Вам также может понравиться
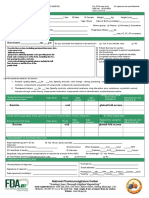
- Adverse Drug Reaction Reporting Form: - Sr. NoДокумент2 страницыAdverse Drug Reaction Reporting Form: - Sr. Nosaadtanvir1256Оценок пока нет
- Adverse Event Report FormДокумент2 страницыAdverse Event Report FormEking InОценок пока нет
- ADR@SAEДокумент23 страницыADR@SAEapi-3810976Оценок пока нет
- Suspected Adverse Reaction FormДокумент2 страницыSuspected Adverse Reaction FormJonathan Deguzman100% (1)
- Adverse Drug Reaction ManagementДокумент5 страницAdverse Drug Reaction ManagementNeha BafanaОценок пока нет
- A. Patient Details: Form NO. ADR-1Документ2 страницыA. Patient Details: Form NO. ADR-1Mkamal MosaОценок пока нет
- Quiz Hospital DocumentationДокумент5 страницQuiz Hospital DocumentationJessica EdiosОценок пока нет
- Mod3 Lectura3 Adverse Event Terminology PDFДокумент17 страницMod3 Lectura3 Adverse Event Terminology PDFMayra ValderramaОценок пока нет
- Inpatient Notes Drafted by N.Yieko: Nicholas Yieko (COMPANY NAME) (Company Address)Документ6 страницInpatient Notes Drafted by N.Yieko: Nicholas Yieko (COMPANY NAME) (Company Address)nicholasОценок пока нет
- Approved ADR FormatДокумент3 страницыApproved ADR Formatinayat.kabirОценок пока нет
- Adverse Drug Reaction FormДокумент3 страницыAdverse Drug Reaction FormHiral PanchalОценок пока нет
- Adverse Drug Reaction FormatДокумент3 страницыAdverse Drug Reaction FormatViky SinghОценок пока нет
- Patient: Age: Hospital No.: Room No.: Impression/Diagnosis: Attending Physician Allergy ToДокумент6 страницPatient: Age: Hospital No.: Room No.: Impression/Diagnosis: Attending Physician Allergy ToClement Nelisher RodriguesОценок пока нет
- Placenta Previa Case Study: Adefuin, Jay Rovillos, Noemie MДокумент40 страницPlacenta Previa Case Study: Adefuin, Jay Rovillos, Noemie MMikes CastroОценок пока нет
- Adverse Eventsd DefinitionsДокумент30 страницAdverse Eventsd Definitionsika sartikaОценок пока нет
- Reporting Suspected Adverse Drug ReactionsДокумент2 страницыReporting Suspected Adverse Drug ReactionsWajeeha HassanОценок пока нет
- Medical history formДокумент1 страницаMedical history formmelyОценок пока нет
- ADR Monitoring and ReportingДокумент13 страницADR Monitoring and ReportingKinjal GamitОценок пока нет
- Pharmacovigilance V01Документ33 страницыPharmacovigilance V01Karveer AghadeОценок пока нет
- Natural History of Disease ProcessДокумент33 страницыNatural History of Disease ProcessalanОценок пока нет
- Investigation FormatДокумент2 страницыInvestigation FormatVinoth PaulОценок пока нет
- Investigation FormatДокумент2 страницыInvestigation FormatVinoth PaulОценок пока нет
- Clinical Condition and Medication Therapy of AmoxiДокумент3 страницыClinical Condition and Medication Therapy of AmoxiRina HerowatiОценок пока нет
- Adverse Drug Reaction FormДокумент3 страницыAdverse Drug Reaction FormHarshОценок пока нет
- Maternity and Child Health Nursing Gynaecology Report (Out Patient)Документ9 страницMaternity and Child Health Nursing Gynaecology Report (Out Patient)Faizah AlshehriОценок пока нет
- Report of Suspected Adverse Reaction To Medicines or VaccinesДокумент2 страницыReport of Suspected Adverse Reaction To Medicines or VaccinesSidhaSaada PatelОценок пока нет
- Activity On Hospital Documentation - HospPharmLab Act 1Документ4 страницыActivity On Hospital Documentation - HospPharmLab Act 1Jan Aerielle AzulОценок пока нет
- My Family's Health RecordДокумент2 страницыMy Family's Health RecordQurat-ul-Ain AzamОценок пока нет
- What To Include in Your Yellow Card of An Adverse Drug ReactionДокумент3 страницыWhat To Include in Your Yellow Card of An Adverse Drug Reactionrhimineecat71Оценок пока нет
- Risk Factors For Cutaneous Adverse Drug ReactionsДокумент26 страницRisk Factors For Cutaneous Adverse Drug ReactionsMukesh Kumar SharmaОценок пока нет
- Dr. Widyati ADR ANALYSIS-PERSIДокумент39 страницDr. Widyati ADR ANALYSIS-PERSIHanaОценок пока нет
- ADR Final1Документ10 страницADR Final1Rubina BisankheОценок пока нет
- Pat 3Документ21 страницаPat 3api-272761526Оценок пока нет
- ICSR FormДокумент1 страницаICSR Formvuki mackoОценок пока нет
- Lecture 5 PharmacovigilanceДокумент32 страницыLecture 5 Pharmacovigilancephoto copyhemnОценок пока нет
- InstructionToFill ADRformДокумент4 страницыInstructionToFill ADRformJahnavi PutrevuОценок пока нет
- ADR FormДокумент2 страницыADR Formapi-3810976Оценок пока нет
- Kuliah 3 - Masalah Berkaitan Dengan Obat - Reg and Inter StudДокумент40 страницKuliah 3 - Masalah Berkaitan Dengan Obat - Reg and Inter StudVerena NatasiaОценок пока нет
- Koringa College of Pharmacy, Dept. of Pharmacy Practice & Pharm D Drug Interaction Documentation FormДокумент1 страницаKoringa College of Pharmacy, Dept. of Pharmacy Practice & Pharm D Drug Interaction Documentation FormHarika PagaОценок пока нет
- Case Investigation Form for AEFIДокумент4 страницыCase Investigation Form for AEFICHICKYОценок пока нет
- Journal Reading Sjs KulitДокумент19 страницJournal Reading Sjs Kulitbella julianaОценок пока нет
- Adverse Drug Reactions: BackgroundДокумент10 страницAdverse Drug Reactions: BackgroundPat YenОценок пока нет
- MTM ToolsДокумент8 страницMTM ToolsEbrahimDawudОценок пока нет
- Diagnosis and Management of ADRsДокумент45 страницDiagnosis and Management of ADRspriyankaОценок пока нет
- Adversedrugreactionmonitoringandreporting Pertemuan 14-15Документ33 страницыAdversedrugreactionmonitoringandreporting Pertemuan 14-15Ani RahayuОценок пока нет
- Patient Database Form, DTPW, PCPДокумент7 страницPatient Database Form, DTPW, PCPClarence100% (1)
- Pediatric HistoryДокумент3 страницыPediatric HistoryMesfin ShifaraОценок пока нет
- Drug (Glucophage)Документ2 страницыDrug (Glucophage)mchaudry7Оценок пока нет
- Pa Tool MihpДокумент23 страницыPa Tool MihpNassif M. BangcolaОценок пока нет
- Flu Consent FormДокумент2 страницыFlu Consent FormTiger Palm TigerОценок пока нет
- RDT 105 – Legal and Ethical Issues in HealthcareДокумент12 страницRDT 105 – Legal and Ethical Issues in HealthcareLoLiTraP KaiОценок пока нет
- Fundamentals PatДокумент20 страницFundamentals Patapi-340247560Оценок пока нет
- PharmacovigilanceДокумент43 страницыPharmacovigilanceTanoy SahaОценок пока нет
- Adverse Eeffects of Drugs and Their Management in PaediatricsДокумент6 страницAdverse Eeffects of Drugs and Their Management in PaediatricsRinchin ChhotenОценок пока нет
- Week 1 CH 1 Intro To PathoДокумент36 страницWeek 1 CH 1 Intro To Pathorami abdiОценок пока нет
- Adverse Eeffects of Drugs and Their Management in PaediatricsДокумент6 страницAdverse Eeffects of Drugs and Their Management in PaediatricsRinchin ChhotenОценок пока нет
- Case FormateДокумент5 страницCase FormateMaido TeОценок пока нет
- Claims Aps Hi MR SurgicalДокумент3 страницыClaims Aps Hi MR SurgicalRudolf CunananОценок пока нет
- Beating the Flu: The Natural Prescription for Surviving Pandemic Influenza and Bird FluОт EverandBeating the Flu: The Natural Prescription for Surviving Pandemic Influenza and Bird FluОценок пока нет
- MORTUARY SERVICESДокумент30 страницMORTUARY SERVICESYogesh ChandraОценок пока нет
- HRALTH ECONOMICSДокумент5 страницHRALTH ECONOMICSYogesh ChandraОценок пока нет
- Barcode Management SystemДокумент17 страницBarcode Management SystemYogesh ChandraОценок пока нет
- M-Health Services: WG CDR DR Yogesh Chandra MBA (HA) Iind Semester Reg No.19P0119023Документ25 страницM-Health Services: WG CDR DR Yogesh Chandra MBA (HA) Iind Semester Reg No.19P0119023Yogesh ChandraОценок пока нет
- HOSPITAL ADMISSION AND DISCHARGEДокумент21 страницаHOSPITAL ADMISSION AND DISCHARGEYogesh ChandraОценок пока нет
- Charitable Hospital PPPДокумент4 страницыCharitable Hospital PPPYogesh ChandraОценок пока нет
- SECURITY SERVICESДокумент13 страницSECURITY SERVICESYogesh ChandraОценок пока нет
- HOUSE KEEPINGДокумент10 страницHOUSE KEEPINGYogesh ChandraОценок пока нет
- Hygiene Sanitation Inspection by SupervisorsДокумент1 страницаHygiene Sanitation Inspection by SupervisorsYogesh ChandraОценок пока нет
- Hospital Waste Management Laws and RealitiesДокумент40 страницHospital Waste Management Laws and RealitiesYogesh ChandraОценок пока нет
- Economic Evaluation in Health CareДокумент18 страницEconomic Evaluation in Health CareYogesh ChandraОценок пока нет
- Inventory Management Issues in Health Care SupplyДокумент34 страницыInventory Management Issues in Health Care SupplyYogesh ChandraОценок пока нет
- SIGNIFICANTДокумент11 страницSIGNIFICANTYogesh ChandraОценок пока нет
- Medication and transfusion errors indicatorsДокумент11 страницMedication and transfusion errors indicatorsYogesh ChandraОценок пока нет
- Emotional Intelligence Effects On JobДокумент94 страницыEmotional Intelligence Effects On JobYogesh Chandra100% (1)
- Hospital Planning Just StartДокумент12 страницHospital Planning Just StartYogesh ChandraОценок пока нет
- Adverse Drug Reaction Reporting Form: - Sr. NoДокумент2 страницыAdverse Drug Reaction Reporting Form: - Sr. NoYogesh ChandraОценок пока нет
- (Kkwalh Ds Nksjku Vknrsa-: Maintain Cough MannersДокумент1 страница(Kkwalh Ds Nksjku Vknrsa-: Maintain Cough MannersYogesh ChandraОценок пока нет
- BMW Rules, 2016 PDFДокумент37 страницBMW Rules, 2016 PDFenvsandyОценок пока нет
- Conflict ManagementДокумент11 страницConflict ManagementYogesh ChandraОценок пока нет
- The Rosemont Behavioral Health Center TurnaroundДокумент20 страницThe Rosemont Behavioral Health Center TurnaroundYogesh ChandraОценок пока нет
- Strategic Management ProcessДокумент2 страницыStrategic Management ProcessYogesh ChandraОценок пока нет