Вам также может понравиться
- Tumors of The NoseДокумент36 страницTumors of The NoseWade JacksonОценок пока нет
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- ShambhaviMahamudraKriya PDFДокумент3 страницыShambhaviMahamudraKriya PDFpvsairam92% (12)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- Effects of Exercise On Laboratory Test ResultsДокумент7 страницEffects of Exercise On Laboratory Test ResultsWade Jackson100% (1)
- Chlamydia Psittaci: Laboratory DiagnosisДокумент12 страницChlamydia Psittaci: Laboratory DiagnosisWade JacksonОценок пока нет
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (400)
- Overview of FistulasДокумент39 страницOverview of FistulasWade JacksonОценок пока нет
- Standards of BehaviorДокумент5 страницStandards of BehaviorWade JacksonОценок пока нет
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- Nervous System PathologyДокумент12 страницNervous System PathologyWade JacksonОценок пока нет
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Cerebral PalsyДокумент2 страницыCerebral PalsyTracy100% (1)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- Immuno 32 2 04Документ52 страницыImmuno 32 2 04mmarquezsaОценок пока нет
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- Procedure For Insertion of Saf T Intima Cannula and Subcutaneous InjectionДокумент16 страницProcedure For Insertion of Saf T Intima Cannula and Subcutaneous Injectionmadimadi11Оценок пока нет
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- Tania Howarth ResumeДокумент3 страницыTania Howarth Resumeapi-362528026Оценок пока нет
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- Clinic Handbook of GastroenterologyДокумент285 страницClinic Handbook of Gastroenterologyansarijaved100% (1)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- Chapter 036Документ9 страницChapter 036Neverends201160% (5)
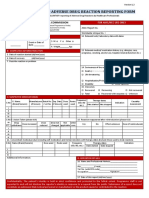
- ADR Reporting FormДокумент2 страницыADR Reporting FormApoorva Tatti100% (1)
- The American College of Radiology BI-RADS Atlas 5 Edition: Frequently Asked QuestionsДокумент18 страницThe American College of Radiology BI-RADS Atlas 5 Edition: Frequently Asked QuestionssatanioОценок пока нет
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- Uti in PregnancyДокумент42 страницыUti in Pregnancydeepak122Оценок пока нет
- 1st Lecture (NCM106 ABC I) Care of Clients in Cellular Aberrations, ABC, Emergency and Disaster NursingДокумент14 страниц1st Lecture (NCM106 ABC I) Care of Clients in Cellular Aberrations, ABC, Emergency and Disaster NursingKamx Mohammed100% (1)
- Endoscopic Skull Base SurgeryДокумент25 страницEndoscopic Skull Base Surgerypramod454992Оценок пока нет
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (345)
- Discharge PlanningДокумент4 страницыDischarge Planningrachel mariam100% (1)
- Appendix 1 Occupational Therapy Bathing-Showering ToolДокумент3 страницыAppendix 1 Occupational Therapy Bathing-Showering ToolNizam lotfiОценок пока нет
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- Vitamin B Deficiency in Children With Infantile Spasms: A Case-Control StudyДокумент5 страницVitamin B Deficiency in Children With Infantile Spasms: A Case-Control StudyireneaureliaОценок пока нет
- Hospital IIIДокумент289 страницHospital IIIAnu GupteОценок пока нет
- Drama Script From Group 3Документ5 страницDrama Script From Group 3Rani NadyaОценок пока нет
- Primary Angle-Closure GlaucomaДокумент10 страницPrimary Angle-Closure Glaucomanisa_kartikaОценок пока нет
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- Euthanasia ThesisДокумент11 страницEuthanasia ThesisAyush MathurОценок пока нет
- Practical Work CA On DX 2012Документ26 страницPractical Work CA On DX 2012Nurul Aulia AbdullahОценок пока нет
- Antihyperglycemic Agents Comparison ChartДокумент9 страницAntihyperglycemic Agents Comparison ChartBonnieОценок пока нет
- 12 Shikha Dorgra DentalДокумент4 страницы12 Shikha Dorgra DentalHarish ChowdaryОценок пока нет
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- Closing Statement PlaintiffДокумент3 страницыClosing Statement PlaintiffJosh HughesОценок пока нет
- Extrapiramidal Symptom Rating Scale PDFДокумент11 страницExtrapiramidal Symptom Rating Scale PDFsisca satyaОценок пока нет
- Hubungan Temuan MRI Dengan Klinis Nyeri Pasien Herniasi Nukleus Pulposus LumbalДокумент13 страницHubungan Temuan MRI Dengan Klinis Nyeri Pasien Herniasi Nukleus Pulposus LumbalHendrawanDianAgungWicaksanaОценок пока нет
- DR Ahmed Abar CVДокумент7 страницDR Ahmed Abar CVAnonymous H1EZvy1yQОценок пока нет
- SchizophreniaДокумент67 страницSchizophreniaHazirah Mokhtar100% (1)
- United General Hospital ICU Expansion Case StudyДокумент7 страницUnited General Hospital ICU Expansion Case StudyTeddy Les Holladayz25% (4)
- Regional Sales Manager Medical Devices in Dallas FT Worth TX Resume James MooreДокумент2 страницыRegional Sales Manager Medical Devices in Dallas FT Worth TX Resume James MooreJamesMoore2Оценок пока нет
- Cruise Ship Safety ConcernsДокумент4 страницыCruise Ship Safety ConcernsAnthony Tunying MantuhacОценок пока нет
- Resume Final 1Документ2 страницыResume Final 1api-308019422Оценок пока нет