Вам также может понравиться
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (345)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
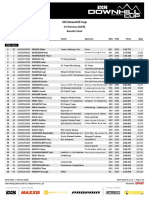
- Results Finals DHC #4 Ilmenau 2023Документ12 страницResults Finals DHC #4 Ilmenau 2023racementОценок пока нет
- YAC Product Positioning Brand StrategyДокумент143 страницыYAC Product Positioning Brand StrategyJosephine RoperОценок пока нет
- ISE II - Phrasal Verbs - Public Figures - RДокумент2 страницыISE II - Phrasal Verbs - Public Figures - RMarianicoElCortoОценок пока нет
- HW Berkser EnglishДокумент2 страницыHW Berkser EnglishNanis Loves RikiОценок пока нет
- Price Tag LyricsДокумент8 страницPrice Tag LyricsUmi Dhilla IsmaОценок пока нет
- Partbook pc130f 7Документ328 страницPartbook pc130f 7Jupray100% (10)
- Grade 4 Unit 11 Practice TestДокумент4 страницыGrade 4 Unit 11 Practice TestYến Nguyễn KimОценок пока нет
- The Fashion Revolution Brought by Audrey HepburnДокумент10 страницThe Fashion Revolution Brought by Audrey HepburnvarunОценок пока нет
- Body Alchemy: The Shredded AcademyДокумент6 страницBody Alchemy: The Shredded AcademyMATHEWS MATHEWSОценок пока нет
- Syh 1552 PDFДокумент1 страницаSyh 1552 PDFSella Pegaso PegasoОценок пока нет
- Football DrillsДокумент25 страницFootball DrillsSha F100% (1)
- Chapter 01 (Intro)Документ14 страницChapter 01 (Intro)Hajim Amir SallehОценок пока нет
- DIB Vs DBB PDFДокумент1 страницаDIB Vs DBB PDFAdhitya DarmadiОценок пока нет
- % %× VCT) PM : F (NewtonДокумент7 страниц% %× VCT) PM : F (NewtonJayОценок пока нет
- Automobile Engineering - Lecture Notes, Study Material and Important Questions, AnswersДокумент5 страницAutomobile Engineering - Lecture Notes, Study Material and Important Questions, AnswersM.V. TVОценок пока нет
- Design Concepts For The Proposed New Cavan Monaghan Community CentreДокумент23 страницыDesign Concepts For The Proposed New Cavan Monaghan Community CentrePeterborough ExaminerОценок пока нет
- Sports Magazine FF2Документ124 страницыSports Magazine FF2Ayaz Ahmed KhanОценок пока нет
- Pekanbaru Film Equipment RentalДокумент1 страницаPekanbaru Film Equipment RentalAhmad Alfaruqi nasutionОценок пока нет
- Recess Games Rotations LPДокумент3 страницыRecess Games Rotations LPapi-507051575Оценок пока нет
- 200 XC USA 2008: Spare Parts Manual: ChassisДокумент32 страницы200 XC USA 2008: Spare Parts Manual: ChassischarlesОценок пока нет
- CZ 75 Kadet: Instruction ManualДокумент0 страницCZ 75 Kadet: Instruction Manualab212amisarОценок пока нет
- Wing Chun TestingДокумент9 страницWing Chun TestingIan100% (1)
- Mini Six Character SheetДокумент1 страницаMini Six Character SheetJoaquin AlonsoОценок пока нет
- English Class. Introductions. 1. Read Below and Complete With The Information of The Angry BirdДокумент6 страницEnglish Class. Introductions. 1. Read Below and Complete With The Information of The Angry BirdСветлана ЗадорожняяОценок пока нет
- Popular MechanicsДокумент132 страницыPopular MechanicsRaviChandra100% (7)
- Last Christmas - MelodiДокумент2 страницыLast Christmas - MelodiAdamОценок пока нет
- Channel LineupДокумент1 страницаChannel LineupBorana LaciОценок пока нет
- Kyokushin Beginners GuideДокумент45 страницKyokushin Beginners GuideKamal TabatabaeeОценок пока нет
- Mansions of Madness Second Editon Rules ReferenceДокумент24 страницыMansions of Madness Second Editon Rules ReferenceGeorge AlexandrisОценок пока нет
- Elan Skis Racing Catalogue 1314 PDFДокумент7 страницElan Skis Racing Catalogue 1314 PDFwest werbeagenturОценок пока нет