Вам также может понравиться
- Fisiologi Ereksi in Amasi Genital Pria: Priapism ProstatitisДокумент1 страницаFisiologi Ereksi in Amasi Genital Pria: Priapism ProstatitisSiti RuchjayaniОценок пока нет
- 4上cs 第一次心智圖Документ1 страница4上cs 第一次心智圖Eric LinОценок пока нет
- MENISCOДокумент26 страницMENISCOSarah SiraitОценок пока нет
- Fatimah Mind Map Pemicu 2 UroДокумент1 страницаFatimah Mind Map Pemicu 2 UroSiti RuchjayaniОценок пока нет
- Chronic Glomerulonephritis in DetailДокумент9 страницChronic Glomerulonephritis in Detailfile fileОценок пока нет
- Backup of ANTIMICROBIALS PRINTABLEДокумент4 страницыBackup of ANTIMICROBIALS PRINTABLEinvading_jam7582100% (1)
- Surgery OSCE PDFДокумент26 страницSurgery OSCE PDFWisal Merghani100% (4)
- Orthopaedic: Congenital, Infection, Neoplasia, Trauma, AppandegesДокумент1 страницаOrthopaedic: Congenital, Infection, Neoplasia, Trauma, AppandegesdinsОценок пока нет
- OSCE 2020 AdamantiumДокумент4 страницыOSCE 2020 Adamantiummerosaber622001Оценок пока нет
- PP Exam 4: Everything That Is in Red Came From Test Your Knowledge!Документ15 страницPP Exam 4: Everything That Is in Red Came From Test Your Knowledge!netanya DoanОценок пока нет
- TermoregulasiДокумент20 страницTermoregulasiAlfiyya nur marhdiyyahОценок пока нет
- Surgery Upper GI HemorrhageДокумент6 страницSurgery Upper GI HemorrhagesarthaktimbadiyaОценок пока нет
- Bed Site TeachingДокумент15 страницBed Site TeachingzainiОценок пока нет
- Isk BSKДокумент5 страницIsk BSKAndy F MonroeОценок пока нет
- 5.2 Renal Masses and Congenital AnomaliesДокумент9 страниц5.2 Renal Masses and Congenital AnomaliesMaria roxanne HernandezОценок пока нет
- Urinary StoneДокумент5 страницUrinary StoneThakoon TtsОценок пока нет
- Practical UtzДокумент3 страницыPractical UtzCathleenCostillasGuiraОценок пока нет
- Intrahepatic Biliary Tract DiseaseДокумент1 страницаIntrahepatic Biliary Tract DiseaseMaryam FadahОценок пока нет
- Lumps and SwellingsДокумент3 страницыLumps and SwellingsEarn ChiОценок пока нет
- Biliary Tract DiseasesДокумент13 страницBiliary Tract DiseasesYara YousefОценок пока нет
- Approach To Abdominal PainДокумент4 страницыApproach To Abdominal PainShamen KohОценок пока нет
- Gastrointestinal OsmosisДокумент174 страницыGastrointestinal OsmosisfabicontrerasenarmОценок пока нет
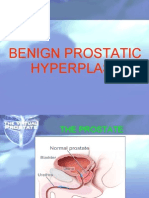
- Benign Prostatic HyperplasiaДокумент5 страницBenign Prostatic Hyperplasiatabangin_hilario100% (1)
- RADIO Liver and GallbladderДокумент6 страницRADIO Liver and GallbladderJeffrey RamosОценок пока нет
- Red Vascular: Polygonal Cells Growing in Nests or Cords Lamellae of Dense CollagenДокумент3 страницыRed Vascular: Polygonal Cells Growing in Nests or Cords Lamellae of Dense CollagenMaryam FadahОценок пока нет
- AmebasДокумент3 страницыAmebasNaomi NicoleОценок пока нет
- Darurat Trauma Uro Print 1.3.13Документ82 страницыDarurat Trauma Uro Print 1.3.13Surya ArhОценок пока нет
- Handouts - Ref PeriopДокумент10 страницHandouts - Ref PerioproseОценок пока нет
- Ileus FixДокумент26 страницIleus FixSelly Chasandra100% (1)
- Acute Scrotal Pain in Adults and Adolescents - Approach To The Patient - DynaMedДокумент66 страницAcute Scrotal Pain in Adults and Adolescents - Approach To The Patient - DynaMedSebastian ChavesОценок пока нет
- Renal - PathДокумент23 страницыRenal - PathKimberly KanemitsuОценок пока нет
- Urinary RetentionДокумент64 страницыUrinary RetentionAntonioIndraTОценок пока нет
- Acute Urinary Retention: Ronald TanggoДокумент63 страницыAcute Urinary Retention: Ronald TanggoKalista ApriyaniОценок пока нет
- DDX - Gastrointestinal Disorders ChartДокумент21 страницаDDX - Gastrointestinal Disorders Chartapi-26938624100% (2)
- Acute Abdominal Bleeding - HandoutДокумент10 страницAcute Abdominal Bleeding - HandoutMohamed FigoОценок пока нет
- Hand Out Biliary Tract Sarajevo 2016-06-18Документ14 страницHand Out Biliary Tract Sarajevo 2016-06-18Тетяна МагасьОценок пока нет
- Pathway Tumor GinjalДокумент1 страницаPathway Tumor GinjalElizabeth VickiОценок пока нет
- NCMB312 RLE Week 1Документ22 страницыNCMB312 RLE Week 1lindzy.amurao01Оценок пока нет
- Approach To A Case of HematuriaДокумент23 страницыApproach To A Case of HematuriaSunil KumarОценок пока нет
- Approach To A Case of HematuriaДокумент23 страницыApproach To A Case of HematuriaSunil KumarОценок пока нет
- Pathophysiology DiagramДокумент1 страницаPathophysiology Diagramzebzeb STEMAОценок пока нет
- Uac VS UvcДокумент1 страницаUac VS UvcJunaidahMubarakAliОценок пока нет
- Chronic Renal Failure: Concise Long Case ApproachДокумент3 страницыChronic Renal Failure: Concise Long Case ApproachUsman Ali AkbarОценок пока нет
- Urologic Trauma: Medical Faculty, University of Sumatera UtaraДокумент42 страницыUrologic Trauma: Medical Faculty, University of Sumatera UtaraMaya Asharie HarahapОценок пока нет
- b9 PKM 2 Urinary Retention Dr. Christian Ronald Tanggo Sp.uДокумент63 страницыb9 PKM 2 Urinary Retention Dr. Christian Ronald Tanggo Sp.uDaud ParluhutanОценок пока нет
- Kidney StonesДокумент1 страницаKidney StonesMo'ayad OkylanОценок пока нет
- Subspec Urology: GU TumorsДокумент5 страницSubspec Urology: GU TumorsThakoon TtsОценок пока нет
- Hematuria: Preseptor: Dr. Sawkar Vijay Pramod, Sp.UДокумент39 страницHematuria: Preseptor: Dr. Sawkar Vijay Pramod, Sp.UFIKRI MUHAMMADОценок пока нет
- Pathophysiology (kidney ppt 자료)Документ5 страницPathophysiology (kidney ppt 자료)tnwls4031Оценок пока нет
- Embryology of The Renal SystemДокумент8 страницEmbryology of The Renal SystemStd DlshsiОценок пока нет
- Upper GITДокумент13 страницUpper GITKiara Govender100% (1)
- MS 2Документ8 страницMS 2Vincent AmitОценок пока нет
- Cardio FinalsДокумент17 страницCardio FinalsNadia AbdurasidОценок пока нет
- GIT Causes-Alcohol LevelДокумент8 страницGIT Causes-Alcohol LevelPuteri Atiqah SyaqilaОценок пока нет
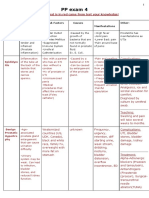
- Disease Characteristics of The Pain Other Associated Symptoms Main Physical Findings Sonography Findings AdenomyosisДокумент2 страницыDisease Characteristics of The Pain Other Associated Symptoms Main Physical Findings Sonography Findings AdenomyosisaliyahОценок пока нет
- Lung CaДокумент1 страницаLung CaAqila MumtazОценок пока нет
- VertigoДокумент50 страницVertigosaltoftheearthlightoftheworld506Оценок пока нет
- HVZ TratamientoДокумент12 страницHVZ TratamientoRamiro LimaОценок пока нет
- Fluid Electrolyte ImbalanceДокумент46 страницFluid Electrolyte ImbalanceAxsa AlexОценок пока нет
- Jurnal Psikiatri 6Документ8 страницJurnal Psikiatri 6Dati DelianaОценок пока нет
- Farmakoterapi DispilidemiaДокумент33 страницыFarmakoterapi DispilidemiavivinОценок пока нет
- PNLE III For Medical Surgical NursingДокумент13 страницPNLE III For Medical Surgical NursingZymer Lee Abasolo100% (1)
- Frozen Shoulder RevisedДокумент17 страницFrozen Shoulder Revisednerissa arvianaОценок пока нет
- Behavioral Health Care PlanДокумент13 страницBehavioral Health Care Planapi-521003884Оценок пока нет
- NCM 112 Endterm Care of Clients With Problems in Cellular Aberrations Acute and ChronicДокумент8 страницNCM 112 Endterm Care of Clients With Problems in Cellular Aberrations Acute and ChronicApril FlorendoОценок пока нет
- Chapter 15 - Autoimmunity - Review QuestionsДокумент2 страницыChapter 15 - Autoimmunity - Review QuestionsTreyton Sekani LopezОценок пока нет
- IASTM - jOURNALДокумент12 страницIASTM - jOURNALviorelОценок пока нет
- Can Present As:: Clinical Communication SkillsДокумент3 страницыCan Present As:: Clinical Communication SkillsMazin obeidОценок пока нет
- Fungal Lung DiseasesДокумент28 страницFungal Lung Diseasessultan khabeebОценок пока нет
- PACK Global Adult Ebook 2018Документ128 страницPACK Global Adult Ebook 2018Gabriel DutraОценок пока нет
- Diseases of Nerve, Muscle and Neuromuscular JunctionДокумент50 страницDiseases of Nerve, Muscle and Neuromuscular JunctionMalueth AnguiОценок пока нет
- Need Motivates The Behaviour of A Person.: Human Needs TheoryДокумент8 страницNeed Motivates The Behaviour of A Person.: Human Needs TheoryDan Ataniel EnsaladaОценок пока нет
- Orthopedic ConditionsДокумент11 страницOrthopedic ConditionsErin Hoffmann100% (3)
- Os 1Документ4 страницыOs 1rizwanОценок пока нет
- Author: Section Editor: Deputy EditorДокумент20 страницAuthor: Section Editor: Deputy EditorEvy Alvionita YurnaОценок пока нет
- Role of Massage Therapy On Reduction of Neonatal Hyperbilirubinemia in Term and Preterm Neonates: A Review of Clinical TrialsДокумент10 страницRole of Massage Therapy On Reduction of Neonatal Hyperbilirubinemia in Term and Preterm Neonates: A Review of Clinical TrialsEni RahmawatiОценок пока нет
- Bone Marrow AbnormalitiesДокумент24 страницыBone Marrow AbnormalitiesUmar BakshiОценок пока нет
- Keratitis Ec Infiltrat OS: Case Presentation IДокумент30 страницKeratitis Ec Infiltrat OS: Case Presentation IAnonymous LxoYFc4mk9Оценок пока нет
- Towards Better Patient Care Drugs To Avoid in 2024Документ11 страницTowards Better Patient Care Drugs To Avoid in 2024Juan Diego Sánchez BaenaОценок пока нет
- Vi Psa Pres Common Eye Conditions Aug10 3.08.29 PMДокумент58 страницVi Psa Pres Common Eye Conditions Aug10 3.08.29 PMSarthak KabiОценок пока нет
- Piogenic Cocci: Ania Kurniawati PD, Dr. MkesДокумент58 страницPiogenic Cocci: Ania Kurniawati PD, Dr. MkesSilmi Zhillan Nur RahmanОценок пока нет
- Qtern 84413Документ19 страницQtern 84413Manoj KaluvakotaОценок пока нет
- Drug Study On Emergency Drugs Final - )Документ12 страницDrug Study On Emergency Drugs Final - )wen_pil100% (3)
- Laporan Jaga 6 9 2019Документ20 страницLaporan Jaga 6 9 2019Nitari Rahmi PutriОценок пока нет
- Respiratory Distress Syndrome 1Документ35 страницRespiratory Distress Syndrome 1Marrah Avila AcuinОценок пока нет
- Mixed Radiolucent/radio-Opaque Jaw Lesions (Schematic Radiographic Approach)Документ1 страницаMixed Radiolucent/radio-Opaque Jaw Lesions (Schematic Radiographic Approach)Vansh Vardhan MadaharОценок пока нет
- The Obesity Code: Unlocking the Secrets of Weight LossОт EverandThe Obesity Code: Unlocking the Secrets of Weight LossРейтинг: 4 из 5 звезд4/5 (6)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsОт EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsОценок пока нет
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeОт EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeРейтинг: 2 из 5 звезд2/5 (1)
- The Age of Magical Overthinking: Notes on Modern IrrationalityОт EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityРейтинг: 4 из 5 звезд4/5 (24)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaОт EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisОт EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisРейтинг: 4.5 из 5 звезд4.5/5 (42)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedОт EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedРейтинг: 5 из 5 звезд5/5 (80)
- ADHD is Awesome: A Guide to (Mostly) Thriving with ADHDОт EverandADHD is Awesome: A Guide to (Mostly) Thriving with ADHDРейтинг: 5 из 5 звезд5/5 (1)
- Self-Care for Autistic People: 100+ Ways to Recharge, De-Stress, and Unmask!От EverandSelf-Care for Autistic People: 100+ Ways to Recharge, De-Stress, and Unmask!Рейтинг: 5 из 5 звезд5/5 (1)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsОт EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsРейтинг: 5 из 5 звезд5/5 (1)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisОт EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisРейтинг: 4 из 5 звезд4/5 (1)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.От EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Рейтинг: 4.5 из 5 звезд4.5/5 (110)
- Gut: the new and revised Sunday Times bestsellerОт EverandGut: the new and revised Sunday Times bestsellerРейтинг: 4 из 5 звезд4/5 (392)
- Why We Die: The New Science of Aging and the Quest for ImmortalityОт EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityРейтинг: 4 из 5 звезд4/5 (3)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsОт EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsРейтинг: 4.5 из 5 звезд4.5/5 (169)
- Cult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryОт EverandCult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryРейтинг: 4 из 5 звезд4/5 (44)
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessОт EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessРейтинг: 4.5 из 5 звезд4.5/5 (328)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsОт EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsРейтинг: 3.5 из 5 звезд3.5/5 (3)
- When the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisОт EverandWhen the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisРейтинг: 3.5 из 5 звезд3.5/5 (2)
- Sleep Stories for Adults: Overcome Insomnia and Find a Peaceful AwakeningОт EverandSleep Stories for Adults: Overcome Insomnia and Find a Peaceful AwakeningРейтинг: 4 из 5 звезд4/5 (3)
- Gut: The Inside Story of Our Body's Most Underrated Organ (Revised Edition)От EverandGut: The Inside Story of Our Body's Most Underrated Organ (Revised Edition)Рейтинг: 4 из 5 звезд4/5 (378)
- To Explain the World: The Discovery of Modern ScienceОт EverandTo Explain the World: The Discovery of Modern ScienceРейтинг: 3.5 из 5 звезд3.5/5 (51)
- The Marshmallow Test: Mastering Self-ControlОт EverandThe Marshmallow Test: Mastering Self-ControlРейтинг: 4.5 из 5 звезд4.5/5 (58)