Вам также может понравиться
- Cover PageДокумент1 страницаCover PagehafizahhoshniОценок пока нет
- Dermatology Year 4 Batch 4Документ5 страницDermatology Year 4 Batch 4hafizahhoshniОценок пока нет
- Anaesthesiology Year 4 Batch 4Документ4 страницыAnaesthesiology Year 4 Batch 4hafizahhoshniОценок пока нет
- Ygb4g1 Im TheoryДокумент7 страницYgb4g1 Im TheoryhafizahhoshniОценок пока нет
- Ent Year 4 Batch 4Документ2 страницыEnt Year 4 Batch 4hafizahhoshniОценок пока нет
- Hafizah Binti Mohd HoshniДокумент1 страницаHafizah Binti Mohd HoshnihafizahhoshniОценок пока нет
- Benign Hepatobiliary DisordersДокумент29 страницBenign Hepatobiliary DisordershafizahhoshniОценок пока нет
- Hafizah Binti Mohd Hsohni Musculoskeletal Anatomy Chest TraumaДокумент47 страницHafizah Binti Mohd Hsohni Musculoskeletal Anatomy Chest TraumahafizahhoshniОценок пока нет
- FORENSIC: End Posting Exam - 5 JANUARY 2018 Year 4 Batch 4 MCQДокумент5 страницFORENSIC: End Posting Exam - 5 JANUARY 2018 Year 4 Batch 4 MCQhafizahhoshniОценок пока нет
- Hafizah Hoshni PneumothoraxДокумент47 страницHafizah Hoshni PneumothoraxhafizahhoshniОценок пока нет
- Hafizah Hoshni Truth TellingДокумент14 страницHafizah Hoshni Truth TellinghafizahhoshniОценок пока нет
- 2 Hafizah Hoshni ConfidentialityДокумент16 страниц2 Hafizah Hoshni ConfidentialityhafizahhoshniОценок пока нет
- Anatomy Abdominal Wall and HerniasДокумент23 страницыAnatomy Abdominal Wall and HerniashafizahhoshniОценок пока нет
- Hafizah Binti Mohd Hoshni Musculoskeletal Anatomy Abdominal WallДокумент42 страницыHafizah Binti Mohd Hoshni Musculoskeletal Anatomy Abdominal WallhafizahhoshniОценок пока нет
- Hafizah Binti Mohd Hoshni Musculoskeletal Anatomy Skeleton of The ThoraxДокумент28 страницHafizah Binti Mohd Hoshni Musculoskeletal Anatomy Skeleton of The ThoraxhafizahhoshniОценок пока нет
- Epidemiology of CVD DiseasesДокумент19 страницEpidemiology of CVD DiseaseshafizahhoshniОценок пока нет
- Electrophysiology of HeartДокумент46 страницElectrophysiology of HearthafizahhoshniОценок пока нет
- Development of Heart Part 1Документ60 страницDevelopment of Heart Part 1hafizahhoshniОценок пока нет
- Fats and Water Soluble VitaminsДокумент31 страницаFats and Water Soluble VitaminshafizahhoshniОценок пока нет
- Mr. Raja - (Shortness of Breath and Cough) : History of Present IllnessДокумент3 страницыMr. Raja - (Shortness of Breath and Cough) : History of Present IllnesshafizahhoshniОценок пока нет
- Paper 1 Cardiovascular SystemДокумент2 страницыPaper 1 Cardiovascular SystemhafizahhoshniОценок пока нет
- Students Copy - Chest PainДокумент1 страницаStudents Copy - Chest PainhafizahhoshniОценок пока нет
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (400)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- Driving Pressure Study OLVДокумент13 страницDriving Pressure Study OLVlucasОценок пока нет
- Guideline Title: Intra-Aortic Balloon Pump ManagementДокумент16 страницGuideline Title: Intra-Aortic Balloon Pump ManagementJansen ChОценок пока нет
- Lecture 1 Mechanical Ventilation An IntroductionДокумент20 страницLecture 1 Mechanical Ventilation An IntroductionEng Kian NgОценок пока нет
- The Attachments of The Breast To The Chest Wall: A Dissection StudyДокумент12 страницThe Attachments of The Breast To The Chest Wall: A Dissection StudyjuanrangoneОценок пока нет
- Budget Plan Wound ClinicДокумент4 страницыBudget Plan Wound ClinicRegalado Aguhayon100% (1)
- Instructions: Operation ManualДокумент104 страницыInstructions: Operation ManualLatif Fathul EvendiОценок пока нет
- Anatomy and PhysiologyДокумент28 страницAnatomy and PhysiologyeliseudesafateОценок пока нет
- Gastrointestinal System DisordersДокумент112 страницGastrointestinal System DisordersTaate MohammedОценок пока нет
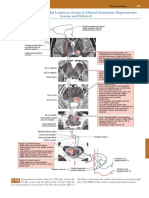
- Posterior Column-Medial Lemniscus System in Clinical Orientation: Representative Lesions and DeficitsДокумент1 страницаPosterior Column-Medial Lemniscus System in Clinical Orientation: Representative Lesions and DeficitsEduardo RodriguezОценок пока нет
- Management of Surgical Scars: Grace Lee Peng,, Julia L. KerolusДокумент5 страницManagement of Surgical Scars: Grace Lee Peng,, Julia L. Kerolusban huỳnhОценок пока нет
- Step 2ck Important (AutoRecovered)Документ101 страницаStep 2ck Important (AutoRecovered)Aishwarya SridharОценок пока нет
- Port A CathДокумент14 страницPort A CathMerika JimenezОценок пока нет
- Past Question NursingДокумент37 страницPast Question NursingOpeyemi Omolabake67% (3)
- New Deadline For Submission of AbstractsДокумент2 страницыNew Deadline For Submission of AbstractsmanognaaaaОценок пока нет
- Sedation Vacation in Neurocritical Care: A Proposal AlgorithmДокумент3 страницыSedation Vacation in Neurocritical Care: A Proposal Algorithmrodolfo riosОценок пока нет
- Constrictive PericarditisДокумент5 страницConstrictive Pericarditisvicky3101Оценок пока нет
- Stainless Steel Crowns PDFДокумент4 страницыStainless Steel Crowns PDFLuciaTrinovenaLaseОценок пока нет
- Catheters and Guide Wires: Presenter: Omkar Gaonkar Course: M.SC., Mit 2 SEM Moderator: Kayalvizhi R DATE:26/03/2019Документ42 страницыCatheters and Guide Wires: Presenter: Omkar Gaonkar Course: M.SC., Mit 2 SEM Moderator: Kayalvizhi R DATE:26/03/2019Omkar GaonkarОценок пока нет
- Core Concepts For Local RN ExamsДокумент16 страницCore Concepts For Local RN ExamsChantilly Marie VillarinОценок пока нет
- Hassan - Pediatric TraumaДокумент12 страницHassan - Pediatric TraumaRicardo GrilloОценок пока нет
- UntitledДокумент10 страницUntitledMashkat AbdelwahabОценок пока нет
- Introduction To NeuroanatomyДокумент20 страницIntroduction To NeuroanatomySurjagnee SannyamatОценок пока нет
- 1) BiopsyДокумент30 страниц1) BiopsySosa GeorgeОценок пока нет
- AuscultationДокумент41 страницаAuscultationAnonymous ZUaUz1wwОценок пока нет
- Red Flag Symptoms - Abdominal Pain - GPonlineДокумент7 страницRed Flag Symptoms - Abdominal Pain - GPonlinedrsadafrafiОценок пока нет
- Parasagittal MeningiomaДокумент51 страницаParasagittal MeningiomaAji Setia UtamaОценок пока нет
- Tatalaksana Dan Prognosis Tumor PeriampullarДокумент16 страницTatalaksana Dan Prognosis Tumor PeriampullarVerico PratamaОценок пока нет
- CPC PancreatitisДокумент67 страницCPC PancreatitisM. Baidar SaeedОценок пока нет
- Benign Tumors of UterusДокумент44 страницыBenign Tumors of UterusZunaira ZahraОценок пока нет