Вам также может понравиться
- Adhesive Capsulitis Presentation May 2009Документ29 страницAdhesive Capsulitis Presentation May 2009cm4100% (1)
- ODC Form 2A: Jru@jru - Edu WWW - Jru.edu - PHДокумент5 страницODC Form 2A: Jru@jru - Edu WWW - Jru.edu - PHSharmaine MadlaОценок пока нет
- Calorimetry Problems KeyДокумент2 страницыCalorimetry Problems KeyDon'tAsK TheStupidOnesОценок пока нет
- Family Life Cycle PDFДокумент2 страницыFamily Life Cycle PDFDon'tAsK TheStupidOnes100% (1)
- Case Form Nov 2018Документ4 страницыCase Form Nov 2018Don'tAsK TheStupidOnesОценок пока нет
- Case Form Nov 2018Документ4 страницыCase Form Nov 2018Don'tAsK TheStupidOnesОценок пока нет
- Case Form Nov 2018Документ4 страницыCase Form Nov 2018Don'tAsK TheStupidOnesОценок пока нет
- Case Form Nov 2018Документ4 страницыCase Form Nov 2018Don'tAsK TheStupidOnesОценок пока нет
- Case Form Nov 2018Документ4 страницыCase Form Nov 2018Don'tAsK TheStupidOnesОценок пока нет
- Case Form Nov 2018Документ4 страницыCase Form Nov 2018Don'tAsK TheStupidOnesОценок пока нет
- Case Form Nov 2018Документ4 страницыCase Form Nov 2018Don'tAsK TheStupidOnesОценок пока нет
- Case Form Nov 2018Документ4 страницыCase Form Nov 2018Don'tAsK TheStupidOnesОценок пока нет
- College of Allied HealthДокумент3 страницыCollege of Allied HealthDiana MuañaОценок пока нет
- PRC-BON Memorandum Order No. 1-b Series of 2009Документ2 страницыPRC-BON Memorandum Order No. 1-b Series of 2009PhilippineNursingDirectory.comОценок пока нет
- College of Nursing Cebu City: Surgical Scrub In: Hospital, Municipality/City/ ProvinceДокумент2 страницыCollege of Nursing Cebu City: Surgical Scrub In: Hospital, Municipality/City/ Provincerey.dnggОценок пока нет
- New PRC Form For Batch 2012Документ2 страницыNew PRC Form For Batch 2012Matthew VillonОценок пока нет
- Scrub FormДокумент3 страницыScrub FormJane LaquihonОценок пока нет
- Assisted Delivery In: University of Iloilo Rizal Street, Iloilo City Tel No. (033) 338-1071 Loc. 146Документ3 страницыAssisted Delivery In: University of Iloilo Rizal Street, Iloilo City Tel No. (033) 338-1071 Loc. 146Khyara Marie Estante DemiarОценок пока нет
- Nursing Program PRC FormsДокумент6 страницNursing Program PRC FormsNeil BuquiaОценок пока нет
- PRC-BON Memorandum Order No. 2-b Series of 2009Документ5 страницPRC-BON Memorandum Order No. 2-b Series of 2009PhilippineNursingDirectory.com100% (3)
- QF SON 001 06.20.2023 Rev.05 Case LoadДокумент6 страницQF SON 001 06.20.2023 Rev.05 Case LoadALMIA CAISSA DYОценок пока нет
- PRC CasesДокумент6 страницPRC Casesrie rieОценок пока нет
- Jose Rizal University: ODC Form 1CДокумент3 страницыJose Rizal University: ODC Form 1CJonieP84Оценок пока нет
- School of Health Sciences: O.R. Form 1 AДокумент1 страницаSchool of Health Sciences: O.R. Form 1 AVeigner Whyng CabugayanОценок пока нет
- DR Case Forms Revised March 2022Документ1 страницаDR Case Forms Revised March 2022epepОценок пока нет
- PRC BoN Memorandum No.3-B s.08-O.R.D.R.initial Cord Care FORMДокумент5 страницPRC BoN Memorandum No.3-B s.08-O.R.D.R.initial Cord Care FORMFilipino Nurses CentralОценок пока нет
- Bhci DR Case FormДокумент2 страницыBhci DR Case Formray raisОценок пока нет
- España Boulevard, Sampaloc, Manila, Philippines 1015 Tel. No. 406-1611 Loc.8241 Telefax: 731-5738 WebsiteДокумент1 страницаEspaña Boulevard, Sampaloc, Manila, Philippines 1015 Tel. No. 406-1611 Loc.8241 Telefax: 731-5738 WebsiteNyeam NyeamОценок пока нет
- España Boulevard, Sampaloc, Manila, Philippines 1015 Tel. No. 406-1611 Loc.8241 Telefax: 731-5738 WebsiteДокумент1 страницаEspaña Boulevard, Sampaloc, Manila, Philippines 1015 Tel. No. 406-1611 Loc.8241 Telefax: 731-5738 WebsiteNyeam NyeamОценок пока нет
- Jose Rizal University: ODC Form 1AДокумент2 страницыJose Rizal University: ODC Form 1AJonieP84Оценок пока нет
- Scrub FormsДокумент4 страницыScrub FormsJazel UyОценок пока нет
- Not Applicable For Birthing/Lying-In Clinics/HomesДокумент3 страницыNot Applicable For Birthing/Lying-In Clinics/HomesGayle BautistaОценок пока нет
- 1022 A Cases Form Surgical ScrubДокумент1 страница1022 A Cases Form Surgical ScrubCatherine AteradoОценок пока нет
- Jose Rizal University: ODC Form 1BДокумент3 страницыJose Rizal University: ODC Form 1BJonieP84Оценок пока нет
- PRC FormsДокумент5 страницPRC FormsCelline Isabelle ReyesОценок пока нет
- Actual Delivery FormДокумент1 страницаActual Delivery FormGilyan ZaniahОценок пока нет
- Cases Forms New CurДокумент11 страницCases Forms New CurKiana Agana AsenieroОценок пока нет
- España Boulevard, Sampaloc, Manila, Philippines 1015 Tel. No. 406-1611 Loc.8241 Telefax: 731-5738 WebsiteДокумент1 страницаEspaña Boulevard, Sampaloc, Manila, Philippines 1015 Tel. No. 406-1611 Loc.8241 Telefax: 731-5738 WebsiteNyeam NyeamОценок пока нет
- PRC-Cases Form 02Документ5 страницPRC-Cases Form 02Kceey CruzОценок пока нет
- Or DR Summary CasesДокумент5 страницOr DR Summary CasesAndrian BunaОценок пока нет
- Tarlac State University: Romulo Blvd. San Vicente, Tarlac City (045) 493-1865/ Telefax. (045) 982-0110/ WWW - Tsu.edu - PHДокумент5 страницTarlac State University: Romulo Blvd. San Vicente, Tarlac City (045) 493-1865/ Telefax. (045) 982-0110/ WWW - Tsu.edu - PHXIEROINОценок пока нет
- Assisted Delivery Form 1Документ4 страницыAssisted Delivery Form 1Khyara Marie Estante DemiarОценок пока нет
- Saint Louis University: D.R. FormДокумент6 страницSaint Louis University: D.R. FormTeanu Jose Gabrillo TamayoОценок пока нет
- Scrub Forms NewДокумент6 страницScrub Forms Newbluenurse88Оценок пока нет
- PRC Forms UpdatedДокумент5 страницPRC Forms Updatedehjing100% (3)
- Or Exhibit FormДокумент3 страницыOr Exhibit FormAewooncardivilla21Оценок пока нет
- Manila Tytana CollegesДокумент1 страницаManila Tytana CollegesSkyeОценок пока нет
- Surgical Procedure PerformedДокумент2 страницыSurgical Procedure PerformedDominic BristolОценок пока нет
- Doctor'S Order Sheet: HSP-004-MED-0Документ2 страницыDoctor'S Order Sheet: HSP-004-MED-0Mark Emil BautistaОценок пока нет
- 6 Pre-Operative Information FormДокумент1 страница6 Pre-Operative Information FormAina Haravata50% (2)
- Or PRC Form-CircuДокумент1 страницаOr PRC Form-CircuVinz Alyssa Mae OñoОценок пока нет
- PRC 4m Pakalat Pls MSEUFДокумент2 страницыPRC 4m Pakalat Pls MSEUFjewaОценок пока нет
- Case FormДокумент6 страницCase Formmilkman16Оценок пока нет
- Procedure Performed: Hospital/Home/Lying-in Clinic, Municipality/City/ProvinceДокумент5 страницProcedure Performed: Hospital/Home/Lying-in Clinic, Municipality/City/ProvincejefzisgoodОценок пока нет
- Hospital StandardQC FormsДокумент22 страницыHospital StandardQC FormstotqmОценок пока нет
- PRC DR Inbc LongДокумент3 страницыPRC DR Inbc Longma.jassein.oppus.21Оценок пока нет
- New Forms of Cases PRC 2Документ6 страницNew Forms of Cases PRC 2Corenne Hope ObadoОценок пока нет
- PRC Forms - Blank FormДокумент5 страницPRC Forms - Blank FormAkio OzaragaОценок пока нет
- PRC Forms NewДокумент5 страницPRC Forms NewCiao AtienzaОценок пока нет
- Cross-Training: The Medical Assistant WorkbookОт EverandCross-Training: The Medical Assistant WorkbookОценок пока нет
- Heart of the Field "Refresher & Nha Certification Quick Notes"От EverandHeart of the Field "Refresher & Nha Certification Quick Notes"Оценок пока нет
- For Portfolio LS6 Digital CitizenshipДокумент4 страницыFor Portfolio LS6 Digital CitizenshipDon'tAsK TheStupidOnesОценок пока нет
- Principles of Biology I Lab ManualДокумент75 страницPrinciples of Biology I Lab ManualDon'tAsK TheStupidOnesОценок пока нет
- For Portfolio LS3 Mathematical and Problem Solving SkillsДокумент8 страницFor Portfolio LS3 Mathematical and Problem Solving SkillsDon'tAsK TheStupidOnesОценок пока нет
- For Portfolio LS2 ScienceДокумент7 страницFor Portfolio LS2 ScienceDon'tAsK TheStupidOnesОценок пока нет
- For Portfolio LS1 EnglishДокумент5 страницFor Portfolio LS1 EnglishDon'tAsK TheStupidOnesОценок пока нет
- Lesson 1 - WHAT IS BIOLOGYДокумент5 страницLesson 1 - WHAT IS BIOLOGYDon'tAsK TheStupidOnesОценок пока нет
- Prelim Exam Reviewer - Biology Lab: by Team Meow Meow (Halimeow and 3 Headed Creature)Документ7 страницPrelim Exam Reviewer - Biology Lab: by Team Meow Meow (Halimeow and 3 Headed Creature)Don'tAsK TheStupidOnesОценок пока нет
- Welcome General Chemistry For Engineering and TechnologistДокумент9 страницWelcome General Chemistry For Engineering and TechnologistDon'tAsK TheStupidOnesОценок пока нет
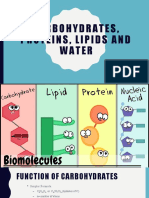
- Lesson 2 - Water, CarbohydratesДокумент22 страницыLesson 2 - Water, CarbohydratesDon'tAsK TheStupidOnesОценок пока нет
- Quiz 1-ChemДокумент2 страницыQuiz 1-ChemDon'tAsK TheStupidOnesОценок пока нет
- Gibbs WorksheetДокумент4 страницыGibbs WorksheetDon'tAsK TheStupidOnesОценок пока нет
- Quiz 2 - ChemДокумент3 страницыQuiz 2 - ChemDon'tAsK TheStupidOnesОценок пока нет
- Int Ener SolnsДокумент3 страницыInt Ener SolnsDon'tAsK TheStupidOnesОценок пока нет
- Global Warming: Public Health Impacts and SolutionsДокумент45 страницGlobal Warming: Public Health Impacts and SolutionsDon'tAsK TheStupidOnesОценок пока нет
- Bomb Calorimetry Practice ProblemsДокумент2 страницыBomb Calorimetry Practice ProblemsDon'tAsK TheStupidOnesОценок пока нет
- UNIVERSAL COLLEGE OF PARANAQUE. FinalsДокумент26 страницUNIVERSAL COLLEGE OF PARANAQUE. FinalsDon'tAsK TheStupidOnesОценок пока нет
- Lp8 - DIgestive System DiseasesДокумент4 страницыLp8 - DIgestive System DiseasesTeacher OliОценок пока нет
- Pediatric Cardiac Arrest AlgorithmДокумент27 страницPediatric Cardiac Arrest AlgorithmLinna AndrianiОценок пока нет
- PolicySoftCopy 201910201120390513 5dabf5af537a7b2e32033e06 PDFДокумент35 страницPolicySoftCopy 201910201120390513 5dabf5af537a7b2e32033e06 PDFNaveen KrishnaОценок пока нет
- Burns SeminarДокумент66 страницBurns SeminarPratibha Thakur100% (1)
- Parasitology - TrematodesДокумент16 страницParasitology - TrematodesMarlex SuanОценок пока нет
- AAST Renal Injury ScaleДокумент11 страницAAST Renal Injury ScaleyuenkeithОценок пока нет
- Get Your Life Back Thyroid Health MANUAL PDF 1 by Kim Wolinski FINALДокумент52 страницыGet Your Life Back Thyroid Health MANUAL PDF 1 by Kim Wolinski FINALKrn Glez100% (8)
- The Effect of 3.2% and 3.8% Sodium CitrateДокумент6 страницThe Effect of 3.2% and 3.8% Sodium CitrateBambang KurniawanОценок пока нет
- Renal Function TestsДокумент23 страницыRenal Function TestsKer YehunОценок пока нет
- Module 4 Assignment PosterДокумент1 страницаModule 4 Assignment PosterChelsie Rachelle BrownОценок пока нет
- Pediatrics:: History Taking and Physical Examination of AdolescentsДокумент14 страницPediatrics:: History Taking and Physical Examination of AdolescentsJüdith Marie Reyes BauntoОценок пока нет
- Cardiac Glycosides 815Документ19 страницCardiac Glycosides 815SanskritiОценок пока нет
- Obat Katalog Tahun 2017Документ96 страницObat Katalog Tahun 2017Aqim Apa AdanyaОценок пока нет
- Personalized Acute Kidney Injury TreatmentДокумент8 страницPersonalized Acute Kidney Injury TreatmentGabriela PachecoОценок пока нет
- Kuliah Dermato Terapi 2013Документ46 страницKuliah Dermato Terapi 2013Vania EssiandaОценок пока нет
- Internship Report Noor Arshad 28Документ80 страницInternship Report Noor Arshad 28hammadОценок пока нет
- Individual SOAP Note ExampleДокумент2 страницыIndividual SOAP Note ExampleAneesaОценок пока нет
- Chapter 46 Antianginal AgentsДокумент14 страницChapter 46 Antianginal AgentsJewel SantosОценок пока нет
- Open Heart Surgery CaabgДокумент6 страницOpen Heart Surgery CaabgGopi KrishnanОценок пока нет
- What Is Anorexia NervosaДокумент2 страницыWhat Is Anorexia NervosaHe DoloresОценок пока нет
- Badie 2004Документ11 страницBadie 2004Bhayu Rizallinoor BhayuОценок пока нет
- (Ha Lab) Sas#9Документ9 страниц(Ha Lab) Sas#9Erwin RomeroОценок пока нет
- 2010 Orthopaedic JournalДокумент80 страниц2010 Orthopaedic JournalPooria1989Оценок пока нет
- Pulmonary Artery CatheterДокумент32 страницыPulmonary Artery Catheterwaqas_xs100% (1)
- Reading - Age With Moderate DehydrationДокумент8 страницReading - Age With Moderate DehydrationSophia IbuyanОценок пока нет
- Nursing Board Exam Topics and Questions June 2009Документ3 страницыNursing Board Exam Topics and Questions June 2009menuloud33% (3)
- Case Proforma Final, SurgeryДокумент37 страницCase Proforma Final, SurgeryDiwakesh C B100% (4)
- Physiotherapy Management of TMJ PainДокумент4 страницыPhysiotherapy Management of TMJ Painakheel ahammed100% (1)
- Teaching Plan For PidДокумент5 страницTeaching Plan For PidokaciaОценок пока нет