Вам также может понравиться
- Indirect Inguinal HerniaДокумент53 страницыIndirect Inguinal HerniaYlamher Bufi ImperialОценок пока нет
- Circumcision in Baby BoysДокумент6 страницCircumcision in Baby BoysJbl2328Оценок пока нет
- Tamang GrammarДокумент12 страницTamang Grammarsoftdina100% (1)
- Uterine MyomaДокумент38 страницUterine MyomaErika Capitly100% (1)
- Indirect Inguinal HerniaДокумент54 страницыIndirect Inguinal HerniaYlamher Bufi Imperial100% (1)
- Distortion of The Ecclesiological Views of Metropolitan Chrysostomos of PhlorinaДокумент11 страницDistortion of The Ecclesiological Views of Metropolitan Chrysostomos of PhlorinaHibernoSlavОценок пока нет
- Interview With Hohepa Mapiria Joseph - Joe - Murphy Royal Regent 7 July 2003Документ61 страницаInterview With Hohepa Mapiria Joseph - Joe - Murphy Royal Regent 7 July 2003kiwiit100% (8)
- Chapter 1Документ38 страницChapter 1Kurt dela Torre100% (1)
- Abruptio Placenta FullДокумент10 страницAbruptio Placenta FullChester ManaloОценок пока нет
- Inguinal Hernia by Dr. TalabiДокумент16 страницInguinal Hernia by Dr. TalabidayomanОценок пока нет
- GFP EnauДокумент2 страницыGFP EnauDomenico BevilacquaОценок пока нет
- Melo V PeopleДокумент1 страницаMelo V PeoplejjangОценок пока нет
- Libi Vs IACДокумент1 страницаLibi Vs IACBingoheartОценок пока нет
- AutoPIPE Tutorial PDFДокумент156 страницAutoPIPE Tutorial PDFdhaktodesatyajitОценок пока нет
- Ectopic PregnancyДокумент9 страницEctopic PregnancyCatherine ZamoraОценок пока нет
- Inguinal Hernia: Shohreh Toutounchi Reference: Schwartz Principles of Surgery 2010 Internship: 1391Документ29 страницInguinal Hernia: Shohreh Toutounchi Reference: Schwartz Principles of Surgery 2010 Internship: 1391Ritz CelsoОценок пока нет
- Case Study of Abruptio PlacentaДокумент14 страницCase Study of Abruptio PlacentaLexy Milante80% (10)
- Uterine Fibroids: Q: What Are Fibroids? AДокумент8 страницUterine Fibroids: Q: What Are Fibroids? Abasantjain12345Оценок пока нет
- UTERINE ATONY - CASE STUDY - EditedДокумент50 страницUTERINE ATONY - CASE STUDY - EditedMonica BorjaОценок пока нет
- Epispadias and Exstrophy 1 PDFДокумент4 страницыEpispadias and Exstrophy 1 PDFSabria Chairunnisa RosadiОценок пока нет
- N 290-Chapter 46 ReviewДокумент4 страницыN 290-Chapter 46 ReviewArmelle DelvaОценок пока нет
- NpfuДокумент10 страницNpfunagarathnanmОценок пока нет
- Epispadias and Exstrophy 1Документ4 страницыEpispadias and Exstrophy 1Alip WildanОценок пока нет
- Ilovepdf MergedДокумент53 страницыIlovepdf MergedHardikОценок пока нет
- What Is TAHДокумент9 страницWhat Is TAHBanaag JayОценок пока нет
- TAHBSO-convertedДокумент5 страницTAHBSO-convertedShean Y. LamosaoОценок пока нет
- Bioethics-Abortion-And-Euthanasia 2Документ3 страницыBioethics-Abortion-And-Euthanasia 2Alvin Josh CalingayanОценок пока нет
- CASE ANALYSIS Ectopic Pregnancy Part 1Документ10 страницCASE ANALYSIS Ectopic Pregnancy Part 1Diane Celine SantianoОценок пока нет
- C. Hematuria - Jurnal Uro 1Документ4 страницыC. Hematuria - Jurnal Uro 1kikiaprilianiОценок пока нет
- Hypospadias 1Документ4 страницыHypospadias 1ufrieОценок пока нет
- Vaginal Agenesis PDFДокумент4 страницыVaginal Agenesis PDFBill HarmanОценок пока нет
- AbortionДокумент4 страницыAbortionDr. Muha. Hasan Mahbub-Ur-RahmanОценок пока нет
- Hypospadiasis and EpispadiasisДокумент9 страницHypospadiasis and EpispadiasisThilaga RamОценок пока нет
- MRKH DissertationДокумент4 страницыMRKH DissertationWriteMyPaperForCheapUK100% (1)
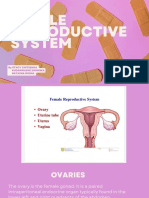
- Female Reproductive SystemДокумент48 страницFemale Reproductive SystemLarry MagwegweОценок пока нет
- Hypospadias in BriefДокумент3 страницыHypospadias in BriefbebibebihoОценок пока нет
- AMODIAДокумент3 страницыAMODIAMarriel AmodiaОценок пока нет
- Endometriosis: by Jane LyttletonДокумент8 страницEndometriosis: by Jane Lyttletonitsik12886Оценок пока нет
- Male Reproductive System 1mittalДокумент23 страницыMale Reproductive System 1mittalSAYMABANUОценок пока нет
- Inguinal Hernia in Pediatric PatientsДокумент17 страницInguinal Hernia in Pediatric PatientsPatrycjaSkierkaОценок пока нет
- ColporrhaphyДокумент28 страницColporrhaphyDobre DenisaОценок пока нет
- Pelvic Floor Dialogues Issue 6Документ4 страницыPelvic Floor Dialogues Issue 6Urología GinecológicaОценок пока нет
- How Reproductive Systems Work: Merck ManualsДокумент3 страницыHow Reproductive Systems Work: Merck ManualsAlexs VillafloresОценок пока нет
- Osun State University, Osogbo: Department of Nursing SciencesДокумент6 страницOsun State University, Osogbo: Department of Nursing SciencesGreg Carmela annОценок пока нет
- A Laparotomy Is A Large Incision MadeДокумент4 страницыA Laparotomy Is A Large Incision Mademnemonics101Оценок пока нет
- Agenesis VaginaДокумент6 страницAgenesis Vaginai305Оценок пока нет
- Obstetric Fistula An Overview: Brad R. Mackinnon University of VermontДокумент32 страницыObstetric Fistula An Overview: Brad R. Mackinnon University of VermontJhansi PeddiОценок пока нет
- HYPOSPADIUSДокумент21 страницаHYPOSPADIUSLady350zОценок пока нет
- What Is InfertilityДокумент11 страницWhat Is InfertilityReyansh gargОценок пока нет
- Case Presentation Second Year 2nd SemesterДокумент36 страницCase Presentation Second Year 2nd SemesterJohn Robert PescadorОценок пока нет
- Diagnóstico Tardio de MARДокумент8 страницDiagnóstico Tardio de MARthedoctor1986Оценок пока нет
- What Is Hypospadias?Документ5 страницWhat Is Hypospadias?Anonymous MWd5UOUuiyОценок пока нет
- Medical Transcription Sample OBДокумент8 страницMedical Transcription Sample OBAngelo AlbaОценок пока нет
- What Is An Imperforated Anus?: Cincinnati Children's HospitalДокумент5 страницWhat Is An Imperforated Anus?: Cincinnati Children's HospitalRej PanganibanОценок пока нет
- Sexual Reproduction in Humans CLASS 10Документ5 страницSexual Reproduction in Humans CLASS 10shallowОценок пока нет
- Hys Tero Salpingo GramДокумент5 страницHys Tero Salpingo GramShreMulyanaRahimОценок пока нет
- Laparoscopic Ectopic Pregnancy India: Tubal Ligation Surgery With Medical TourismДокумент4 страницыLaparoscopic Ectopic Pregnancy India: Tubal Ligation Surgery With Medical TourismJen Elcano MejiaОценок пока нет
- Infertility EssayДокумент5 страницInfertility EssayaryroxОценок пока нет
- Presentation and Discussion ReportДокумент8 страницPresentation and Discussion ReportGresia FalentinaОценок пока нет
- HypospadiasДокумент12 страницHypospadiasMohamed Na3eemОценок пока нет
- Anorectal Malformations (ARM) in Girls: The Children's HospitalДокумент12 страницAnorectal Malformations (ARM) in Girls: The Children's HospitalAnishaОценок пока нет
- Ovarian CancerДокумент4 страницыOvarian CancerJuan Miguel Caspe MangayaОценок пока нет
- Hernias AdultosДокумент8 страницHernias AdultosJuan Jose SantivañezОценок пока нет
- History: Current Symptoms Are Explored Using Open-Ended Questions Followed by Specific QuestionsДокумент9 страницHistory: Current Symptoms Are Explored Using Open-Ended Questions Followed by Specific QuestionsRirin Dwi LestariОценок пока нет
- AbortionДокумент6 страницAbortionChelsie May Mahilum TudioОценок пока нет
- Guide to Pediatric Urology and Surgery in Clinical PracticeОт EverandGuide to Pediatric Urology and Surgery in Clinical PracticeОценок пока нет
- A Simple Guide to Rectal Prolapse, (Updated) diagnosis, Treatment and Related ConditionsОт EverandA Simple Guide to Rectal Prolapse, (Updated) diagnosis, Treatment and Related ConditionsОценок пока нет
- Hazardous Location Division Listed LED Light: Model 191XLДокумент2 страницыHazardous Location Division Listed LED Light: Model 191XLBernardo Damas EspinozaОценок пока нет
- Why Do Climates Change ?: Climate Changes Over The Last MillenniumДокумент44 страницыWhy Do Climates Change ?: Climate Changes Over The Last Millenniumshaira alliah de castroОценок пока нет
- Regional Trial Court National Capital Judicial Region: ComplainantДокумент5 страницRegional Trial Court National Capital Judicial Region: ComplainantNeil Patrick QuiniquiniОценок пока нет
- Jazz Guitar Soloing Etude F Blues 3 To 9 ArpsДокумент1 страницаJazz Guitar Soloing Etude F Blues 3 To 9 ArpsLeonardoPiresОценок пока нет
- Sample Invoice PDFДокумент3 страницыSample Invoice PDFMarcus OlivieraaОценок пока нет
- Assignment Practice ProblemsДокумент5 страницAssignment Practice ProblemsibrahimmoizОценок пока нет
- Enga10 Speaking Test3Документ2 страницыEnga10 Speaking Test3luana serraОценок пока нет
- This Study Resource WasДокумент2 страницыThis Study Resource Waskaye nicolasОценок пока нет
- Uplifting Hauora Maori RealДокумент32 страницыUplifting Hauora Maori RealFano AsiataОценок пока нет
- Soal Materi 1 KLS X IntroductionДокумент2 страницыSoal Materi 1 KLS X IntroductionFira AnandaОценок пока нет
- SPE 166182 Radio Frequency Identification (RFID) Leads The Way in The Quest For Intervention Free Upper Completion InstallationДокумент9 страницSPE 166182 Radio Frequency Identification (RFID) Leads The Way in The Quest For Intervention Free Upper Completion InstallationjangolovaОценок пока нет
- Region XiДокумент2 страницыRegion XiGarcia, Rafael Rico O.Оценок пока нет
- Maulana Azad Library, Aligarh Muslim UniversityДокумент38 страницMaulana Azad Library, Aligarh Muslim Universitybijesh babuОценок пока нет
- The Post OfficeДокумент4 страницыThe Post OfficeKatherine LuisОценок пока нет
- INSTRUCTIONS FOR USOL PRIVATE REAPPEAR DE January 2022Документ4 страницыINSTRUCTIONS FOR USOL PRIVATE REAPPEAR DE January 2022RaghavОценок пока нет
- Statistics and Data CollectionДокумент11 страницStatistics and Data CollectionRichimon LicerioОценок пока нет
- Optical CamouflageДокумент27 страницOptical CamouflageAlliluddin ShaikОценок пока нет
- University of Physician V CIRДокумент24 страницыUniversity of Physician V CIROlivia JaneОценок пока нет
- 5 Manifestos Da ArteДокумент3 страницы5 Manifestos Da ArteCinthia MendonçaОценок пока нет
- Individual Ability in SoftwareДокумент9 страницIndividual Ability in Softwaredhana0809100% (4)
- ABC LTD ProposalДокумент4 страницыABC LTD ProposalAbhishek JurianiОценок пока нет
- Lescture OPACДокумент5 страницLescture OPACAgulto, Ivan R.Оценок пока нет
- Architecture As Interface - Healing Architecture For Epatients. In: Healing Architecture. Hrsg. Nickl-Weller. 2013Документ6 страницArchitecture As Interface - Healing Architecture For Epatients. In: Healing Architecture. Hrsg. Nickl-Weller. 2013Asmaa AyadОценок пока нет