Вам также может понравиться
- Hema II Chapter11 - QA in HematologyДокумент29 страницHema II Chapter11 - QA in HematologyAmanuel MaruОценок пока нет
- Hematology II Notes - MagtalasДокумент12 страницHematology II Notes - MagtalasAbhugz VosotrosОценок пока нет
- Clinial MicrosДокумент53 страницыClinial MicrosDreyden HaloОценок пока нет
- Blood Type Review WorksheetДокумент2 страницыBlood Type Review WorksheetSofa100% (2)
- Relevance of Serum Tumor MarkersДокумент25 страницRelevance of Serum Tumor MarkersDrPawan KirtaniОценок пока нет
- Hematology BMLS 103Документ88 страницHematology BMLS 103harpreetОценок пока нет
- 8 Part Eye Exam RevisedДокумент17 страниц8 Part Eye Exam RevisedpasambalyrradjohndarОценок пока нет
- 8 Part Eye Exam RevisedДокумент17 страниц8 Part Eye Exam RevisedpasambalyrradjohndarОценок пока нет
- Clinical Chemistry 2 Lecture Notes in Trace ElementsДокумент6 страницClinical Chemistry 2 Lecture Notes in Trace ElementsMoira Pauline LibroraniaОценок пока нет
- Psych Osce Reviewer 1Документ10 страницPsych Osce Reviewer 1pasambalyrradjohndarОценок пока нет
- Psych Osce Reviewer 1Документ10 страницPsych Osce Reviewer 1pasambalyrradjohndarОценок пока нет
- Defining The Practice of Medical Technology or Clinical Laboratory Science ProfessionДокумент27 страницDefining The Practice of Medical Technology or Clinical Laboratory Science ProfessionKianna TicsayОценок пока нет
- Blood SmearДокумент2 страницыBlood SmearSolomon RotimiОценок пока нет
- Lec1 Introduction To Immunohematology1Документ20 страницLec1 Introduction To Immunohematology1Dalia M. MohsenОценок пока нет
- Autoimmune Hemolytic AnemiaДокумент55 страницAutoimmune Hemolytic AnemiaNicky SebastianОценок пока нет
- Blood Groups & Blood BankingДокумент36 страницBlood Groups & Blood BankingGodfrey Pizaroh Mujuzi100% (2)
- Blood Transfusion ManualДокумент35 страницBlood Transfusion ManualSaradha PellatiОценок пока нет
- Laboratory Evaluation of PlateletsДокумент28 страницLaboratory Evaluation of PlateletsTom Anthony TonguiaОценок пока нет
- Blood Bank TypingДокумент34 страницыBlood Bank TypingSkylarОценок пока нет
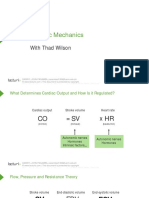
- Cardiac Mechanics: With Thad WilsonДокумент26 страницCardiac Mechanics: With Thad WilsonpasambalyrradjohndarОценок пока нет
- Oral Rehydration TherapyДокумент12 страницOral Rehydration TherapypasambalyrradjohndarОценок пока нет
- Peripheral Smear ExaminationДокумент75 страницPeripheral Smear ExaminationMoorthi100% (1)
- Cross Matching-Wps OfficeДокумент22 страницыCross Matching-Wps Officeashwini priyaОценок пока нет
- Week10 Immunohematologypart1Документ158 страницWeek10 Immunohematologypart1Micah Daniel TapiaОценок пока нет
- Blood BasicsДокумент30 страницBlood Basicskholoud220Оценок пока нет
- Platelets: o Serotonin, ADP & ATP o Destroyed by RESДокумент7 страницPlatelets: o Serotonin, ADP & ATP o Destroyed by RESEunice AndradeОценок пока нет
- Hematology 2 Topic 2 Prelim2222Документ73 страницыHematology 2 Topic 2 Prelim2222Mary Lyka ReyesОценок пока нет
- Blood Bank UnitДокумент9 страницBlood Bank UnitMary CabalceОценок пока нет
- Group 6 - Immunohematology - Blood BankingДокумент8 страницGroup 6 - Immunohematology - Blood Bankingjulo_05Оценок пока нет
- PATHO 1.01a Cellular Response To Stress and Toxic Insults Part I - YanezДокумент8 страницPATHO 1.01a Cellular Response To Stress and Toxic Insults Part I - Yanezpasambalyrradjohndar100% (1)
- Cerebrospinal Fluid: By: Raynhier G. Constantino, RMTДокумент53 страницыCerebrospinal Fluid: By: Raynhier G. Constantino, RMTJaellah MatawaОценок пока нет
- WBC Diff CountДокумент47 страницWBC Diff CountPogo LocoОценок пока нет
- UrinalysisДокумент36 страницUrinalysisMarl EstradaОценок пока нет
- ImmunohematologyДокумент38 страницImmunohematologyNoreenОценок пока нет
- Assessment and Management of Patients With Hematologic DisordersДокумент20 страницAssessment and Management of Patients With Hematologic Disorderschristine mercado100% (1)
- Adverse Reaction Blood BankДокумент10 страницAdverse Reaction Blood BankyourfamilydoctorОценок пока нет
- Hematology PDFДокумент85 страницHematology PDFammarОценок пока нет
- Wardclass Powerpoint Blood TransfusionДокумент27 страницWardclass Powerpoint Blood TransfusionKatherine 'Chingboo' Leonico Laud60% (5)
- Blood Bank ProceduresДокумент33 страницыBlood Bank Procedures99noname100% (1)
- Promissory NoteДокумент1 страницаPromissory NotepasambalyrradjohndarОценок пока нет
- Blood ComponentДокумент17 страницBlood ComponentJes CmtОценок пока нет
- Chapter Blood: RBC Platelet HemostasisДокумент89 страницChapter Blood: RBC Platelet Hemostasisapi-19916399100% (1)
- Blood BankingДокумент7 страницBlood BankingRoiland Atienza BaybayonОценок пока нет
- Manual Platelet CountДокумент14 страницManual Platelet CountMiyo SobremisanaОценок пока нет
- Cross MatchingДокумент3 страницыCross MatchingTP RMad100% (7)
- 1 Edited My Class Note 1 On Blood BankДокумент42 страницы1 Edited My Class Note 1 On Blood Bankmatewos100% (1)
- Alloimmunisation To Blood Group AntigensДокумент34 страницыAlloimmunisation To Blood Group AntigensbloodbankОценок пока нет
- Automation in HaematologyДокумент67 страницAutomation in Haematologyk11a1r18Оценок пока нет
- CBC Reviewer Anaphy LabДокумент9 страницCBC Reviewer Anaphy LabARVINE JUSTINE CORPUZОценок пока нет
- Abs Elu HandoutДокумент6 страницAbs Elu HandoutSiti Fadhilla TsabithaОценок пока нет
- Lesson 5: Nature of The Clinical LaboratoryДокумент8 страницLesson 5: Nature of The Clinical LaboratoryJohn Daniel AriasОценок пока нет
- Hemoglobin DeterminationДокумент1 страницаHemoglobin DeterminationLecture NotesОценок пока нет
- Lecture On Blood Groups, Transfusion, RH Incompatibility by Dr. RoomiДокумент41 страницаLecture On Blood Groups, Transfusion, RH Incompatibility by Dr. RoomiMudassar Roomi100% (1)
- Disorders of Iron Kinetics and Heme MetabolismДокумент12 страницDisorders of Iron Kinetics and Heme MetabolismJoanne JardinОценок пока нет
- CLS 400 - Test 4 (Extra Credit)Документ8 страницCLS 400 - Test 4 (Extra Credit)McNeeseInsiderОценок пока нет
- Thrombopoiesis and Megakaryopoiesis: BY Dr. Etu-Efeotor T. PДокумент22 страницыThrombopoiesis and Megakaryopoiesis: BY Dr. Etu-Efeotor T. PPrincewill SeiyefaОценок пока нет
- Chapter 14 - Routine and Point of Care Testing in HematologyДокумент10 страницChapter 14 - Routine and Point of Care Testing in HematologyNathaniel Sim100% (1)
- Basics of ImmunohematologyДокумент28 страницBasics of ImmunohematologyAkhil ChaudharyОценок пока нет
- Exercise 8 Direct Antiglobulin Test (DAT) : ObjectivesДокумент9 страницExercise 8 Direct Antiglobulin Test (DAT) : ObjectivesTrang HuynhОценок пока нет
- Intro To ImmunohematoДокумент48 страницIntro To Immunohematojong188Оценок пока нет
- Flashcards in Abo Blood GroupДокумент10 страницFlashcards in Abo Blood GroupVincent ReyesОценок пока нет
- Compatibility Testing: Week 5Документ33 страницыCompatibility Testing: Week 5Bridgette100% (1)
- Blood BankДокумент32 страницыBlood Bankpikachu100% (1)
- Compatibility Testing - BloodДокумент5 страницCompatibility Testing - BloodMunish DograОценок пока нет
- Immuno HematologyДокумент35 страницImmuno HematologyAlan McLeanОценок пока нет
- Blood Components Where Do They Come From?: Introduction To HaematologyДокумент11 страницBlood Components Where Do They Come From?: Introduction To Haematologydorsa koraeiОценок пока нет
- Blood Group Systems ISBTДокумент25 страницBlood Group Systems ISBTkusumahpratiwi100% (1)
- 4 - HemoglobinopathiesДокумент19 страниц4 - HemoglobinopathiesHamzehОценок пока нет
- BMED425 20130926124157 SyllabusДокумент8 страницBMED425 20130926124157 Syllabusahmad0% (1)
- Hematology 1 Lab - The Reticulocyte CountДокумент17 страницHematology 1 Lab - The Reticulocyte CountCIRILO MABBORANGОценок пока нет
- (PHA) 2.13 Immunopharmacology - Dr. Marbella PDFДокумент10 страниц(PHA) 2.13 Immunopharmacology - Dr. Marbella PDFpasambalyrradjohndarОценок пока нет
- Cardiology An Introduction: 12 Cardiomyopathy With Joseph S. Alpert, M.DДокумент36 страницCardiology An Introduction: 12 Cardiomyopathy With Joseph S. Alpert, M.DpasambalyrradjohndarОценок пока нет
- Application For Academic RecordДокумент1 страницаApplication For Academic RecordpasambalyrradjohndarОценок пока нет
- Monthly Blood Glucose Diary PDFДокумент1 страницаMonthly Blood Glucose Diary PDFpasambalyrradjohndarОценок пока нет
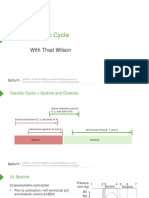
- Cardiac Cycle: With Thad WilsonДокумент25 страницCardiac Cycle: With Thad WilsonpasambalyrradjohndarОценок пока нет
- Loop Diuretics: Producers of The Greatest Diuresis With Rhonda LawesДокумент23 страницыLoop Diuretics: Producers of The Greatest Diuresis With Rhonda LawespasambalyrradjohndarОценок пока нет
- Recording The Medical HistoryДокумент8 страницRecording The Medical HistorypasambalyrradjohndarОценок пока нет
- A Cross-Sectional Study On The Association Between Screen Time Exposure and Concentration Among Undergraduate University Students of UermmmciДокумент3 страницыA Cross-Sectional Study On The Association Between Screen Time Exposure and Concentration Among Undergraduate University Students of UermmmcipasambalyrradjohndarОценок пока нет
- Amoeba: Cytoplasm (Both in Cyst and Peripheral Chromatin (Both Trophozoite Cyst AmoebaДокумент1 страницаAmoeba: Cytoplasm (Both in Cyst and Peripheral Chromatin (Both Trophozoite Cyst AmoebapasambalyrradjohndarОценок пока нет
- Charcoal Tracing Revised - ResultsДокумент3 страницыCharcoal Tracing Revised - ResultspasambalyrradjohndarОценок пока нет
- Assignment Types of Blood DonationДокумент4 страницыAssignment Types of Blood Donationfayzah alshammariОценок пока нет
- ABO and RH Blood Group SystemДокумент31 страницаABO and RH Blood Group SystemKaab Ishaq100% (1)
- Vibrio CholeraeДокумент12 страницVibrio Choleraedorothy kageniОценок пока нет
- Blood Bank Laboratory Assignment 2 - Endterm Ahg TestДокумент5 страницBlood Bank Laboratory Assignment 2 - Endterm Ahg TestAnastasiaОценок пока нет
- KF - 07 - Blood Grouping 2019 - 03 - enДокумент4 страницыKF - 07 - Blood Grouping 2019 - 03 - enSurta DevianaОценок пока нет
- Activity No. 7.1 BloodДокумент2 страницыActivity No. 7.1 BloodDree SermanОценок пока нет
- Dengue NS1Документ1 страницаDengue NS1rajОценок пока нет
- Interpretation: L30 - Para-Cc Shop No 3, Shubh Complex, Para, Old para Thana, para LucknowДокумент5 страницInterpretation: L30 - Para-Cc Shop No 3, Shubh Complex, Para, Old para Thana, para LucknowYogesh BaranwalОценок пока нет
- RH IncompatibilitiesДокумент28 страницRH IncompatibilitiesTofitofi TofiОценок пока нет
- Asbmt: Clinical Guide To ABO-Incompatible Allogeneic Stem Cell TransplantationДокумент7 страницAsbmt: Clinical Guide To ABO-Incompatible Allogeneic Stem Cell TransplantationMohana ReddyОценок пока нет
- Blood TransfusionДокумент5 страницBlood Transfusionrupali gahalianОценок пока нет
- Blood Transfusion Whole Blood: Right Blood Component Right Time Right ReasonДокумент13 страницBlood Transfusion Whole Blood: Right Blood Component Right Time Right ReasonalysalorenoОценок пока нет
- Serum PresentationДокумент22 страницыSerum PresentationPratap MauryaОценок пока нет
- Group 8 A2 Modules 5 7 IMMUNOHEMATOLOGYДокумент4 страницыGroup 8 A2 Modules 5 7 IMMUNOHEMATOLOGYKrystelle Anne PenaflorОценок пока нет
- Diagnostic Tyfoid 1Документ4 страницыDiagnostic Tyfoid 1Roberto SoehartonoОценок пока нет
- Acog Practice Bullet In: Management of Alloimmunization During PregnancyДокумент9 страницAcog Practice Bullet In: Management of Alloimmunization During PregnancyTatiiana ZpiitiiaОценок пока нет
- Preparation of Distilled WaterДокумент23 страницыPreparation of Distilled WaterdesaishantiОценок пока нет
- Branches of ScienceДокумент4 страницыBranches of ScienceEmerald RizaldaОценок пока нет
- Z+blood TransfusionДокумент16 страницZ+blood TransfusionilhamaminsyaputraОценок пока нет
- The RH Blood Group SystemДокумент5 страницThe RH Blood Group SystemKIM KYRISH DELA CRUZОценок пока нет
- IS MIDTERM-mergedДокумент35 страницIS MIDTERM-mergedGennelyn Ross Delos ReyesОценок пока нет
- Robertson 1987Документ4 страницыRobertson 1987parag fОценок пока нет
- Medsurg (112) Rle: Care of Patients With Problems of The Hematologic SystemДокумент5 страницMedsurg (112) Rle: Care of Patients With Problems of The Hematologic SystemChelsea Faith SarandiОценок пока нет
- Histoplasma CapsulatumДокумент20 страницHistoplasma CapsulatumNayrobi GuillénОценок пока нет