Вам также может понравиться
- Practical Handbook for Small-Gauge Vitrectomy: A Step-By-Step Introduction to Surgical TechniquesОт EverandPractical Handbook for Small-Gauge Vitrectomy: A Step-By-Step Introduction to Surgical TechniquesОценок пока нет
- 2007bg 11Документ6 страниц2007bg 11souq alkanzОценок пока нет
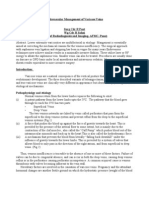
- Radiofrequency Ablation Therapy For Varicose VeinsДокумент7 страницRadiofrequency Ablation Therapy For Varicose VeinsFauziah Nurul LailiОценок пока нет
- Varicose Vein Treatment Tips and Trick - Ablation or GlueДокумент30 страницVaricose Vein Treatment Tips and Trick - Ablation or GlueNata NakamuraОценок пока нет
- 2013 Phlebology EliasДокумент5 страниц2013 Phlebology EliasronnyОценок пока нет
- Lnvaginated Axial Stripping and Stab Avulsion (Hook) Phlebectomy: A Definitive Outpatient Procedure For Primary Varicose VeinsДокумент9 страницLnvaginated Axial Stripping and Stab Avulsion (Hook) Phlebectomy: A Definitive Outpatient Procedure For Primary Varicose VeinsAbrar SabawiОценок пока нет
- Technology Assessment Status Evaluation Endoscopic Band Ligation of VaricesДокумент3 страницыTechnology Assessment Status Evaluation Endoscopic Band Ligation of VaricesElmer PalaciosОценок пока нет
- Endovasc VV MXДокумент9 страницEndovasc VV MXdrrochanОценок пока нет
- EJVES VF Watanabe April 2020Документ4 страницыEJVES VF Watanabe April 2020Francisco Álvarez MarcosОценок пока нет
- Endovenous Laser Treatment of Varicose Veins EVLTДокумент18 страницEndovenous Laser Treatment of Varicose Veins EVLTCTAFDocuments100% (1)
- Aneurysmorrhaphy (Eng)Документ14 страницAneurysmorrhaphy (Eng)Harlan IdrisОценок пока нет
- Ulcera EndovascДокумент4 страницыUlcera EndovascGustavo DolinskyОценок пока нет
- In-Human Robot-Assisted Retinal Vein Cannulation, A World FirstДокумент10 страницIn-Human Robot-Assisted Retinal Vein Cannulation, A World Firstjhorman bulaОценок пока нет
- Varicose Veins of The Lower Extremities Treatment ForДокумент17 страницVaricose Veins of The Lower Extremities Treatment ForsalinasjulioОценок пока нет
- JDattaMegheInstMedSciUniv162235-4959576 134635Документ5 страницJDattaMegheInstMedSciUniv162235-4959576 134635shyampanga2Оценок пока нет
- Quiz ReviewerДокумент6 страницQuiz ReviewerNER CARLO SANTOSОценок пока нет
- Kjtcs043 06 09Документ7 страницKjtcs043 06 09정윤형Оценок пока нет
- Endoscopic Wedge Excisions With CO2 Laser For Subglottic Stenosis, 2020Документ5 страницEndoscopic Wedge Excisions With CO2 Laser For Subglottic Stenosis, 2020Araceli BarreraОценок пока нет
- Varicose Veins Endovenous Laser TreatmentДокумент17 страницVaricose Veins Endovenous Laser TreatmentaillОценок пока нет
- Varicose Vein TreatmentДокумент22 страницыVaricose Vein TreatmentRavi GuptaОценок пока нет
- Cobb - Endoscopic Carpal Tunnel ReleaseДокумент8 страницCobb - Endoscopic Carpal Tunnel ReleaseJohnny WangОценок пока нет
- Prospective Randomized Comparison of External Dacryocystorhinostomy and Endonasal Laser DacryocystorhinostomyДокумент8 страницProspective Randomized Comparison of External Dacryocystorhinostomy and Endonasal Laser DacryocystorhinostomySaaraAlleyahAlAnaziОценок пока нет
- Endoscopic Septoplasty: Indications, Technique, and ResultsДокумент5 страницEndoscopic Septoplasty: Indications, Technique, and ResultsGabriel Vazquez RamosОценок пока нет
- Randomized Clinical Trial of Mechanochemical and Endovenous Thermal Ablation of Great Saphenous Varicose VeinsДокумент7 страницRandomized Clinical Trial of Mechanochemical and Endovenous Thermal Ablation of Great Saphenous Varicose VeinsAmade DeaОценок пока нет
- Jurnal VarisesДокумент4 страницыJurnal VarisesMas AbrarОценок пока нет
- 0068KJR - KJR 12 481Документ6 страниц0068KJR - KJR 12 481Indra dig DrОценок пока нет
- Vascular Access: The Impact of Ultrasonography: Acesso Vascular: o Impacto Da UltrassonografiaДокумент6 страницVascular Access: The Impact of Ultrasonography: Acesso Vascular: o Impacto Da UltrassonografiaLatescu ConstantinОценок пока нет
- Adenoidectomy and Tosillectomy MethodsДокумент5 страницAdenoidectomy and Tosillectomy MethodsBkas GrgОценок пока нет
- Day 4 - APPEC 2021 PDFДокумент397 страницDay 4 - APPEC 2021 PDFGaurieОценок пока нет
- Randomized Foam TrialДокумент10 страницRandomized Foam TrialrachiddellarОценок пока нет
- Lessons Learned After 366 Thermoablated VeinsДокумент5 страницLessons Learned After 366 Thermoablated VeinsAlexandre Campos Moraes AmatoОценок пока нет
- Biolitec Leonardo Multifunction 200 - 2021 - LengkapДокумент13 страницBiolitec Leonardo Multifunction 200 - 2021 - Lengkapdedi KurniawanОценок пока нет
- Gibson Et Al-2012-Transforaminal Endoscopic Spinal SurgeryДокумент7 страницGibson Et Al-2012-Transforaminal Endoscopic Spinal SurgeryjuanguapoОценок пока нет
- Foam SclerotherapyДокумент6 страницFoam SclerotherapyrachiddellarОценок пока нет
- What Are Angioplasty and Vascular Stenting?Документ5 страницWhat Are Angioplasty and Vascular Stenting?mcewenpОценок пока нет
- Iranjradiol 14 03 21742Документ5 страницIranjradiol 14 03 21742AisahОценок пока нет
- Multimodal Tretment of Intracranial Aneurysm: A. Chiriac, I. Poeata, J. Baldauf, H.W. SchroederДокумент10 страницMultimodal Tretment of Intracranial Aneurysm: A. Chiriac, I. Poeata, J. Baldauf, H.W. SchroederApryana Damayanti ARОценок пока нет
- Endoscopic Septoplasty: Nishi GuptaДокумент4 страницыEndoscopic Septoplasty: Nishi GuptaBayuLesmonoОценок пока нет
- Focus: Real-Time Ultrasound-Guided External Ventricular Drain Placement: Technical NoteДокумент5 страницFocus: Real-Time Ultrasound-Guided External Ventricular Drain Placement: Technical NoteOdiet RevenderОценок пока нет
- Minimally İnvasive Surgery-Laparoscopy and Thoracoscopy in Small AnimalsДокумент7 страницMinimally İnvasive Surgery-Laparoscopy and Thoracoscopy in Small Animalstaner_soysuren100% (1)
- Anestesia para Cirugia VitroretinealДокумент6 страницAnestesia para Cirugia Vitroretinealluis castro martinezОценок пока нет
- Magine Methods: Matta M.DДокумент28 страницMagine Methods: Matta M.Dmichal ben meronОценок пока нет
- 23824-Brain AVM With OnyxДокумент6 страниц23824-Brain AVM With OnyxCut FadmalaОценок пока нет
- Management of Brain AVM Procedural Hemorrhagic Complication by The Security'' Catheter TechniqueДокумент5 страницManagement of Brain AVM Procedural Hemorrhagic Complication by The Security'' Catheter TechniquePaulo de TarcioОценок пока нет
- How To Avoid Complications in Endoscopic Skull Base SurgeryДокумент12 страницHow To Avoid Complications in Endoscopic Skull Base SurgeryDr. T. BalasubramanianОценок пока нет
- EVLAДокумент5 страницEVLAGustavo DolinskyОценок пока нет
- Transnasal Endoscopic Neochoanal TechniqueДокумент4 страницыTransnasal Endoscopic Neochoanal TechniqueNalendra Tri WidhianartoОценок пока нет
- Braun Neurology Endoscope SystemДокумент132 страницыBraun Neurology Endoscope SystemMārcis RancānsОценок пока нет
- Applying The WALANT Technique To Surgical Treatment of Distal Radius FracturesДокумент6 страницApplying The WALANT Technique To Surgical Treatment of Distal Radius Fracturesdaniel saucedoОценок пока нет
- Endoscopic Surgery of The OrbitДокумент5 страницEndoscopic Surgery of The OrbitTugce InceОценок пока нет
- Articulo en InglesДокумент4 страницыArticulo en InglesNatalia Gonzalez PerezОценок пока нет
- PCNL Consent FormДокумент4 страницыPCNL Consent FormSaisabelaОценок пока нет
- 701 2022 Article 5445Документ9 страниц701 2022 Article 5445PeyepeyeОценок пока нет
- Radiofrequency Ablation (Liver Tumor)Документ9 страницRadiofrequency Ablation (Liver Tumor)Amna BatoolОценок пока нет
- 297 1289 1 SMДокумент7 страниц297 1289 1 SMRaissaОценок пока нет
- Ophthalmology 8 1079Документ3 страницыOphthalmology 8 1079Raúl Plasencia SaliniОценок пока нет
- Recent Advances in Obstructive JaundiceДокумент38 страницRecent Advances in Obstructive JaundiceCT Natarajan100% (1)
- Endoscopic Versus No-Touch'' Saphenous Vein Harvesting For Coronary Artery Bypass Grafting: A Trade-Off Between Wound Healing and Graft PatencyДокумент13 страницEndoscopic Versus No-Touch'' Saphenous Vein Harvesting For Coronary Artery Bypass Grafting: A Trade-Off Between Wound Healing and Graft PatencyMissing ManОценок пока нет
- Endovenous Microwave Ablation of Great Saphenous VeinДокумент3 страницыEndovenous Microwave Ablation of Great Saphenous VeinMalekseuofi مالك السيوفيОценок пока нет
- Most Important Questions: Breathing & Exchange of Gases Body Fluids & CirculationДокумент209 страницMost Important Questions: Breathing & Exchange of Gases Body Fluids & CirculationLarry JunctionОценок пока нет
- Lecture 12 Cardio Intensive CasesДокумент32 страницыLecture 12 Cardio Intensive Casesraul0% (1)
- 11 The Pericardium and The HeartДокумент39 страниц11 The Pericardium and The HeartJeff D'erique Ozil TettehОценок пока нет
- Lucr - III Part 3Документ130 страницLucr - III Part 3Dan GaidauОценок пока нет
- Vasculitis: (Takayasu's Arteritis & Giant Cell Arteritis)Документ3 страницыVasculitis: (Takayasu's Arteritis & Giant Cell Arteritis)nivraeОценок пока нет
- Pages From Color Atlas of Anatomy - A Photog. Study of The Human Body 7th Ed. - J. Rohen, Et Al., (Lippincott, 2011) WW PDFДокумент1 страницаPages From Color Atlas of Anatomy - A Photog. Study of The Human Body 7th Ed. - J. Rohen, Et Al., (Lippincott, 2011) WW PDFOmer MerzićОценок пока нет
- CVS Examination 3rd MBДокумент30 страницCVS Examination 3rd MBsnowlover boyОценок пока нет
- Cardiovascular SystemДокумент40 страницCardiovascular SystemDouglas Jacques100% (1)
- E351 Full PDFДокумент13 страницE351 Full PDFajes coolОценок пока нет
- Diara Jossiean M. Rogacion: Clinical Clerk 2020-2021 Group 5B Department of MedicineДокумент19 страницDiara Jossiean M. Rogacion: Clinical Clerk 2020-2021 Group 5B Department of MedicineJara RogacionОценок пока нет
- OK - Modul Ortho - Bone Cement Implantation SyndromeДокумент18 страницOK - Modul Ortho - Bone Cement Implantation SyndromeWanditoGayuhUtomoОценок пока нет
- KD Pda DanielДокумент38 страницKD Pda DanielDavid JonathanОценок пока нет
- European Heart Journal Supplements (2019) - SeptemberДокумент82 страницыEuropean Heart Journal Supplements (2019) - SeptemberBeard BeardОценок пока нет
- Pathophysiology of Native Coronary, Vein Graft, and In-Stent Atherosclerosis PDFДокумент20 страницPathophysiology of Native Coronary, Vein Graft, and In-Stent Atherosclerosis PDFJorge Arturo Bustos MartinezОценок пока нет
- Qangioxa 3D Single Vessel Analysis: Introduction ToДокумент31 страницаQangioxa 3D Single Vessel Analysis: Introduction ToJhoni DarjudinОценок пока нет
- Hemodynamics MonitoringДокумент12 страницHemodynamics MonitoringBhawna Joshi100% (3)
- Zero To Finals MedicineДокумент352 страницыZero To Finals MedicinePlay100% (23)
- AortographyДокумент31 страницаAortographyWendy Escalante100% (1)
- Terminalia Arjuna (Arjun Bark) Benefits, Uses, Dosage & Side EffectsДокумент22 страницыTerminalia Arjuna (Arjun Bark) Benefits, Uses, Dosage & Side EffectsManas Arora100% (1)
- Re Ca VAДокумент9 страницRe Ca VAmanudanuОценок пока нет
- Surface Anatomy of The Heart 3Документ2 страницыSurface Anatomy of The Heart 3ammarmashalyОценок пока нет
- Hypertension: Hozan Jaza MSC Clinical Pharmacy College of Pharmacy 10/12/2020Документ81 страницаHypertension: Hozan Jaza MSC Clinical Pharmacy College of Pharmacy 10/12/2020Alan K MhamadОценок пока нет
- Sacubitril Valsartan The Role of NeprilyДокумент11 страницSacubitril Valsartan The Role of NeprilySalvanabilaОценок пока нет
- The Cardiovascular SystemДокумент29 страницThe Cardiovascular SystemTumbali Kein Chester BayleОценок пока нет
- Sample Report Alpha DogДокумент130 страницSample Report Alpha DogUsman DastgirОценок пока нет
- The Popliteal ArteryДокумент11 страницThe Popliteal ArteryKrishnamurthy VenkatachalamОценок пока нет
- The Human Circulatory System: Teacher: D.Bleau School: ST Anthony's Secondary SchoolДокумент10 страницThe Human Circulatory System: Teacher: D.Bleau School: ST Anthony's Secondary SchoolCaiden HenryОценок пока нет
- Cardiovascular Surgery in The Elderly: Salim and LДокумент19 страницCardiovascular Surgery in The Elderly: Salim and LThanh BinhОценок пока нет
- Activity 7 The Cardiovascular SystemДокумент4 страницыActivity 7 The Cardiovascular SystemEllen Mynelle MabulacОценок пока нет
- CardiomyopathiesДокумент9 страницCardiomyopathiesSaurabh BhandariОценок пока нет