Вам также может понравиться
- Chimeric Groin Free Flaps Design and Clinical Application - Microsurgery, Vol. 36 Issue 3 (BZ 22588160)Документ10 страницChimeric Groin Free Flaps Design and Clinical Application - Microsurgery, Vol. 36 Issue 3 (BZ 22588160)Manny TrujilloОценок пока нет
- 1 s2.0 S0749806317312173 MainДокумент8 страниц1 s2.0 S0749806317312173 MaindragaancaОценок пока нет
- Tzaveas 2010Документ6 страницTzaveas 2010moonwalker2099Оценок пока нет
- The Journal of Foot & Ankle SurgeryДокумент4 страницыThe Journal of Foot & Ankle SurgeryEma.diazОценок пока нет
- The Modified Brostr M Gould Procedure - Early Results Usi - 2014 - Foot and AnklДокумент5 страницThe Modified Brostr M Gould Procedure - Early Results Usi - 2014 - Foot and AnklFyodorovich Makarov NikolaiОценок пока нет
- Reconstruction of An Achilles Tendon Defect Utilizing An Achilles Tendon Allograft JFAS 1996Документ8 страницReconstruction of An Achilles Tendon Defect Utilizing An Achilles Tendon Allograft JFAS 1996Evan BowlesОценок пока нет
- Article PDFДокумент9 страницArticle PDFAqsa FarooqОценок пока нет
- E Poster IndriДокумент4 страницыE Poster IndriIndri Pratiwi TobingОценок пока нет
- Management of Displaced Patella Fracture With Modified Tension Band Wiring and Percutaneous Cannulated Screws-A DilemmaДокумент6 страницManagement of Displaced Patella Fracture With Modified Tension Band Wiring and Percutaneous Cannulated Screws-A Dilemmaavinashrao39Оценок пока нет
- Distal Femoral Autograft For Acetabular Reconstruction in THAДокумент7 страницDistal Femoral Autograft For Acetabular Reconstruction in THASeagate PramonoОценок пока нет
- Case Report Indri-Noha FIXДокумент5 страницCase Report Indri-Noha FIXIndri Pratiwi TobingОценок пока нет
- Septic Ligament: ArthroscopicДокумент7 страницSeptic Ligament: ArthroscopicleonardocahyoОценок пока нет
- Anterior Tibial Spine ACL Avulsion Fracture TreateДокумент5 страницAnterior Tibial Spine ACL Avulsion Fracture TreateDyah PurwitaОценок пока нет
- Ankle Stabilization With Arthroscopic Versus Open With Suture Tape Augmentation Techniques X1D XJ. George DeVries PDFДокумент5 страницAnkle Stabilization With Arthroscopic Versus Open With Suture Tape Augmentation Techniques X1D XJ. George DeVries PDFcrpcsxfdkgОценок пока нет
- A Severe Acute Achilles Rupture and Repair JFAS 1995Документ5 страницA Severe Acute Achilles Rupture and Repair JFAS 1995Evan BowlesОценок пока нет
- 11 - 2015 - Outcome Acetabuloplastia y Osteotomia VarizantesДокумент8 страниц11 - 2015 - Outcome Acetabuloplastia y Osteotomia VarizantesDaniel Alejandro Sini RiosОценок пока нет
- 1348 6456 4 PBДокумент7 страниц1348 6456 4 PB林良駿Оценок пока нет
- Seguimiento A 5 Años PTGH ReversaДокумент7 страницSeguimiento A 5 Años PTGH Reversamarcelogascon.oОценок пока нет
- DF W ReconДокумент11 страницDF W ReconPraveen RavishankaranОценок пока нет
- A New Instrument For Surgical Stabilization of Multiple Rib FracturesДокумент9 страницA New Instrument For Surgical Stabilization of Multiple Rib Fracturesduke3443Оценок пока нет
- Clark 1998Документ10 страницClark 1998Yordhanno Xavier Fallaque RuizОценок пока нет
- Resurfacing For Perthes DiseaseДокумент6 страницResurfacing For Perthes Diseaseyarimar hoyosОценок пока нет
- Jurnal PICO No 1Документ6 страницJurnal PICO No 1Dwiky YudhistiraОценок пока нет
- Anterior Versus Posterior Surgical Approach For Lumbosacral TuberculosisДокумент9 страницAnterior Versus Posterior Surgical Approach For Lumbosacral TuberculosisI Made Dhita PriantharaОценок пока нет
- The Journal of Foot & Ankle Surgery: Christopher Bibbo, DO, DPM, FACFASДокумент5 страницThe Journal of Foot & Ankle Surgery: Christopher Bibbo, DO, DPM, FACFASdamonenОценок пока нет
- Painful Knee 2024 International Journal of Surgery Case ReportsДокумент6 страницPainful Knee 2024 International Journal of Surgery Case ReportsRonald QuezadaОценок пока нет
- Capsular Augmentation in Colonna Arthroplasty For The Management of Chronic Hip DislocationДокумент5 страницCapsular Augmentation in Colonna Arthroplasty For The Management of Chronic Hip DislocationFerney Leon BalceroОценок пока нет
- Calcanectomy For OsteomyelitisДокумент7 страницCalcanectomy For OsteomyelitisCleff FlowersОценок пока нет
- Calcified Tendo Achillis Insertion New SX Approach JFAS 1991Документ4 страницыCalcified Tendo Achillis Insertion New SX Approach JFAS 1991Evan BowlesОценок пока нет
- Medicine The American Journal of SportsДокумент8 страницMedicine The American Journal of Sportshieuminhduong7Оценок пока нет
- Use of Reverse Lateral Arm Flap For Coverage of Elbow in Burn PatientsДокумент3 страницыUse of Reverse Lateral Arm Flap For Coverage of Elbow in Burn PatientsPalwasha MalikОценок пока нет
- Ma 2021Документ6 страницMa 2021bigben9262Оценок пока нет
- Arthroscopic Treatment of Anterosuperior Rotator CДокумент8 страницArthroscopic Treatment of Anterosuperior Rotator CGabriel RojasОценок пока нет
- Aaos 2010Документ220 страницAaos 2010Yusufa ArdyОценок пока нет
- Elective Frozen Elephant Trunk Procedure Using The E-Vita Open Plus Prosthesis in 94 Patients: A Multicentre French RegistryДокумент7 страницElective Frozen Elephant Trunk Procedure Using The E-Vita Open Plus Prosthesis in 94 Patients: A Multicentre French RegistryrédaОценок пока нет
- Reconstruction of The Skin Defect of The Knee Using A Reverse Anterolateral Thigh Island FlapДокумент4 страницыReconstruction of The Skin Defect of The Knee Using A Reverse Anterolateral Thigh Island FlapAndrea Del VillarОценок пока нет
- Articles by Dr. Nata ParnesДокумент19 страницArticles by Dr. Nata ParnesWatertown Daily TimesОценок пока нет
- Top Ten Pearls For Successful Hip ArthrosДокумент10 страницTop Ten Pearls For Successful Hip ArthrosMoustafa MohamedОценок пока нет
- Unicompartmental Knee Arthroplasty: Indications, Surgical Techniques and ComplicationsОт EverandUnicompartmental Knee Arthroplasty: Indications, Surgical Techniques and ComplicationsTad L. GerlingerОценок пока нет
- Brief Resume of Intended WorkДокумент7 страницBrief Resume of Intended WorkNavin ChandarОценок пока нет
- Obesity PDFДокумент21 страницаObesity PDFIka Elwinda DariseОценок пока нет
- Synchronous Open Hernioplasty of Primary Bilateral Inguinal HerniaДокумент6 страницSynchronous Open Hernioplasty of Primary Bilateral Inguinal HerniaKhaled MonazeaОценок пока нет
- Flexible 3D Laparoscopic Assisted Reduction andДокумент9 страницFlexible 3D Laparoscopic Assisted Reduction andgevowo3277Оценок пока нет
- 21 JMSCRДокумент6 страниц21 JMSCRRakesh KumarОценок пока нет
- Modified Arthroscopic Latarjet Procedure: Suture-Button Fixation Achieves Excellent Remodeling at 3-Year Follow-UpДокумент9 страницModified Arthroscopic Latarjet Procedure: Suture-Button Fixation Achieves Excellent Remodeling at 3-Year Follow-UpFarida KhodjaОценок пока нет
- Patellar Tendon or Semitendinosus Tendon Autografts For Anterior Cruciate Ligament Reconstruction?Документ7 страницPatellar Tendon or Semitendinosus Tendon Autografts For Anterior Cruciate Ligament Reconstruction?lipemagalhaesОценок пока нет
- 2002 Scarf FundaДокумент9 страниц2002 Scarf FundaRuth Aydeé SoláОценок пока нет
- Functional Outcome External Fixation Dated 17 March, 2021Документ7 страницFunctional Outcome External Fixation Dated 17 March, 2021Arshad khanОценок пока нет
- Analysis of Surgical Management of Proximal Humeral FracturesДокумент5 страницAnalysis of Surgical Management of Proximal Humeral FracturesRhizka djitmauОценок пока нет
- Aao2016 ReconДокумент163 страницыAao2016 ReconAnonymous 43mqs5pElf100% (6)
- Eliasson 2018Документ11 страницEliasson 2018seriesediversosОценок пока нет
- A Modified Boytchev Procedure For Recurrent Anterior Dislocation of The Shoulder Khaled M Mostafa and Kamal El-GafaryДокумент9 страницA Modified Boytchev Procedure For Recurrent Anterior Dislocation of The Shoulder Khaled M Mostafa and Kamal El-GafaryDebangshu KumarОценок пока нет
- Frontolateral Partial LaryngectomyДокумент7 страницFrontolateral Partial LaryngectomyJeremy HermantoОценок пока нет
- Drughelp - Care 6.22Документ10 страницDrughelp - Care 6.22Joko RifaiОценок пока нет
- Double-Pedicle Propeller Flap For Reconstruction of The Foot and Ankle: Anatomical Study and Clinical ApplicationsДокумент12 страницDouble-Pedicle Propeller Flap For Reconstruction of The Foot and Ankle: Anatomical Study and Clinical ApplicationsWulan PurnamiОценок пока нет
- Aps 39 345Документ9 страницAps 39 345isabelОценок пока нет
- Reversetotalshoulder Arthroplasty: Early Results of Forty-One Cases and A Review of The LiteratureДокумент11 страницReversetotalshoulder Arthroplasty: Early Results of Forty-One Cases and A Review of The LiteratureBruno FellipeОценок пока нет
- Transition To Anterior Approach in Primary Total Hip Arthroplasty Learning Curve ComplicationsДокумент7 страницTransition To Anterior Approach in Primary Total Hip Arthroplasty Learning Curve ComplicationsAthenaeum Scientific PublishersОценок пока нет
- 1 s2.0 S2210261217304431 MainДокумент4 страницы1 s2.0 S2210261217304431 MainChristopher BermeoОценок пока нет
- Rajiv Gandhi University of Health Sciences, Bengaluru, KarnatakaДокумент9 страницRajiv Gandhi University of Health Sciences, Bengaluru, KarnatakaNavin ChandarОценок пока нет
- EjercicioДокумент12 страницEjercicioVillateAngelaОценок пока нет
- ALR Brief SedentaryBehaviors IssueBrief May2014Документ1 страницаALR Brief SedentaryBehaviors IssueBrief May2014VillateAngelaОценок пока нет
- Sedentary Behaviors and Youth: Current Trends and The Impact On HealthДокумент12 страницSedentary Behaviors and Youth: Current Trends and The Impact On HealthVillateAngelaОценок пока нет
- Biomechanical Considerations For PDFДокумент10 страницBiomechanical Considerations For PDFVillateAngelaОценок пока нет
- SedentaryДокумент79 страницSedentaryVillateAngelaОценок пока нет
- Contractura 11 PDFДокумент2 страницыContractura 11 PDFVillateAngelaОценок пока нет
- Solomon Moore2017Документ8 страницSolomon Moore2017VillateAngelaОценок пока нет
- 1 s2.0 S2095254617300650 Main PDFДокумент7 страниц1 s2.0 S2095254617300650 Main PDFVillateAngelaОценок пока нет
- Tendón de Alquiles CirugiaДокумент8 страницTendón de Alquiles CirugiaVillateAngelaОценок пока нет
- Paradoxical Advantage of Middle Aged Sedentary Over Young Sedentary OnДокумент6 страницParadoxical Advantage of Middle Aged Sedentary Over Young Sedentary OnVillateAngelaОценок пока нет
- Geriatric Nursing: Mona Choi, PHD, RN, Sangwoo Ahn, BSN, RN, Dukyoo Jung, PHD, RNДокумент5 страницGeriatric Nursing: Mona Choi, PHD, RN, Sangwoo Ahn, BSN, RN, Dukyoo Jung, PHD, RNVillateAngelaОценок пока нет
- The Impact of High Intensity Interval Training On The CTNT Response To AcuteДокумент25 страницThe Impact of High Intensity Interval Training On The CTNT Response To AcuteVillateAngelaОценок пока нет
- Phisycal Education, School Physical Activity, School Sports and Academic PerformanceДокумент12 страницPhisycal Education, School Physical Activity, School Sports and Academic Performancearjuna_s2100% (3)
- Autoinjerto de La Vaina Del Recto Anterior en WRAP-Aumento de La Ruptura Del Tendón de AquilesSДокумент5 страницAutoinjerto de La Vaina Del Recto Anterior en WRAP-Aumento de La Ruptura Del Tendón de AquilesSVillateAngelaОценок пока нет
- Fernandes2011 Muscle Injury - Physiopathology, DiagnosisДокумент9 страницFernandes2011 Muscle Injury - Physiopathology, DiagnosisFranklin RcrОценок пока нет
- The Effects of Continuous External Compression On Delayed-Onset Muscle Soreness (DOMS)Документ2 страницыThe Effects of Continuous External Compression On Delayed-Onset Muscle Soreness (DOMS)VillateAngelaОценок пока нет
- Biomechanical Considerations ForДокумент10 страницBiomechanical Considerations ForVillateAngelaОценок пока нет
- Ruptura Aguda Del Tendón de Aquiles Cirugía Mínimamente Invasiva Versus Tratamiento No Quirúrgico Con Carga Inmediata de Peso CompletoДокумент6 страницRuptura Aguda Del Tendón de Aquiles Cirugía Mínimamente Invasiva Versus Tratamiento No Quirúrgico Con Carga Inmediata de Peso CompletoVillateAngelaОценок пока нет
- CaracterizaciónДокумент30 страницCaracterizaciónVillateAngelaОценок пока нет
- Manejo de Rupturas Agudas Del Tendón de AquilesДокумент9 страницManejo de Rupturas Agudas Del Tendón de AquilesVillateAngelaОценок пока нет
- Achilles Tendon DisordersДокумент7 страницAchilles Tendon DisordersVillateAngelaОценок пока нет
- Ruptura Aguda Del Tendón de Aquiles Cirugía Mínimamente Invasiva Versus Tratamiento No Quirúrgico Con Carga Inmediata de Peso CompletoДокумент6 страницRuptura Aguda Del Tendón de Aquiles Cirugía Mínimamente Invasiva Versus Tratamiento No Quirúrgico Con Carga Inmediata de Peso CompletoVillateAngelaОценок пока нет
- Evaluación Del Tratamiento Quirúrgico para El Tendón de Aquiles Roto en 31 Atletas. GENIALДокумент8 страницEvaluación Del Tratamiento Quirúrgico para El Tendón de Aquiles Roto en 31 Atletas. GENIALVillateAngelaОценок пока нет
- Unit-3.1.2-Sleeve and Cotter JointДокумент18 страницUnit-3.1.2-Sleeve and Cotter JointAsvath Guru100% (2)
- Business Plan Example - Little LearnerДокумент26 страницBusiness Plan Example - Little LearnerCourtney mcintosh100% (1)
- Anti Stain Nsl30 Super - Msds - SdsДокумент8 страницAnti Stain Nsl30 Super - Msds - SdsS.A. MohsinОценок пока нет
- ASD Diagnosis Tools - UpToDateДокумент3 страницыASD Diagnosis Tools - UpToDateEvy Alvionita Yurna100% (1)
- 2022-Brochure Neonatal PiccДокумент4 страницы2022-Brochure Neonatal PiccNAIYA BHAVSARОценок пока нет
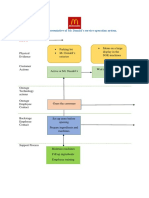
- Blueprint Huynh My Ky Duyen 2022 McDonald'sДокумент2 страницыBlueprint Huynh My Ky Duyen 2022 McDonald'sHuỳnh Mỹ Kỳ DuyênОценок пока нет
- ISO - TR - 15608 - 2017 (En) - Pipe Grouping SystemsДокумент12 страницISO - TR - 15608 - 2017 (En) - Pipe Grouping SystemsTeodor ProdanОценок пока нет
- Sav4747 PDFДокумент49 страницSav4747 PDFAndres Antonio Moreno CastroОценок пока нет
- HUM110 Gilgamesh EssayДокумент4 страницыHUM110 Gilgamesh EssaynsmeganОценок пока нет
- Sample SWMSДокумент4 страницыSample SWMSJuma KavesuОценок пока нет
- Itc LimitedДокумент64 страницыItc Limitedjulee G0% (1)
- Brody2012 PDFДокумент13 страницBrody2012 PDFfrancisca caceresОценок пока нет
- Pengaruh Kualitas Anc Dan Riwayat Morbiditas Maternal Terhadap Morbiditas Maternal Di Kabupaten SidoarjoДокумент9 страницPengaruh Kualitas Anc Dan Riwayat Morbiditas Maternal Terhadap Morbiditas Maternal Di Kabupaten Sidoarjohikmah899Оценок пока нет
- 1A Wound Care AdviceДокумент2 страницы1A Wound Care AdviceGrace ValenciaОценок пока нет
- K EtaДокумент14 страницK EtaJosue Teni BeltetonОценок пока нет
- Reading Practice 6Документ5 страницReading Practice 6Âu DươngОценок пока нет
- Q1. (A) The Diagram Shows A Microphone Being Used To Detect The Output From AДокумент10 страницQ1. (A) The Diagram Shows A Microphone Being Used To Detect The Output From ASivmi MalishaОценок пока нет
- MSDS - Granular Silica GelДокумент3 страницыMSDS - Granular Silica GelLailal HaqimОценок пока нет
- 7-Multiple RegressionДокумент17 страниц7-Multiple Regressionحاتم سلطانОценок пока нет
- DyslexiaДокумент19 страницDyslexiaKeren HapkhОценок пока нет
- 2 Dawn150Документ109 страниц2 Dawn150kirubelОценок пока нет
- J130KДокумент6 страницJ130KBelkisa ŠaćiriОценок пока нет
- BV Lesson Plan 4Документ3 страницыBV Lesson Plan 4api-252119803Оценок пока нет
- E61 DiagramДокумент79 страницE61 Diagramthanes1027Оценок пока нет
- Review - Practical Accounting 1Документ2 страницыReview - Practical Accounting 1Kath LeynesОценок пока нет
- 41403A - Guide - Rev - 12-20-17 - With Edits - 2-16-18Документ167 страниц41403A - Guide - Rev - 12-20-17 - With Edits - 2-16-18Ronald KahoraОценок пока нет
- Parche CRP 65 - Ficha Técnica - en InglesДокумент2 страницыParche CRP 65 - Ficha Técnica - en IngleserwinvillarОценок пока нет
- Carboset CA-600 - CST600 - CO - enДокумент3 страницыCarboset CA-600 - CST600 - CO - enNilsОценок пока нет
- Crime Data Analysis 1Документ2 страницыCrime Data Analysis 1kenny laroseОценок пока нет
- Chapter 2 Unfinished RRLДокумент22 страницыChapter 2 Unfinished RRLGM XylerОценок пока нет