Вам также может понравиться
- Application Assessment IEMRT June 2020 Version ENДокумент7 страницApplication Assessment IEMRT June 2020 Version ENnotanonyuserОценок пока нет
- CCC CCEapplicДокумент2 страницыCCC CCEapplicrupukrisОценок пока нет
- Form 2021 22 Mbbs UpdatedДокумент4 страницыForm 2021 22 Mbbs UpdatedAqsaОценок пока нет
- Undergraduate Application Form-23022022Документ2 страницыUndergraduate Application Form-23022022bongisebodgeОценок пока нет
- Undertaking For Caste Validity Certificate For Maharashtra State Candidates Taking Admission in The Nit+ System To The Verifying Centre In-ChargeДокумент1 страницаUndertaking For Caste Validity Certificate For Maharashtra State Candidates Taking Admission in The Nit+ System To The Verifying Centre In-ChargeDysonОценок пока нет
- 캐나다 VCC International Education Application FormДокумент4 страницы캐나다 VCC International Education Application FormJoins 세계유학Оценок пока нет
- Provider & Order Information: Fax Completed Form To 844-870-8875Документ1 страницаProvider & Order Information: Fax Completed Form To 844-870-8875BrianОценок пока нет
- Dube Trade Port Application FormДокумент7 страницDube Trade Port Application FormNcediswaОценок пока нет
- Scholar SchemeДокумент5 страницScholar SchemeShravan ReddyОценок пока нет
- CMC Vellore Fellowship in Infectious Diseases Application FormДокумент7 страницCMC Vellore Fellowship in Infectious Diseases Application FormNick AОценок пока нет
- Senior Residents & Senior Demonstrators - Annexure 1 & IIДокумент3 страницыSenior Residents & Senior Demonstrators - Annexure 1 & IIsarath6872Оценок пока нет
- Ncert Form-2022Документ6 страницNcert Form-2022suyashy143Оценок пока нет
- Philippine College of Occupational Medicine, Inc. (PCOM)Документ3 страницыPhilippine College of Occupational Medicine, Inc. (PCOM)Kat S. Paule, MDОценок пока нет
- Re Admission FormДокумент2 страницыRe Admission FormMissy SamanthaОценок пока нет
- 1 (T) Air SQN NCC, Secunderabad Risk Certifiate: Signature of CO UnitДокумент2 страницы1 (T) Air SQN NCC, Secunderabad Risk Certifiate: Signature of CO UnitAmarnath ReddyОценок пока нет
- Graduate App FormДокумент7 страницGraduate App FormmahmoudОценок пока нет
- LOCAL SCHOLARSHIP APPLICATIONДокумент4 страницыLOCAL SCHOLARSHIP APPLICATIONCHRISTOPHER SCALE100% (1)
- NOTICEДокумент5 страницNOTICEJohn Phillipp MacaraigОценок пока нет
- Subject:-Undertaking For Caste Validity CertificateДокумент1 страницаSubject:-Undertaking For Caste Validity CertificateDannyОценок пока нет
- IFOM Clinical Science Examination Application Form AY 2017-2018Документ2 страницыIFOM Clinical Science Examination Application Form AY 2017-2018ArchanaОценок пока нет
- Nafteeday Gacalo13Документ6 страницNafteeday Gacalo13stpvpxdv5cОценок пока нет
- Part A. Personal Information: Membership Application FormДокумент3 страницыPart A. Personal Information: Membership Application Formriya RoyОценок пока нет
- Application For Admission: Please Note: This Entire Form Is To Be Completed by The Applicant. Please Print ClearlyДокумент3 страницыApplication For Admission: Please Note: This Entire Form Is To Be Completed by The Applicant. Please Print ClearlyJanuhu ZakaryОценок пока нет
- Office of The Executive Secretary of The Supreme Court of VirginiaДокумент6 страницOffice of The Executive Secretary of The Supreme Court of VirginiaDR LIMBOОценок пока нет
- AOY Registration Form 2020V3Документ2 страницыAOY Registration Form 2020V3PaulОценок пока нет
- Emp Application Revised Feb 2006Документ4 страницыEmp Application Revised Feb 2006Rachel HensleyОценок пока нет
- SSSI ApplicationFormForEmployment-V3.0 1633574829Документ2 страницыSSSI ApplicationFormForEmployment-V3.0 1633574829renierarong18Оценок пока нет
- Division of Graduate Medical Studies: Yong Loo Lin School of MedicineДокумент5 страницDivision of Graduate Medical Studies: Yong Loo Lin School of MedicinebloresamОценок пока нет
- Certified Professional in Supply Management Application For RecertificationДокумент5 страницCertified Professional in Supply Management Application For RecertificationVikash GuptaОценок пока нет
- History Form For AdultsДокумент9 страницHistory Form For AdultsFazal HaqueОценок пока нет
- CEMAP - Recognition-Of-Prior-Learning-Rpl-02-21-IntДокумент2 страницыCEMAP - Recognition-Of-Prior-Learning-Rpl-02-21-IntMike HendersonОценок пока нет
- Postgraduate Application FormДокумент3 страницыPostgraduate Application Formsisay gebremariamОценок пока нет
- GZU Postgraduate Application FormДокумент6 страницGZU Postgraduate Application FormRamin Le MiexОценок пока нет
- ANSYS Explicit STR (Autodyn Part 1) PDFДокумент3 страницыANSYS Explicit STR (Autodyn Part 1) PDFnguyenhОценок пока нет
- Applicant Application FormДокумент6 страницApplicant Application FormJocelyn Joy ArcegaОценок пока нет
- 42bb5 c1f75 Application Form For Mos DoctorsДокумент2 страницы42bb5 c1f75 Application Form For Mos DoctorsDanish KhanОценок пока нет
- AA Claim FormДокумент5 страницAA Claim FormpenchanskyОценок пока нет
- IMA FormДокумент3 страницыIMA FormSandeep OdelaОценок пока нет
- Application form for Henley MBAДокумент6 страницApplication form for Henley MBALars Peter HammelОценок пока нет
- Indemnity BondДокумент1 страницаIndemnity BondKhader BashaОценок пока нет
- Ged Test Accom App AdhdДокумент7 страницGed Test Accom App AdhdJeannette DorfmanОценок пока нет
- Electronic CKK 2018 AIT ApplicationДокумент5 страницElectronic CKK 2018 AIT ApplicationAnonymous kMFSq9ayGОценок пока нет
- UP College of Law Application for Law Aptitude ExamДокумент3 страницыUP College of Law Application for Law Aptitude ExamAngelica Fojas RañolaОценок пока нет
- Ned University of Engineering and Technology Examinations Department Degree Application FormДокумент2 страницыNed University of Engineering and Technology Examinations Department Degree Application FormAbdul RashidОценок пока нет
- Application For Flight Training in Canada 2022Документ3 страницыApplication For Flight Training in Canada 2022Abdur RehmanОценок пока нет
- TW-SH-CCIC Duplicate Certificate Proforma - 482.Документ4 страницыTW-SH-CCIC Duplicate Certificate Proforma - 482.Tirupati TirumalaОценок пока нет
- EFRCFC InstAppДокумент1 страницаEFRCFC InstAppBeste1979Оценок пока нет
- Honors College Undergraduate Petition: I RequestДокумент2 страницыHonors College Undergraduate Petition: I RequestEric MoralesОценок пока нет
- DAP - Fillable - Nomination - Application FormДокумент1 страницаDAP - Fillable - Nomination - Application FormRye SteveyОценок пока нет
- International: Application For MembershipДокумент4 страницыInternational: Application For MembershipManuelEduardoSanchezSotoОценок пока нет
- Resident Leadership Program App Packet - Nov2018Документ6 страницResident Leadership Program App Packet - Nov2018Subhasis RoyОценок пока нет
- Apply for ICAI Goodstanding CertificateДокумент1 страницаApply for ICAI Goodstanding Certificateak9754197Оценок пока нет
- Cap College Foundation, Inc. Request For School Credentials: Check The Credentials Being RequestedДокумент1 страницаCap College Foundation, Inc. Request For School Credentials: Check The Credentials Being RequestedChristian HizolaОценок пока нет
- TransferapplicationformДокумент3 страницыTransferapplicationformKamera RightОценок пока нет
- Enrolment Form - LAA - Rev...Документ3 страницыEnrolment Form - LAA - Rev...ynkbjtdrjzОценок пока нет
- Enrollment AppДокумент10 страницEnrollment Appapi-218391675Оценок пока нет
- Application Forms Agniveervayu Non-Combatants 02 23Документ4 страницыApplication Forms Agniveervayu Non-Combatants 02 23sudeepchhetri41Оценок пока нет
- Clinical Referral FormДокумент2 страницыClinical Referral FormJan Oneille Y. VallesОценок пока нет
- Form 176 MDB Ecfmg2Документ10 страницForm 176 MDB Ecfmg2Swati TyagiОценок пока нет
- Clerk (Income Maintenance): Passbooks Study GuideОт EverandClerk (Income Maintenance): Passbooks Study GuideОценок пока нет
- Body Weight and Skinfold Thickness in AnДокумент10 страницBody Weight and Skinfold Thickness in AnKalina MassetОценок пока нет
- 2009 Progression Models in ACSMДокумент22 страницы2009 Progression Models in ACSMgustavo10bbmОценок пока нет
- JEP Journal of Exercise Physiology: OnlineДокумент60 страницJEP Journal of Exercise Physiology: OnlineadianjoОценок пока нет
- Technical Report PDFДокумент336 страницTechnical Report PDFKalina MassetОценок пока нет
- Risk of Adverse Pregnancy Out Comes in Women With Polycystic Ovary Syndrome Populationbasedcohort StudyДокумент9 страницRisk of Adverse Pregnancy Out Comes in Women With Polycystic Ovary Syndrome Populationbasedcohort StudyKalina MassetОценок пока нет
- Definição de Qualidade de Vida e IdososДокумент9 страницDefinição de Qualidade de Vida e IdososKalina MassetОценок пока нет
- Week 5 WHLP Nov. 2 6 2020 DISSДокумент5 страницWeek 5 WHLP Nov. 2 6 2020 DISSDaniel BandibasОценок пока нет
- Invoice Inv0006: Er. Mohamed Irshadh P MДокумент1 страницаInvoice Inv0006: Er. Mohamed Irshadh P Mmanoj100% (1)
- Corporate Office Design GuideДокумент23 страницыCorporate Office Design GuideAshfaque SalzОценок пока нет
- Business Data Communications and Networking 13Th Edition Fitzgerald Test Bank Full Chapter PDFДокумент40 страницBusiness Data Communications and Networking 13Th Edition Fitzgerald Test Bank Full Chapter PDFthrongweightypfr100% (12)
- Little Match GirlДокумент8 страницLittle Match GirlsubhaseduОценок пока нет
- Bpo Segment by Vitthal BhawarДокумент59 страницBpo Segment by Vitthal Bhawarvbhawar1141100% (1)
- Solar Powered Rickshaw PDFДокумент65 страницSolar Powered Rickshaw PDFPrãvëèñ Hêgådë100% (1)
- I Saw Water Flowing - VaticanДокумент3 страницыI Saw Water Flowing - VaticanChu Gia KhôiОценок пока нет
- TOPIC 12 Soaps and DetergentsДокумент14 страницTOPIC 12 Soaps and DetergentsKaynine Kiko50% (2)
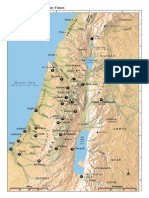
- Israel Bible MapДокумент1 страницаIsrael Bible MapMoses_JakkalaОценок пока нет
- Relay Models Per Types Mdp38 EnuДокумент618 страницRelay Models Per Types Mdp38 Enuazer NadingaОценок пока нет
- Httpswww.ceec.Edu.twfilesfile Pool10j07580923432342090202 97指考英文試卷 PDFДокумент8 страницHttpswww.ceec.Edu.twfilesfile Pool10j07580923432342090202 97指考英文試卷 PDFAurora ZengОценок пока нет
- Exam SE UZДокумент2 страницыExam SE UZLovemore kabbyОценок пока нет
- Special Blood CollectionДокумент99 страницSpecial Blood CollectionVenomОценок пока нет
- SPACES Nepal - Green Schools Building The FutureДокумент3 страницыSPACES Nepal - Green Schools Building The FutureBimal ThapaОценок пока нет
- Cignal Channel 490Документ2 страницыCignal Channel 490Arild JuliusОценок пока нет
- Strategic Planning and Program Budgeting in Romania RecentДокумент6 страницStrategic Planning and Program Budgeting in Romania RecentCarmina Ioana TomariuОценок пока нет
- Saic P 3311Документ7 страницSaic P 3311Arshad ImamОценок пока нет
- Tattva Sandoha PujaДокумент2 страницыTattva Sandoha PujaSathis KumarОценок пока нет
- Under the Angels Restaurant Transports Guests to Old CracowДокумент2 страницыUnder the Angels Restaurant Transports Guests to Old CracowBence KlusóczkiОценок пока нет
- 4TH Quarter English 10 Assessment TestДокумент6 страниц4TH Quarter English 10 Assessment TestafbnjkcdОценок пока нет
- 1 Ancient-IndiaДокумент14 страниц1 Ancient-Indiakaushik joshiОценок пока нет
- Unitrain I Overview enДокумент1 страницаUnitrain I Overview enDragoi MihaiОценок пока нет
- Line GraphДокумент13 страницLine GraphMikelAgberoОценок пока нет
- Business Beyond Profit Motivation Role of Employees As Decision-Makers in The Business EnterpriseДокумент6 страницBusiness Beyond Profit Motivation Role of Employees As Decision-Makers in The Business EnterpriseCaladhiel100% (1)
- Writing Assessment and Evaluation Checklist - PeerДокумент1 страницаWriting Assessment and Evaluation Checklist - PeerMarlyn Joy YaconОценок пока нет
- General Physics 1: Activity Title: What Forces You? Activity No.: 1.3 Learning Competency: Draw Free-Body DiagramsДокумент5 страницGeneral Physics 1: Activity Title: What Forces You? Activity No.: 1.3 Learning Competency: Draw Free-Body DiagramsLeonardo PigaОценок пока нет
- #1 HR Software in Sudan-Khartoum-Omdurman-Nyala-Port-Sudan - HR System - HR Company - HR SolutionДокумент9 страниц#1 HR Software in Sudan-Khartoum-Omdurman-Nyala-Port-Sudan - HR System - HR Company - HR SolutionHishamОценок пока нет
- History: The Origin of Kho-KhotheДокумент17 страницHistory: The Origin of Kho-KhotheIndrani BhattacharyaОценок пока нет
- TAFC R10 SP54 Release NotesДокумент10 страницTAFC R10 SP54 Release NotesBejace NyachhyonОценок пока нет