Вам также может понравиться
- Current Techniques in Canine and Feline NeurosurgeryОт EverandCurrent Techniques in Canine and Feline NeurosurgeryAndy ShoresОценок пока нет
- Shoulder Muscle Forces and Tendon Excursions During Glenohumeral Abduction in The Scapular Plane - McMahon Et Al. 1995Документ10 страницShoulder Muscle Forces and Tendon Excursions During Glenohumeral Abduction in The Scapular Plane - McMahon Et Al. 1995Frangolho JoãoОценок пока нет
- 2021 Influence of invertor and evertor muscle fatigue on functional jump tests andДокумент4 страницы2021 Influence of invertor and evertor muscle fatigue on functional jump tests andktan.lboroОценок пока нет
- Tullberg-Manip Not Alter Sij Spine98Документ8 страницTullberg-Manip Not Alter Sij Spine98Swapna HarnishОценок пока нет
- Standard Reference Values For Musculoskeletal - Schmidt Schicke Gromnica-IhleДокумент7 страницStandard Reference Values For Musculoskeletal - Schmidt Schicke Gromnica-IhleFer Hijar FraustoОценок пока нет
- Indirect Ultrasound Measurement of Humeral Torsion in Adolescent Baseball Players and Non-Athletic AdultsДокумент9 страницIndirect Ultrasound Measurement of Humeral Torsion in Adolescent Baseball Players and Non-Athletic Adults杨钦杰Оценок пока нет
- Lower Limb Spasticity Assessment Using An Inertial Sensor: A Reliability StudyДокумент13 страницLower Limb Spasticity Assessment Using An Inertial Sensor: A Reliability StudyGeangu Costin AlexОценок пока нет
- Sagittal Spine Posture Assessment: Feasibility of A Protocol Based On Intersegmental MomentsДокумент5 страницSagittal Spine Posture Assessment: Feasibility of A Protocol Based On Intersegmental MomentsVizaОценок пока нет
- Sonography of Shoulder Impingement SyndromeДокумент5 страницSonography of Shoulder Impingement Syndromeapi-263772125Оценок пока нет
- Journal of BiomechanicsДокумент10 страницJournal of BiomechanicsjothiОценок пока нет
- Karduna2005 PDFДокумент7 страницKarduna2005 PDFAlexandraОценок пока нет
- oberДокумент5 страницoberAndrey LingОценок пока нет
- Art 3A10.1007 2Fs00540 012 1429 ZДокумент4 страницыArt 3A10.1007 2Fs00540 012 1429 ZRusman Hadi RachmanОценок пока нет
- Revision of The Shoulder Normalization Tests Is Required To Include Rhomboid Major and Teres MajorДокумент4 страницыRevision of The Shoulder Normalization Tests Is Required To Include Rhomboid Major and Teres MajorTulkas el fuerteОценок пока нет
- Muscle Activation Pattern of Hip Arthroplasty Patients in WalkingДокумент9 страницMuscle Activation Pattern of Hip Arthroplasty Patients in Walkingsebas valadezОценок пока нет
- Influence of High-Heeled Shoes On The Sagittal Balance of The Spine and The Whole Body 2016 PDFДокумент8 страницInfluence of High-Heeled Shoes On The Sagittal Balance of The Spine and The Whole Body 2016 PDFJuan Carlos LescanoОценок пока нет
- 3 Chiropractic Subluxation IndicatorsДокумент46 страниц3 Chiropractic Subluxation IndicatorsMário Ornelas100% (3)
- Measurement of Coracohumeral Distance in 3 Shoulder Positions Using Dynamic Ultrasonography: Correlation With Subscapularis TearДокумент7 страницMeasurement of Coracohumeral Distance in 3 Shoulder Positions Using Dynamic Ultrasonography: Correlation With Subscapularis TearIvone Cruzado UrcoОценок пока нет
- Aob 21 208Документ5 страницAob 21 208MmdОценок пока нет
- Primary Total Shoulder Arthroplasty Performed Entirely Thru The Rotator Interval - Technique and Minimum Two-Year OutcomesДокумент10 страницPrimary Total Shoulder Arthroplasty Performed Entirely Thru The Rotator Interval - Technique and Minimum Two-Year OutcomesmotohumeresОценок пока нет
- 2011 Test de Flexión Con RotaciónДокумент5 страниц2011 Test de Flexión Con RotaciónPablo Cuevas SaldivarОценок пока нет
- Measurement of Subacromial Impingement of The Rotator CuffДокумент6 страницMeasurement of Subacromial Impingement of The Rotator Cufffelci.oscarОценок пока нет
- Artigo Médico UltrassonografistaДокумент4 страницыArtigo Médico UltrassonografistaGeraldo MoraesОценок пока нет
- propiocepcion hombro post cirugiaДокумент6 страницpropiocepcion hombro post cirugiamarcelogascon.oОценок пока нет
- Additional Abstracts: The Bear-Hug Test: A New and Sensitive Test For Diagnosing A Subscapularis TearДокумент9 страницAdditional Abstracts: The Bear-Hug Test: A New and Sensitive Test For Diagnosing A Subscapularis Tearo7113Оценок пока нет
- tmp5092 TMPДокумент8 страницtmp5092 TMPFrontiersОценок пока нет
- Accepted ManuscriptДокумент40 страницAccepted ManuscriptDaniel CarcamoОценок пока нет
- Cavallo - CAPESB 2021Документ2 страницыCavallo - CAPESB 2021tanvir anwarОценок пока нет
- Tutore Post-Op Immobilization Optimal Shoulder Immobilization Postures Following Surgical Repair of Rotator Cuff Tears A Simulation AnalysisДокумент8 страницTutore Post-Op Immobilization Optimal Shoulder Immobilization Postures Following Surgical Repair of Rotator Cuff Tears A Simulation AnalysisAndreaHistoryXОценок пока нет
- December2006RRHardwickДокумент8 страницDecember2006RRHardwickHaile Mariam González GarcíaОценок пока нет
- F.Luciano C.Zilianti L.Perini A.Guzzardella G.Pavei Get Rights and ContentДокумент68 страницF.Luciano C.Zilianti L.Perini A.Guzzardella G.Pavei Get Rights and ContentgvozdenОценок пока нет
- Peroneal Reaction Times and Eversion Motor Response in Healthy and Unstable AnklesДокумент6 страницPeroneal Reaction Times and Eversion Motor Response in Healthy and Unstable AnklesPatricia BortolottiОценок пока нет
- Effect of Hip and Knee Joint Angles On Resting HamДокумент10 страницEffect of Hip and Knee Joint Angles On Resting HamMaria Clara BrandãoОценок пока нет
- Revisit To Scapular Dyskinesis - Three-Dimensional Wing Computed Tomography in Prone PositionДокумент8 страницRevisit To Scapular Dyskinesis - Three-Dimensional Wing Computed Tomography in Prone PositionDaniel CarcamoОценок пока нет
- Nyffeler - Effects of Glenoid Compont Version On Humeral Head Displacement and Joint Reaction ForcesДокумент5 страницNyffeler - Effects of Glenoid Compont Version On Humeral Head Displacement and Joint Reaction ForcesRaphael BazanОценок пока нет
- 2015 Schmitz FOCUSED AND RADIAL Shockwave For Musculoskeletal, More SmilaritiesДокумент2 страницы2015 Schmitz FOCUSED AND RADIAL Shockwave For Musculoskeletal, More SmilaritieskangmasОценок пока нет
- Differences in Muscle Shoulder External Rotation in Open Kinetic Chain and Closed Kinetic Chain Exercises PDFДокумент3 страницыDifferences in Muscle Shoulder External Rotation in Open Kinetic Chain and Closed Kinetic Chain Exercises PDFLeonardiniОценок пока нет
- Cat 2Документ5 страницCat 2Edgardo BivimasОценок пока нет
- Pelet 2006 Bankart repair for recurrent anterior glenohumeral instability- Results at twenty-nine years’ follow-upДокумент5 страницPelet 2006 Bankart repair for recurrent anterior glenohumeral instability- Results at twenty-nine years’ follow-uptheorthopaedistОценок пока нет
- Roussouly-Classification of The Normal Variation in The Sagittal Alignment of The Human Lumbar SpineДокумент8 страницRoussouly-Classification of The Normal Variation in The Sagittal Alignment of The Human Lumbar Spinedr.s.russo5172Оценок пока нет
- X-Ray: Correlation Study Between Cervical X-Ray Sagittal Parameters and Chuna Posture Analysis ResultsДокумент13 страницX-Ray: Correlation Study Between Cervical X-Ray Sagittal Parameters and Chuna Posture Analysis Resultskang soon cheolОценок пока нет
- Kam 2018Документ11 страницKam 2018JT DanielsОценок пока нет
- Alyas Upright MRI LXДокумент14 страницAlyas Upright MRI LXLuca PellaОценок пока нет
- Strain and Excursion of The Sciatic, Tibial, and Plantar Nerves During A Modified Straight Leg Raising TestДокумент7 страницStrain and Excursion of The Sciatic, Tibial, and Plantar Nerves During A Modified Straight Leg Raising TestPantelis BaltzisОценок пока нет
- Movimiento Del Escafoides Con Aparato de Yeso. 2017Документ7 страницMovimiento Del Escafoides Con Aparato de Yeso. 2017brakanataОценок пока нет
- High Tibial Osteotomy For Osteoarthritis of The KneeДокумент6 страницHigh Tibial Osteotomy For Osteoarthritis of The Kneealyek92Оценок пока нет
- 245-Article Text-456-1-10-20190606Документ6 страниц245-Article Text-456-1-10-20190606Oana RuxandraОценок пока нет
- Exploring the Feasibility of the Use of Sphygmomanometer for Assessing Hip Abductor Muscle Strength in Avascular Necrosis Patients – A Pilot StudyДокумент3 страницыExploring the Feasibility of the Use of Sphygmomanometer for Assessing Hip Abductor Muscle Strength in Avascular Necrosis Patients – A Pilot StudyInternational Journal of Innovative Science and Research TechnologyОценок пока нет
- Effects of Fatigue On Stability of Upper Extremity During Bench-Press ExerciseДокумент5 страницEffects of Fatigue On Stability of Upper Extremity During Bench-Press Exerciseyp huangОценок пока нет
- Influence of Hysteresis On Joint Position Sense in The Human Knee JointДокумент7 страницInfluence of Hysteresis On Joint Position Sense in The Human Knee JointpredragbozicОценок пока нет
- Mccre Esh 2013Документ1 страницаMccre Esh 2013Francisco Javier Luza RamosОценок пока нет
- Escamilla 2001Документ15 страницEscamilla 2001Cristina VicenteОценок пока нет
- SEGUIMIENTO A 5 AÑOS PTGH REVERSAДокумент7 страницSEGUIMIENTO A 5 AÑOS PTGH REVERSAmarcelogascon.oОценок пока нет
- The Disabled Throwing Shoulder Spectrum of Pathology Part II Evaluation and Treatment of SLAP Lesions in Throwers PDFДокумент9 страницThe Disabled Throwing Shoulder Spectrum of Pathology Part II Evaluation and Treatment of SLAP Lesions in Throwers PDFWallison LeaoОценок пока нет
- 1 s2.0 S0749806303001701 MainДокумент9 страниц1 s2.0 S0749806303001701 MainYoh ChenОценок пока нет
- Mouthguard Article ViiДокумент4 страницыMouthguard Article ViiRuxandra FitaОценок пока нет
- Muscle Activation and Kinematic Analysis During The Inclined Leg Press Exercise in Young FemalesДокумент14 страницMuscle Activation and Kinematic Analysis During The Inclined Leg Press Exercise in Young FemalesMari Calica GimenezОценок пока нет
- Wavelet Analysis of Rearfoot Loading of Patients After Medial Patellofemoral Ligament MPFL ReconstructionДокумент6 страницWavelet Analysis of Rearfoot Loading of Patients After Medial Patellofemoral Ligament MPFL ReconstructionceydaalyazhotamisОценок пока нет
- Infraspinatus Muscle AtrophyДокумент4 страницыInfraspinatus Muscle AtrophysudersonОценок пока нет
- Variabilidade Da Arquitetura Regional Do Quadríceps em Homens Treinados Avaliados Pelo Modo B e Ultrassonografia de Campo de Visão EstendidoДокумент17 страницVariabilidade Da Arquitetura Regional Do Quadríceps em Homens Treinados Avaliados Pelo Modo B e Ultrassonografia de Campo de Visão Estendidoleal thiagoОценок пока нет
- Knee Osteoarthritis (OA) Physical TherapyДокумент2 страницыKnee Osteoarthritis (OA) Physical TherapyrahmarahmatОценок пока нет
- 1 s2.0 S1526590021003163 MainДокумент26 страниц1 s2.0 S1526590021003163 MainrahmarahmatОценок пока нет
- 2022 09 27 22280421v1 FullДокумент19 страниц2022 09 27 22280421v1 FullrahmarahmatОценок пока нет
- Parkinson DiseaseДокумент9 страницParkinson DiseaseMarco GunawanОценок пока нет
- 1 s2.0 S0004951414602749 MainДокумент6 страниц1 s2.0 S0004951414602749 MainrahmarahmatОценок пока нет
- Osteoarthritis Physical Activity Care Pathway (OA-PCP) : Results of A Feasibility TrialДокумент11 страницOsteoarthritis Physical Activity Care Pathway (OA-PCP) : Results of A Feasibility TrialrahmarahmatОценок пока нет
- PMH2666 Exercises After Humerus Fracture 2019 Apr 29Документ1 страницаPMH2666 Exercises After Humerus Fracture 2019 Apr 29rahmarahmatОценок пока нет
- PIIS1063458419312099Документ6 страницPIIS1063458419312099rahmarahmatОценок пока нет
- 32 33 GP Hip Knee Orthopedic Referrals For Oa v3.2 Jan20Документ2 страницы32 33 GP Hip Knee Orthopedic Referrals For Oa v3.2 Jan20rahmarahmatОценок пока нет
- PrinciplesWoundHealing WCCSpring2011 PDFДокумент5 страницPrinciplesWoundHealing WCCSpring2011 PDFaajelОценок пока нет
- Oswestry Low Back Pain QuestionnaireДокумент4 страницыOswestry Low Back Pain QuestionnairerahmarahmatОценок пока нет
- Hurschler2004 PDFДокумент7 страницHurschler2004 PDFrahmarahmatОценок пока нет
- Astm D4910-02Документ4 страницыAstm D4910-02Saqib GhafoorОценок пока нет
- Ergonomics: Zero - Gee Ergonomic Computer and Gaming WorkstationДокумент38 страницErgonomics: Zero - Gee Ergonomic Computer and Gaming WorkstationsoumikhalderОценок пока нет
- The Ship Captain's Medical GuideДокумент239 страницThe Ship Captain's Medical Guidekukuriku13100% (1)
- Periarticular Disorders of ExtremitiesДокумент59 страницPeriarticular Disorders of Extremitiesskin_docОценок пока нет
- Chronic Lateral Elbow PainДокумент62 страницыChronic Lateral Elbow Painloopy100Оценок пока нет
- Resistance Stretch Bands: Instructions and Exercises: Douglas Williams Executive HealthДокумент14 страницResistance Stretch Bands: Instructions and Exercises: Douglas Williams Executive HealthAneury BaezОценок пока нет
- Agnikarma DR DanishДокумент47 страницAgnikarma DR DanishDrDanish Javed100% (4)
- 12-Radial & Ulnar NervesДокумент14 страниц12-Radial & Ulnar NervesHafizah HoshniОценок пока нет
- Assistive DevicesДокумент30 страницAssistive DevicesrlinaoОценок пока нет
- Bnorton Soap NotesДокумент2 страницыBnorton Soap Notesapi-285530156Оценок пока нет
- 74 Fundamental Gymnastics Positions With DiagramДокумент5 страниц74 Fundamental Gymnastics Positions With DiagramLaurence Vishnu P. MagadaОценок пока нет
- My Fracture NotesДокумент20 страницMy Fracture NotesZai AkmaОценок пока нет
- ICSE Class 9 Chapter 12 Skelatal and LocomotionДокумент4 страницыICSE Class 9 Chapter 12 Skelatal and LocomotionArpan KaurОценок пока нет
- Anatomy & Physiology: Study of the Human BodyДокумент37 страницAnatomy & Physiology: Study of the Human BodyIndu GОценок пока нет
- Session #19 SAS - AnaPhy (Lab) (Agdana, Nicole Ken)Документ10 страницSession #19 SAS - AnaPhy (Lab) (Agdana, Nicole Ken)Nicole Ken AgdanaОценок пока нет
- Supple Leopard Mobility NotesДокумент4 страницыSupple Leopard Mobility Notesbtwx67% (3)
- KINETEC 6080: Assembly and Set-Up InstructionsДокумент13 страницKINETEC 6080: Assembly and Set-Up InstructionsNgọcОценок пока нет
- Computer Workstation ErgonomicsДокумент16 страницComputer Workstation ErgonomicsJuliusSarmientoОценок пока нет
- Surgery Exam ReviewДокумент14 страницSurgery Exam ReviewYousif AlaaОценок пока нет
- Orthopedic Specialist's Clinical Authority DetailsДокумент12 страницOrthopedic Specialist's Clinical Authority DetailsGestiОценок пока нет
- 10 Weeks To Fit Program Calendar ScheduleДокумент4 страницы10 Weeks To Fit Program Calendar ScheduleAnita KokaОценок пока нет
- Non Operative Proximal Humeral FXДокумент2 страницыNon Operative Proximal Humeral FXAdmirОценок пока нет
- E C I R P: Shoulder RehabilitationДокумент7 страницE C I R P: Shoulder RehabilitationMatias QuintanillaОценок пока нет
- Merrill's Pocket Guide To Radiography 14th EditionДокумент349 страницMerrill's Pocket Guide To Radiography 14th EditionA71M100% (1)
- Basketball Shooting Errors and Corrections: by Dr. Hal WisselДокумент1 страницаBasketball Shooting Errors and Corrections: by Dr. Hal WisselEduardo H. MezzomoОценок пока нет
- Lesson Plan 3 - Safe CarriesДокумент2 страницыLesson Plan 3 - Safe CarriesGiovanni RossiОценок пока нет
- MCQsДокумент9 страницMCQsratnav_ratanОценок пока нет
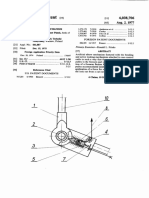
- 1977 - Artificial Elbow Mechanism - Us4038706Документ7 страниц1977 - Artificial Elbow Mechanism - Us4038706Arturo VaineОценок пока нет
- Advice For Care of Elbow FracturesДокумент2 страницыAdvice For Care of Elbow FracturesShahid KalimОценок пока нет
- Assessing Musculoskeletal (MSK) SystemДокумент8 страницAssessing Musculoskeletal (MSK) SystemKeren GaciasОценок пока нет