: Stephanie Sanderson, RN, MSN, CNS, CCNS, CCRN Medical Cardiac ICU-UNMHNicole Adkins100% (1)
- Introd To ECG Code Blue Champs March 2019Документ52 страницыIntrod To ECG Code Blue Champs March 2019james rukenya100% (1)
- ACLS Provider Manual Supplementary Material: © 2020 American Heart AssociationДокумент75 страницACLS Provider Manual Supplementary Material: © 2020 American Heart AssociationpolelОценок пока нет
- ACLS CE-Part I of III - ECG Strip Interpretation W Case Scenarios SupplementalДокумент80 страницACLS CE-Part I of III - ECG Strip Interpretation W Case Scenarios SupplementalMarc Imhotep Cray, M.D.100% (2)
- The 12-Lead Electrocardiogram for Nurses and Allied ProfessionalsОт EverandThe 12-Lead Electrocardiogram for Nurses and Allied ProfessionalsОценок пока нет
- Shock: Shout For Help/Activate Emergency ResponseДокумент6 страницShock: Shout For Help/Activate Emergency ResponseandiyanimalikОценок пока нет
- DIT High Yield Questions PDFДокумент13 страницDIT High Yield Questions PDFjoshОценок пока нет
- American Heart Association Guidelines For CPR 2015: Christopher RyalinoДокумент50 страницAmerican Heart Association Guidelines For CPR 2015: Christopher RyalinoLightОценок пока нет
- PALS Study GuideДокумент12 страницPALS Study GuidePrerna SehgalОценок пока нет
- The Little Black Book of Ecg Secrets PDFДокумент12 страницThe Little Black Book of Ecg Secrets PDFamaandreiОценок пока нет
- Step2Ck Nbme 8 QuestionsДокумент166 страницStep2Ck Nbme 8 Questionstaha albarghathyОценок пока нет
- Ecgs Made Easy 5th Edition Aehlert Test BankДокумент14 страницEcgs Made Easy 5th Edition Aehlert Test BankQuinn50% (2)
- Pediatric Advanced Life Support: I. PALS System Approach AlgorithmДокумент19 страницPediatric Advanced Life Support: I. PALS System Approach AlgorithmIsabel Castillo100% (1)
- 3 Combined AHA BLS ACLS Updates CombinedДокумент5 страниц3 Combined AHA BLS ACLS Updates Combinedamanrup randhawa100% (1)
- 15 Item ACLS Drill With RationaleДокумент12 страниц15 Item ACLS Drill With RationaleLj Ferolino100% (1)
- Emergency Lecture PDFДокумент57 страницEmergency Lecture PDFDuane Liloc100% (1)
- American Heart Association Guidelines For CPR 2015: Wanida Chongarunngamsang, MD. Faculty of Srinakarinwirot UniversityДокумент49 страницAmerican Heart Association Guidelines For CPR 2015: Wanida Chongarunngamsang, MD. Faculty of Srinakarinwirot UniversityZulkarnainBustamamОценок пока нет
- AHA ELearning ACLS Precourse Self-Assessment and Precourse WorkДокумент1 страницаAHA ELearning ACLS Precourse Self-Assessment and Precourse Work9kjsntkrzcОценок пока нет
- 15 Item Acls DrillДокумент4 страницы15 Item Acls DrillVal SolidumОценок пока нет
- Echocardiographic Atlas of Adult Congenital Heart Disease: Hakimeh Sadeghian Zahra Savand-RoomiДокумент486 страницEchocardiographic Atlas of Adult Congenital Heart Disease: Hakimeh Sadeghian Zahra Savand-RoomiGeorgiana-Gratiela MalaescuОценок пока нет
- Acls ExamДокумент42 страницыAcls ExamScribdTranslationsОценок пока нет
- ToxidromesДокумент1 страницаToxidromesMayer Rosenberg100% (7)
- ACLS Class Packet 2015Документ9 страницACLS Class Packet 2015Chi Wiin100% (3)
- ACLS Training - Most Important Points To RememberДокумент5 страницACLS Training - Most Important Points To RememberEman ElzeftawyОценок пока нет
- TestДокумент11 страницTestzenagit123456100% (1)
- 2020 Acls Megacode Testing Scenarios - 2Документ13 страниц2020 Acls Megacode Testing Scenarios - 2Dr. Saqib RazaОценок пока нет
- ACLS DrugsДокумент16 страницACLS Drugstostc100% (2)
- AHA ACLS Written Test: Ready To Study? Start With FlashcardsДокумент8 страницAHA ACLS Written Test: Ready To Study? Start With FlashcardssallyОценок пока нет
- NCP For Acute Coronary SyndromeДокумент3 страницыNCP For Acute Coronary Syndromesarahtot75% (4)
- CPR ACLS Study GuideДокумент18 страницCPR ACLS Study GuideJohn Phamacy100% (1)
- Sample Acls For DummiesДокумент3 страницыSample Acls For DummiesTodd Cole100% (1)
- AclsДокумент85 страницAclsJulia CostaОценок пока нет
- ACLS Study Guide: Ecg Strip InterpretationДокумент12 страницACLS Study Guide: Ecg Strip InterpretationMariana Berger100% (1)
- Torsade De Pointes, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsОт EverandTorsade De Pointes, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsОценок пока нет
- Cerebrovascular AccidentДокумент15 страницCerebrovascular AccidentBeeshma BirjasinghОценок пока нет
- AHA Examination Auscultation Part IVДокумент42 страницыAHA Examination Auscultation Part IVHananya ManroeОценок пока нет
- Chapter 20 - Cardiac EmergenciesДокумент96 страницChapter 20 - Cardiac EmergenciesAmit KlОценок пока нет
- PALS Precourse Self 2023Документ9 страницPALS Precourse Self 2023Airene SibleОценок пока нет
- 2010 Integrated Updated Circulation ACLS Acute Coronary Syndromes AlgorithmДокумент1 страница2010 Integrated Updated Circulation ACLS Acute Coronary Syndromes Algorithmms_lezahОценок пока нет
- CardiomyopathiesДокумент48 страницCardiomyopathiesTanvir AhmedОценок пока нет
- Pepp Als PretestДокумент4 страницыPepp Als PretestDave BoppОценок пока нет
- AclsДокумент11 страницAclsdyah rahayu hutamiОценок пока нет
- Rhythm Recognition - ACLS Medical Training 1Документ9 страницRhythm Recognition - ACLS Medical Training 1Catalina BorquezОценок пока нет
- BLS SummaryДокумент2 страницыBLS Summaryreyes markОценок пока нет
- ACLS and MegacodeДокумент33 страницыACLS and MegacodeMark Joseph100% (1)
- Cardiac Dysrhythmia Final Study GuideДокумент14 страницCardiac Dysrhythmia Final Study GuideBSNNursing101100% (2)
- Acls MegacodeДокумент8 страницAcls Megacodes33d_destinyОценок пока нет
- PALS Precourse Self-AssessmentДокумент2 страницыPALS Precourse Self-AssessmentGabriel Del RosarioОценок пока нет
- ACLS QuizletДокумент7 страницACLS Quizletek.9006001Оценок пока нет
- Acls LectureДокумент15 страницAcls LectureVincent BautistaОценок пока нет
- Basic Life Support (BLS) Training Course: FeaturesДокумент1 страницаBasic Life Support (BLS) Training Course: FeaturesSheryl Fuentes De GuzmanОценок пока нет
- ITLS Answer Sheet 8th EditionДокумент1 страницаITLS Answer Sheet 8th EditionStan Anis100% (1)
- Arterial Lines in PACU: Presented by Autum Jacobs RN, BSNДокумент34 страницыArterial Lines in PACU: Presented by Autum Jacobs RN, BSNinuko1212Оценок пока нет
- Quick Guide To Identify Various Ecg RhythmsДокумент8 страницQuick Guide To Identify Various Ecg RhythmsVergiling SheebaОценок пока нет
- Mastering Electocardiograms - Honda-2Документ3 страницыMastering Electocardiograms - Honda-2Christian MacielОценок пока нет
- Grady EMS Drug List 2017 FINALДокумент20 страницGrady EMS Drug List 2017 FINALThomas LeachОценок пока нет
- Heart Failure: Diagnosis and EvaluationДокумент29 страницHeart Failure: Diagnosis and Evaluation黃昱睿Оценок пока нет
- Tof Case ReportДокумент11 страницTof Case ReportPatrick DycocoОценок пока нет
- Ebook Cardiology Board Review and Self Assessment A Companion Guide To Hursts The Heart PDF Full Chapter PDFДокумент67 страницEbook Cardiology Board Review and Self Assessment A Companion Guide To Hursts The Heart PDF Full Chapter PDFjohn.eastman290100% (26)
- Diagnosis and Management of AFДокумент135 страницDiagnosis and Management of AFMatthew ChristopherОценок пока нет
- Diamondback 360 Coronary Orbital Atherectomy SystemДокумент51 страницаDiamondback 360 Coronary Orbital Atherectomy SystemManigandan DhamodhiranОценок пока нет
- 1 8 KardiologiaДокумент78 страниц1 8 KardiologiaRati ZivzivadzeОценок пока нет
- Heart Sounds: Presented by Group 2A & 3AДокумент13 страницHeart Sounds: Presented by Group 2A & 3AMeow Catto100% (1)
- Cardiovascular DisordersДокумент20 страницCardiovascular DisordersHampson MalekanoОценок пока нет
- Algoritma CHFДокумент1 страницаAlgoritma CHFdiany astutiОценок пока нет
- Sport - Cardiology Course - Program PDFДокумент4 страницыSport - Cardiology Course - Program PDFNico IonaşcuОценок пока нет
- Congenital-Heart-Disease MidwiferyДокумент16 страницCongenital-Heart-Disease MidwiferyDrMaxamuud Caqli NuurОценок пока нет
- Infectious Disease of The HeartДокумент3 страницыInfectious Disease of The HeartClaire GidoОценок пока нет
- Effect of Progressive Muscle Relaxation Combined With Deep Breathing Technique Immediately After Aerobic Exercises On Essential HypertensionДокумент2 страницыEffect of Progressive Muscle Relaxation Combined With Deep Breathing Technique Immediately After Aerobic Exercises On Essential HypertensionNetraОценок пока нет
- Heart Valve DiseaseДокумент12 страницHeart Valve DiseaseLucero Larios GarcíaОценок пока нет
- Preview ACLS Algorithm PDFДокумент29 страницPreview ACLS Algorithm PDFsiti marwiyahОценок пока нет
- Cardiology Basic QuestionsДокумент9 страницCardiology Basic QuestionsSunita PooniaОценок пока нет
- Zuñega - Congenital Heart Disease Educational MaterialsДокумент13 страницZuñega - Congenital Heart Disease Educational MaterialsAprilene Angel Balaque ZunegaОценок пока нет
- Ischemic Heart DiseaseДокумент4 страницыIschemic Heart DiseaseBanana CakeОценок пока нет
- Lesson Plan MyocardialДокумент4 страницыLesson Plan MyocardialV MОценок пока нет