Вам также может понравиться
- Enjoying Pure Wellness: Discovering and Maximizing the Benefits of IV Nutritional and Regenerational TherapyОт EverandEnjoying Pure Wellness: Discovering and Maximizing the Benefits of IV Nutritional and Regenerational TherapyРейтинг: 5 из 5 звезд5/5 (1)
- Complications Associated With Intravenous TherapyДокумент18 страницComplications Associated With Intravenous TherapyIyah Jane Villahermosa50% (2)
- The Nurse Practitioner in UrologyОт EverandThe Nurse Practitioner in UrologyMichelle LajinessОценок пока нет
- Ways of Knowing in A Clinical CaseДокумент8 страницWays of Knowing in A Clinical CaseAntonioОценок пока нет
- The Empowered Patient: Navigating the Healthcare System with ConfidenceОт EverandThe Empowered Patient: Navigating the Healthcare System with ConfidenceОценок пока нет
- Understand Congestive Heart FailureДокумент5 страницUnderstand Congestive Heart FailureOanh HoangОценок пока нет
- The Role of Dialysis Nurse On Nutritional Therapy of DialysisДокумент6 страницThe Role of Dialysis Nurse On Nutritional Therapy of DialysisAryoОценок пока нет
- Fundamentals of Nursing Lecture Notes PDF - CompressДокумент43 страницыFundamentals of Nursing Lecture Notes PDF - CompressFelyn DavideОценок пока нет
- 151 Nursing DocumentationДокумент24 страницы151 Nursing DocumentationNasrullah UllahОценок пока нет
- IV TherapyДокумент5 страницIV TherapyThunderОценок пока нет
- Case 36 AscitesДокумент4 страницыCase 36 AscitesMichaelОценок пока нет
- Fluids Electrolytes and Acid Base ImbalancesДокумент8 страницFluids Electrolytes and Acid Base ImbalancesSamantha Bernardo UndaОценок пока нет
- 09 Pearls On How To Start IV TherapyДокумент53 страницы09 Pearls On How To Start IV TherapyЩербакова Лена100% (2)
- Post Op Assessment SurgeryДокумент20 страницPost Op Assessment SurgeryAbdullah MatarОценок пока нет
- ETOH Case StudyДокумент5 страницETOH Case StudyCharme Jean RaygonОценок пока нет
- Alcohol WithdrawalДокумент39 страницAlcohol WithdrawalRellie CastroОценок пока нет
- Diabetics Self Management PDFДокумент56 страницDiabetics Self Management PDFwsergio0072Оценок пока нет
- Purposes of Intravenous (IV) TherapyДокумент13 страницPurposes of Intravenous (IV) TherapyPrincess Villasis BaciaОценок пока нет
- Lecture On Metabolic DisordersДокумент56 страницLecture On Metabolic DisordersRoselily Flores CoquillaОценок пока нет
- Qi Project PaperДокумент8 страницQi Project Paperapi-380333919Оценок пока нет
- Anticancer Drugs PharmacologyДокумент19 страницAnticancer Drugs PharmacologyZainОценок пока нет
- Wosaam Board CertificationДокумент4 страницыWosaam Board CertificationLydia KirbyОценок пока нет
- Table Vitamins PDFДокумент3 страницыTable Vitamins PDFthomasqilОценок пока нет
- IV TherapyДокумент34 страницыIV Therapyfairwoods100% (2)
- Vollererhof Spa Hotel PamphletДокумент24 страницыVollererhof Spa Hotel PamphletAustrian National Tourism Board100% (25)
- Psychiatric Registered Nurse.Документ4 страницыPsychiatric Registered Nurse.api-121447848Оценок пока нет
- UTIДокумент46 страницUTIAssad MohammadОценок пока нет
- Basic Principles of Wound ManagementДокумент14 страницBasic Principles of Wound ManagementLuis RuizОценок пока нет
- EbpДокумент21 страницаEbpapi-356303021Оценок пока нет
- 10 1097@01 JAA 0000522145 52305 AaДокумент2 страницы10 1097@01 JAA 0000522145 52305 AaAwal Safar M100% (1)
- Perioperative NursingДокумент24 страницыPerioperative Nursingann aquino100% (1)
- Intravenous Therapy: By: Jahzeel B. Acab Enzo Miguel BandoquilloДокумент46 страницIntravenous Therapy: By: Jahzeel B. Acab Enzo Miguel BandoquilloJah AcabОценок пока нет
- Intravenous TherapyДокумент10 страницIntravenous TherapyS. AmberОценок пока нет
- NUR 420 Practicum Final Practicum Progress DocumentДокумент7 страницNUR 420 Practicum Final Practicum Progress DocumentBrooke GagnonОценок пока нет
- Generic Name Captopril Brand NamesДокумент18 страницGeneric Name Captopril Brand NamesAiko Villacortes100% (1)
- Cancer Alternative Therapy HumaДокумент9 страницCancer Alternative Therapy HumaHariHaranОценок пока нет
- IV Therapy CompleteДокумент66 страницIV Therapy CompleteSittie Tasneemu M J100% (1)
- Hypertension FactsheetДокумент2 страницыHypertension FactsheetPedro QuintasОценок пока нет
- Guidelines For The Management of Alcohol Dependendence and Acute Withdrawal On General Psychiatry Wards May 2017Документ10 страницGuidelines For The Management of Alcohol Dependendence and Acute Withdrawal On General Psychiatry Wards May 2017renzo85rhОценок пока нет
- How To Appy Holistic Care Talk 24Документ22 страницыHow To Appy Holistic Care Talk 24Syifa FatiyaОценок пока нет
- 3112 MultisystemcasestudyДокумент9 страниц3112 Multisystemcasestudyapi-306118308Оценок пока нет
- Group Research PaperДокумент16 страницGroup Research Paperapi-403093734Оценок пока нет
- Scholarly Capstone PaperДокумент5 страницScholarly Capstone Paperapi-455567458Оценок пока нет
- IV Infusion SolutionДокумент8 страницIV Infusion SolutionmohammedОценок пока нет
- Hemodialysis: By: Liana Lee SenciónДокумент14 страницHemodialysis: By: Liana Lee SenciónKavidu KeshanОценок пока нет
- Definition of Infiltration Phlebitis and ExtravasationДокумент2 страницыDefinition of Infiltration Phlebitis and ExtravasationJessie YingОценок пока нет
- Urinary IncontinenceДокумент12 страницUrinary IncontinenceAmrit Preet KaurОценок пока нет
- Clinical Procedures For Safer Patient Care: Chapter 8. Intravenous TherapyДокумент54 страницыClinical Procedures For Safer Patient Care: Chapter 8. Intravenous TherapyGladys YaresОценок пока нет
- Diet, Exercise, Metabolic SyndromeДокумент9 страницDiet, Exercise, Metabolic SyndromeJason WongОценок пока нет
- WOCN ScopeStandards Pgs 13-1 PDFДокумент2 страницыWOCN ScopeStandards Pgs 13-1 PDFAsep ArdiОценок пока нет
- Radical Cystectomy: History of The ProcedureДокумент6 страницRadical Cystectomy: History of The ProcedureIvy MinaОценок пока нет
- Contemporary ImageДокумент43 страницыContemporary ImageProf. L100% (1)
- Hemodialysis: NURSING DIAGNOSIS: Injury, Risk For (Loss of Vascular Access) Risk Factors May IncludeДокумент10 страницHemodialysis: NURSING DIAGNOSIS: Injury, Risk For (Loss of Vascular Access) Risk Factors May IncludeChevelle Valenciano-GaanОценок пока нет
- Nursing Orientation Program Intravenous TherapyДокумент45 страницNursing Orientation Program Intravenous TherapyMarianne LayloОценок пока нет
- Heparin Drip - PortfolioДокумент20 страницHeparin Drip - Portfolioapi-306657745100% (1)
- SBARДокумент1 страницаSBARBenОценок пока нет
- Case Study HemodialysisДокумент5 страницCase Study HemodialysisCharmaine del RosarioОценок пока нет
- Seizures in Children JULIO 2020Документ29 страницSeizures in Children JULIO 2020Elizabeth HendersonОценок пока нет
- Mds 3Документ3 страницыMds 3api-434982019Оценок пока нет
- 03kathopanishad SriДокумент22 страницы03kathopanishad SriSuresh IndiaОценок пока нет
- Shatyayaniyopanishad - SriДокумент1 страницаShatyayaniyopanishad - SriSuresh IndiaОценок пока нет
- Dattatreyopanishad SriДокумент1 страницаDattatreyopanishad SriSuresh IndiaОценок пока нет
- 02 Dattatreyopanishad SriДокумент1 страница02 Dattatreyopanishad SriSuresh IndiaОценок пока нет
- Vidyaatma - SriДокумент11 страницVidyaatma - SriSuresh IndiaОценок пока нет
- 102 Gaarudopanishad 2Документ1 страница102 Gaarudopanishad 2Suresh IndiaОценок пока нет
- Atarva VedaДокумент515 страницAtarva VedacharankotagiriОценок пока нет
- Sri Sathya Sai Books and Publications Trust, Prasanthi NilayamДокумент2 страницыSri Sathya Sai Books and Publications Trust, Prasanthi NilayamSuresh IndiaОценок пока нет
- BhajaGovindam - ChalapathiraoДокумент8 страницBhajaGovindam - ChalapathiraoSuresh IndiaОценок пока нет
- WHO Report - April 23Документ12 страницWHO Report - April 23CityNewsTorontoОценок пока нет
- Introduction To The WorldДокумент12 страницIntroduction To The WorldAnglophile123Оценок пока нет
- The Story of Deliverance of Jagai-Madhai - Hari Bol The Path To VaikunthaДокумент4 страницыThe Story of Deliverance of Jagai-Madhai - Hari Bol The Path To VaikunthaSuresh IndiaОценок пока нет
- Species Concept - MalletДокумент15 страницSpecies Concept - MalletBoomdayОценок пока нет
- Essence of Maha NarayanopanishadДокумент81 страницаEssence of Maha NarayanopanishadPrabhasini PОценок пока нет
- Can We Place An Idol of The Goddess Laxmiji in A Home Temple - What Are The Rules For Keeping A Laxmiji Idol - Quora PDFДокумент1 страницаCan We Place An Idol of The Goddess Laxmiji in A Home Temple - What Are The Rules For Keeping A Laxmiji Idol - Quora PDFSuresh IndiaОценок пока нет
- Sandhya A Vandana MДокумент117 страницSandhya A Vandana Mpradeepauradkar100% (1)
- 01 Summary of All TextsДокумент203 страницы01 Summary of All TextssrivatsaОценок пока нет
- Spiritual Diary Template - Swami SivanandaДокумент1 страницаSpiritual Diary Template - Swami SivanandausasivaОценок пока нет
- Meditation On Om PDFДокумент124 страницыMeditation On Om PDFIshan KumarОценок пока нет
- Chanting Rules - GRD IYERS PDFДокумент9 страницChanting Rules - GRD IYERS PDFSuresh IndiaОценок пока нет
- User Guide Nokia 105 User GuideДокумент36 страницUser Guide Nokia 105 User GuideSuresh IndiaОценок пока нет
- Super Science of GayatriДокумент177 страницSuper Science of Gayatrisksuman100% (36)
- Digest 420 - Marriage Questions - HH Romapada SwamiДокумент3 страницыDigest 420 - Marriage Questions - HH Romapada SwamiSuresh IndiaОценок пока нет
- Sandhyavandanam PDFДокумент26 страницSandhyavandanam PDFmaggi14Оценок пока нет
- A-Derma Epitheliale AH Duo 40ml - Amazon - in - Beauty PDFДокумент1 страницаA-Derma Epitheliale AH Duo 40ml - Amazon - in - Beauty PDFSuresh IndiaОценок пока нет
- Essentials of Hindu Dharma Part OneДокумент4 страницыEssentials of Hindu Dharma Part Onemishra012Оценок пока нет
- Practical Meditation Spiritual Yoga For The Mind Jayanti B.K.Документ113 страницPractical Meditation Spiritual Yoga For The Mind Jayanti B.K.Suresh India100% (1)
- Who Rights Roles Respon HW Covid 19Документ3 страницыWho Rights Roles Respon HW Covid 19HarryОценок пока нет
- Philosophy - Maya Panchakam PDFДокумент3 страницыPhilosophy - Maya Panchakam PDFSuresh IndiaОценок пока нет
- Reducing Toxin ChemicalsДокумент8 страницReducing Toxin ChemicalsSuresh IndiaОценок пока нет
- AV Y TẾ 2Документ27 страницAV Y TẾ 2Đạt Bùi TiếnОценок пока нет
- Health: Quarter 1, Wk. 2 - Module 2Документ45 страницHealth: Quarter 1, Wk. 2 - Module 2Joy CamОценок пока нет
- LG Residential EN PDFДокумент27 страницLG Residential EN PDFray2001Оценок пока нет
- Daftar Pustaka YyyahahajshДокумент7 страницDaftar Pustaka YyyahahajshDiki NugrahaОценок пока нет
- COPDДокумент59 страницCOPDKarenmedicalОценок пока нет
- DMAS Low Acuity Non Emergent ER Diagnosis Code ListДокумент17 страницDMAS Low Acuity Non Emergent ER Diagnosis Code ListLia TabackmanОценок пока нет
- Amaroli 15 YicДокумент25 страницAmaroli 15 Yicparvesh sangwanОценок пока нет
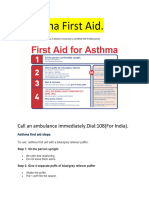
- Asthama First Aid.Документ3 страницыAsthama First Aid.Manoj KumarОценок пока нет
- The Health Benefits of Nose BreathingДокумент4 страницыThe Health Benefits of Nose BreathinganeuОценок пока нет
- NP3Документ12 страницNP3rexinne noahОценок пока нет
- Case StudyДокумент35 страницCase StudysamanОценок пока нет
- Wheezing, Bronchiolitis, and BronchitisДокумент12 страницWheezing, Bronchiolitis, and BronchitisMuhd AzamОценок пока нет
- Paediatric AsthmaДокумент246 страницPaediatric AsthmaOxana TurcuОценок пока нет
- GRAMMAR Health Problems VocabularyДокумент6 страницGRAMMAR Health Problems VocabularyRichard Rivas100% (1)
- Case Study On Bronchial AsthmaДокумент29 страницCase Study On Bronchial Asthmamanny valenciaОценок пока нет
- Housing and Health: Time Again For Public Health ActionДокумент29 страницHousing and Health: Time Again For Public Health ActionLaura ZahariaОценок пока нет
- Physiological Basis of Respiratory Disease (Qutayba Hamid, Joanne Shannon MD, James Martin)Документ816 страницPhysiological Basis of Respiratory Disease (Qutayba Hamid, Joanne Shannon MD, James Martin)RLibdehОценок пока нет
- Salmeterol XinafoateДокумент2 страницыSalmeterol XinafoateKanicio MedelОценок пока нет
- Pedia 102 Quiz 2 SemifinalsДокумент11 страницPedia 102 Quiz 2 Semifinalsquidditch07Оценок пока нет
- Med Surg Respiration-Cardiac NotesДокумент11 страницMed Surg Respiration-Cardiac Notesorganictallgirl50% (2)
- Black Seed (Nigella Sativa) - Clark's NutritionДокумент5 страницBlack Seed (Nigella Sativa) - Clark's NutritionZoran BlamОценок пока нет
- How Food WorksДокумент19 страницHow Food WorksnafeesОценок пока нет
- Dental Treatment of Medical Compromised PatientsДокумент50 страницDental Treatment of Medical Compromised PatientssrinivasОценок пока нет
- Effectiveness of Nebulised Salbutamol Administered in Ambulances To Patients With Severe Acute AsthmaДокумент4 страницыEffectiveness of Nebulised Salbutamol Administered in Ambulances To Patients With Severe Acute AsthmaMaria ClaraОценок пока нет
- Pediatricstatusasthmaticus: Christopher L. Carroll,, Kathleen A. SalaДокумент14 страницPediatricstatusasthmaticus: Christopher L. Carroll,, Kathleen A. SalaAndreea SasuОценок пока нет
- Welcome Homeopathy - Dr. S. C. MadanДокумент195 страницWelcome Homeopathy - Dr. S. C. Madanreza100% (4)
- Saba Hanif Presentation...Документ19 страницSaba Hanif Presentation...Saba KhanОценок пока нет
- Religiosity On VicesДокумент17 страницReligiosity On VicesJohn Philip ParasОценок пока нет
- Nutrition and Respiratory Diseases PDFДокумент53 страницыNutrition and Respiratory Diseases PDFliggiedy100% (1)
- Chronopharmacology and Its Implication To Drug TherapyДокумент22 страницыChronopharmacology and Its Implication To Drug TherapyLogical SolutionsОценок пока нет
- Organic Chemistry for Schools: Advanced Level and Senior High SchoolОт EverandOrganic Chemistry for Schools: Advanced Level and Senior High SchoolОценок пока нет
- Periodic Tales: A Cultural History of the Elements, from Arsenic to ZincОт EverandPeriodic Tales: A Cultural History of the Elements, from Arsenic to ZincРейтинг: 3.5 из 5 звезд3.5/5 (137)
- The Disappearing Spoon: And Other True Tales of Madness, Love, and the History of the World from the Periodic Table of the ElementsОт EverandThe Disappearing Spoon: And Other True Tales of Madness, Love, and the History of the World from the Periodic Table of the ElementsРейтинг: 4 из 5 звезд4/5 (146)
- Is That a Fact?: Frauds, Quacks, and the Real Science of Everyday LifeОт EverandIs That a Fact?: Frauds, Quacks, and the Real Science of Everyday LifeРейтинг: 5 из 5 звезд5/5 (4)
- Monkeys, Myths, and Molecules: Separating Fact from Fiction, and the Science of Everyday LifeОт EverandMonkeys, Myths, and Molecules: Separating Fact from Fiction, and the Science of Everyday LifeРейтинг: 4 из 5 звезд4/5 (1)
- The Regenerative Grower's Guide to Garden Amendments: Using Locally Sourced Materials to Make Mineral and Biological Extracts and FermentsОт EverandThe Regenerative Grower's Guide to Garden Amendments: Using Locally Sourced Materials to Make Mineral and Biological Extracts and FermentsРейтинг: 5 из 5 звезд5/5 (3)
- The Elements We Live By: How Iron Helps Us Breathe, Potassium Lets Us See, and Other Surprising Superpowers of the Periodic TableОт EverandThe Elements We Live By: How Iron Helps Us Breathe, Potassium Lets Us See, and Other Surprising Superpowers of the Periodic TableРейтинг: 3.5 из 5 звезд3.5/5 (22)
- The Periodic Table: A Very Short IntroductionОт EverandThe Periodic Table: A Very Short IntroductionРейтинг: 4.5 из 5 звезд4.5/5 (3)
- The Nature of Drugs Vol. 1: History, Pharmacology, and Social ImpactОт EverandThe Nature of Drugs Vol. 1: History, Pharmacology, and Social ImpactРейтинг: 5 из 5 звезд5/5 (5)
- Chemistry for Breakfast: The Amazing Science of Everyday LifeОт EverandChemistry for Breakfast: The Amazing Science of Everyday LifeРейтинг: 4.5 из 5 звезд4.5/5 (90)
- Handbook of Formulating Dermal Applications: A Definitive Practical GuideОт EverandHandbook of Formulating Dermal Applications: A Definitive Practical GuideОценок пока нет
- A Perfect Red: Empire, Espionage, and the Quest for the Color of DesireОт EverandA Perfect Red: Empire, Espionage, and the Quest for the Color of DesireРейтинг: 4 из 5 звезд4/5 (129)
- Essential Oil Chemistry Formulating Essential Oil Blends that Heal - Aldehyde - Ketone - Lactone: Healing with Essential OilОт EverandEssential Oil Chemistry Formulating Essential Oil Blends that Heal - Aldehyde - Ketone - Lactone: Healing with Essential OilРейтинг: 5 из 5 звезд5/5 (1)
- Chemistry: a QuickStudy Laminated Reference GuideОт EverandChemistry: a QuickStudy Laminated Reference GuideРейтинг: 5 из 5 звезд5/5 (1)
- Formulating, Packaging, and Marketing of Natural Cosmetic ProductsОт EverandFormulating, Packaging, and Marketing of Natural Cosmetic ProductsОценок пока нет
- Guidelines for Integrating Process Safety into Engineering ProjectsОт EverandGuidelines for Integrating Process Safety into Engineering ProjectsОценок пока нет
- The Periodic Table of Elements - Alkali Metals, Alkaline Earth Metals and Transition Metals | Children's Chemistry BookОт EverandThe Periodic Table of Elements - Alkali Metals, Alkaline Earth Metals and Transition Metals | Children's Chemistry BookОценок пока нет
- The Periodic Table of Elements - Post-Transition Metals, Metalloids and Nonmetals | Children's Chemistry BookОт EverandThe Periodic Table of Elements - Post-Transition Metals, Metalloids and Nonmetals | Children's Chemistry BookОценок пока нет