Вам также может понравиться
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- Redefining Cut-Points For High Symptom Burden of The Global Initiative For Chronic Obstructive Lung Disease Classification in 18,577 Patients With Chronic Obstructive Pulmonary DiseaseДокумент15 страницRedefining Cut-Points For High Symptom Burden of The Global Initiative For Chronic Obstructive Lung Disease Classification in 18,577 Patients With Chronic Obstructive Pulmonary DiseaseDejan ŽujovićОценок пока нет
- NIV - Past, Present and FutureДокумент9 страницNIV - Past, Present and FutureDejan ŽujovićОценок пока нет
- Thorax 2010 Baverstock A117 8Документ2 страницыThorax 2010 Baverstock A117 8Dejan ŽujovićОценок пока нет
- Physicians-knowledge-Plaza-J Aerosol Med Pulm Drug Deliver-2012 25 16-22-1Документ8 страницPhysicians-knowledge-Plaza-J Aerosol Med Pulm Drug Deliver-2012 25 16-22-1Dejan ŽujovićОценок пока нет
- Serbia: WHO Framework Convention On Tobacco Control (WHO FCTC) StatusДокумент12 страницSerbia: WHO Framework Convention On Tobacco Control (WHO FCTC) StatusDejan ŽujovićОценок пока нет
- Bipap A30 Specification / Part NumbersДокумент2 страницыBipap A30 Specification / Part NumbersDejan ŽujovićОценок пока нет
- From COPD To Chronic Systemic Inflammatory SyndromeДокумент9 страницFrom COPD To Chronic Systemic Inflammatory SyndromeDejan ŽujovićОценок пока нет
- Serbia: 2016 TOTAL POPULATION: 8 820 000 2016 TOTAL DEATHS: 107 000Документ1 страницаSerbia: 2016 TOTAL POPULATION: 8 820 000 2016 TOTAL DEATHS: 107 000Dejan ŽujovićОценок пока нет
- Articles: BackgroundДокумент9 страницArticles: BackgroundDejan ŽujovićОценок пока нет
- ACOSДокумент14 страницACOSDejan ŽujovićОценок пока нет
- Mukolitici U HOBPДокумент3 страницыMukolitici U HOBPDejan ŽujovićОценок пока нет
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5795)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (345)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1091)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- TEF5-OFF Frontal Electronic TimerДокумент4 страницыTEF5-OFF Frontal Electronic TimerWhendi BmОценок пока нет
- Statistical Mechanics PDFДокумент578 страницStatistical Mechanics PDFraymon6666100% (6)
- Material Specifications: Low Carbon Steel, Hot Rolled Sheet and StripДокумент5 страницMaterial Specifications: Low Carbon Steel, Hot Rolled Sheet and Striptim0% (1)
- Disorders of The Endocrine System and Dental ManagementДокумент63 страницыDisorders of The Endocrine System and Dental ManagementSanni FatimaОценок пока нет
- Starlift MetricДокумент2 страницыStarlift MetricCralesОценок пока нет
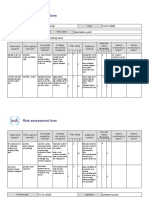
- Risk Assessment Project Iosh - MsДокумент2 страницыRisk Assessment Project Iosh - MsSanjeev Kumar75% (32)
- Nonlinear Analysis and Optimal Design of Reinforced Concrete Plates and ShellsДокумент17 страницNonlinear Analysis and Optimal Design of Reinforced Concrete Plates and Shellsrodain najjarОценок пока нет
- Elevator ControlДокумент3 страницыElevator ControlNATHANОценок пока нет
- NSO SPRДокумент9 страницNSO SPRADITYA SINGHОценок пока нет
- Unusual and Marvelous MapsДокумент33 страницыUnusual and Marvelous MapsRajarajan100% (1)
- TM TC For NanosatelliteДокумент4 страницыTM TC For NanosatelliteSreeja SujithОценок пока нет
- The Effective SpanДокумент4 страницыThe Effective SpanMohamed FarahОценок пока нет
- Art 16-18Документ528 страницArt 16-18ErudíhenОценок пока нет
- GenesДокумент33 страницыGenesJerick RoxasОценок пока нет
- Air Tunnels: Submitted By: Priyanka Sinha SK MD Sibli Akram Ananya Sreyansri NandaДокумент8 страницAir Tunnels: Submitted By: Priyanka Sinha SK MD Sibli Akram Ananya Sreyansri NandaPriyanka SinhaОценок пока нет
- Ace of Spades + Outlaw 125 2019Документ85 страницAce of Spades + Outlaw 125 2019Nelson RodrigoОценок пока нет
- SV9000 Series Products Intrduction PDFДокумент90 страницSV9000 Series Products Intrduction PDFhamph113Оценок пока нет
- Be Project Presentation SuspensionДокумент17 страницBe Project Presentation SuspensionGabrielОценок пока нет
- Civil 416Документ2 страницыCivil 416tskh11Оценок пока нет
- Kasuti of KarnatakaДокумент2 страницыKasuti of KarnatakarhlkОценок пока нет
- Nervous SystemДокумент40 страницNervous SystemJaneОценок пока нет
- Primbon Command 3GДокумент3 страницыPrimbon Command 3GEriska FebriantoОценок пока нет
- Pakistan PresentationДокумент17 страницPakistan PresentationYaseen Khan100% (1)
- Animal Whisperer PDFДокумент4 страницыAnimal Whisperer PDFKevinPriestmanОценок пока нет
- Classification of Tooth StainingДокумент4 страницыClassification of Tooth StainingYAMUNA M.D.S. PAEDODONTICS & PREVENTIVE DENTISTRYОценок пока нет
- Foods 09 01560 PDFДокумент10 страницFoods 09 01560 PDFkim cheОценок пока нет
- Multical® 402: Data SheetДокумент20 страницMultical® 402: Data SheetSundar RamasamyОценок пока нет
- Natural Topography of PakistanДокумент25 страницNatural Topography of Pakistansatayish100% (1)
- Ornament of Clear RealizationДокумент11 страницOrnament of Clear RealizationPrachi AryaОценок пока нет
- Preventive Pump SetДокумент67 страницPreventive Pump Setwtpstp sardОценок пока нет