Вам также может понравиться
- Osteoarthritis Is A Serious DiseaseДокумент4 страницыOsteoarthritis Is A Serious DiseaseSCRIBDОценок пока нет
- NIH Public Access: Author ManuscriptДокумент15 страницNIH Public Access: Author Manuscriptfidatahir93Оценок пока нет
- Osteoarthritis-Patterns, Cardio-Metabolic Risk Factors and Risk of All-Cause Mortality: 20 Years Follow-Up in Patients After Hip or Knee ReplacementДокумент9 страницOsteoarthritis-Patterns, Cardio-Metabolic Risk Factors and Risk of All-Cause Mortality: 20 Years Follow-Up in Patients After Hip or Knee Replacementaxl___Оценок пока нет
- Biomarkers of (Osteo) Arthritis: EditorialДокумент6 страницBiomarkers of (Osteo) Arthritis: EditorialeliasОценок пока нет
- Bir RellДокумент12 страницBir RellGaudeamus IgiturОценок пока нет
- Epidemiologyofosteoarthritis: Tuhina Neogi,, Yuqing ZhangДокумент19 страницEpidemiologyofosteoarthritis: Tuhina Neogi,, Yuqing ZhangIkmal ShahromОценок пока нет
- A Perspective On Osteoarthritis Research in Singapore: ReviewДокумент9 страницA Perspective On Osteoarthritis Research in Singapore: ReviewRhinaОценок пока нет
- Theburdenofosteoarthritis Inolderadults: Gillian A. Hawker,, Lauren K. KingДокумент12 страницTheburdenofosteoarthritis Inolderadults: Gillian A. Hawker,, Lauren K. KingabdulfatahalhemeryОценок пока нет
- Osteoarthritis: Pathology, Diagnosis, and Treatment OptionsДокумент19 страницOsteoarthritis: Pathology, Diagnosis, and Treatment OptionsTrino Rangel FonsecaОценок пока нет
- I. Background: The Hand (PDF - 1.31MB) Hip (PDF - 1.31MB) Knee Top of PageДокумент6 страницI. Background: The Hand (PDF - 1.31MB) Hip (PDF - 1.31MB) Knee Top of PageRisna Allyn AnnisaОценок пока нет
- Researc OrofasdialДокумент18 страницResearc OrofasdialREANANDA MUBARAK SUGIARTOОценок пока нет
- Osteoarthritis: in The ClinicДокумент16 страницOsteoarthritis: in The ClinicKurosaki IchigoОценок пока нет
- Osteoarthritis: OsteoartriteДокумент9 страницOsteoarthritis: OsteoartriteSofia Cerezo MuñozОценок пока нет
- Pereira 2015Документ9 страницPereira 2015Amalia RosaОценок пока нет
- Prevention of MSKДокумент14 страницPrevention of MSKArham ShamsiОценок пока нет
- Genes: Knee Osteoarthritis: A Review of Pathogenesis and State-Of-The-Art Non-Operative Therapeutic ConsiderationsДокумент35 страницGenes: Knee Osteoarthritis: A Review of Pathogenesis and State-Of-The-Art Non-Operative Therapeutic ConsiderationsJeevan VelanОценок пока нет
- Bliddal 2014Документ9 страницBliddal 2014ANAОценок пока нет
- Impact of Osteoarthritis On Activities of Daily LiДокумент9 страницImpact of Osteoarthritis On Activities of Daily LiSetiaty PandiaОценок пока нет
- Assessment of Fracture Risk and Its Application To Screening For Postmenopausal Osteoporosis Synopsis of A WHO ReportДокумент14 страницAssessment of Fracture Risk and Its Application To Screening For Postmenopausal Osteoporosis Synopsis of A WHO ReportKhủngLongSiêuNguyHiểmОценок пока нет
- Oa Glyn-Jones2015Документ12 страницOa Glyn-Jones2015Azmia TabahОценок пока нет
- Fox - Treatment of Knee Osteoarthritis - ER 2010 2 PDFДокумент11 страницFox - Treatment of Knee Osteoarthritis - ER 2010 2 PDFdrksk355Оценок пока нет
- Healthcare 11 02340Документ14 страницHealthcare 11 02340kiwelem698Оценок пока нет
- HHS Public Access: Imaging of Osteoarthritis in Geriatric PatientsДокумент16 страницHHS Public Access: Imaging of Osteoarthritis in Geriatric PatientsNaufal K. YurnadiОценок пока нет
- Comparing The Effects of Ultrasound and Microwave Physiotherapy Treatments On Knee Osteoarthritis by MEasuring Osteocalcin Level and Erythrocyte Sedimentation Rate in BloodДокумент5 страницComparing The Effects of Ultrasound and Microwave Physiotherapy Treatments On Knee Osteoarthritis by MEasuring Osteocalcin Level and Erythrocyte Sedimentation Rate in BloodAlfiana ApriliaОценок пока нет
- Prevalence of Knee Osteoarthritis, Risk Factors, and Quality of Life: The Fifth Korean National Health and Nutrition Examination SurveyДокумент9 страницPrevalence of Knee Osteoarthritis, Risk Factors, and Quality of Life: The Fifth Korean National Health and Nutrition Examination SurveyTanvirОценок пока нет
- InTech-Knee Pain in Adults Adolescents Diagnosis and TreatmentДокумент32 страницыInTech-Knee Pain in Adults Adolescents Diagnosis and Treatmentevil freakОценок пока нет
- Journal of Hand Therapy: JHT R C A #408. Special Issue: WristДокумент10 страницJournal of Hand Therapy: JHT R C A #408. Special Issue: WristcendyjulianaОценок пока нет
- Calcific Tendinitis of The Rotator Cuff State of The Art in Diagnosis PDFДокумент8 страницCalcific Tendinitis of The Rotator Cuff State of The Art in Diagnosis PDFItai IzhakОценок пока нет
- Fmed 08 773417Документ12 страницFmed 08 773417Hadley AuliaОценок пока нет
- Seminars in Arthritis and Rheumatism: Jasvinder A. Singh, Angelo GaffoДокумент6 страницSeminars in Arthritis and Rheumatism: Jasvinder A. Singh, Angelo GaffoVANESSA GLORIA POLIIОценок пока нет
- Osteoarthritis: Epidemiology, Risk Factors, and PathophysiologyДокумент10 страницOsteoarthritis: Epidemiology, Risk Factors, and PathophysiologyMaryama AflahaОценок пока нет
- Epidemiología de La ArtrosisДокумент8 страницEpidemiología de La ArtrosisSandraОценок пока нет
- HHS Public Access: Diagnosis and Treatment of Hip and Knee Osteoarthritis: A ReviewДокумент25 страницHHS Public Access: Diagnosis and Treatment of Hip and Knee Osteoarthritis: A ReviewJose PerezОценок пока нет
- HHS Public Access: Epidemiology of Osteoarthritis: Literature UpdateДокумент16 страницHHS Public Access: Epidemiology of Osteoarthritis: Literature UpdateKhairul AsriОценок пока нет
- F. Lapi, M. Simonetti, R. Michieli, A. Pasqua, M.L. Brandi, B. Frediani, C. Cricelli, G. MazzagliaДокумент6 страницF. Lapi, M. Simonetti, R. Michieli, A. Pasqua, M.L. Brandi, B. Frediani, C. Cricelli, G. Mazzagliafirdha afghaniОценок пока нет
- Effects of Exercise and Physical Activity On Knee OsteoarthritisДокумент9 страницEffects of Exercise and Physical Activity On Knee OsteoarthritisJoseph LimОценок пока нет
- Strategies For Optimising Musculoskeletal Health in The 21 CenturyДокумент15 страницStrategies For Optimising Musculoskeletal Health in The 21 CenturyMarkChristianRobleAlmazanОценок пока нет
- Orthopedic May 2013Документ11 страницOrthopedic May 2013javi222222Оценок пока нет
- Lung Disease in Rheumatoid ArthritisОт EverandLung Disease in Rheumatoid ArthritisAryeh FischerОценок пока нет
- Surgical Oncology: SciencedirectДокумент8 страницSurgical Oncology: SciencedirectMIGUEL MORENOОценок пока нет
- The Epidemiology of Extra-Articular Manifestations in Ankylosing Spondylitis: A Population-Based Matched Cohort StudyДокумент7 страницThe Epidemiology of Extra-Articular Manifestations in Ankylosing Spondylitis: A Population-Based Matched Cohort StudyAdriana VladutuОценок пока нет
- FulltextДокумент11 страницFulltextajeet84bhu2920Оценок пока нет
- Learning Issues FanyДокумент3 страницыLearning Issues Fanyfaridatul jannahОценок пока нет
- 1-Disease MechanismsДокумент5 страниц1-Disease MechanismsMarian Dane PunzalanОценок пока нет
- 2018-1 - Classifications in Brief Tonnis Classification of Hip OsteoarthritisДокумент5 страниц2018-1 - Classifications in Brief Tonnis Classification of Hip OsteoarthritisjosedgalvismdОценок пока нет
- Obesity & Osteoarthritis PDFДокумент9 страницObesity & Osteoarthritis PDFTaufik Ramadhan BiyaОценок пока нет
- Manifestaciones Clinicas de OsteoartritisДокумент10 страницManifestaciones Clinicas de OsteoartritisMeny GarciaОценок пока нет
- Biomolecules: TRPV Channels in Osteoarthritis: A Comprehensive ReviewДокумент25 страницBiomolecules: TRPV Channels in Osteoarthritis: A Comprehensive ReviewTedОценок пока нет
- FFFGVДокумент10 страницFFFGVyundaОценок пока нет
- Body Mass Index and Susceptibility To Knee Osteoarthritis: A Systematic Review and Meta-AnalysisДокумент7 страницBody Mass Index and Susceptibility To Knee Osteoarthritis: A Systematic Review and Meta-AnalysisAmalia RosaОценок пока нет
- 1 s2.0 S1530891X20481868 MainДокумент9 страниц1 s2.0 S1530891X20481868 MainSaugi HudaОценок пока нет
- Fragility Fracture Discriminative Ability of Radius Quantitative Ultrasound: A Systematic Review and Meta-AnalysisДокумент16 страницFragility Fracture Discriminative Ability of Radius Quantitative Ultrasound: A Systematic Review and Meta-AnalysisTarib TrifaОценок пока нет
- 5 Oa RMДокумент15 страниц5 Oa RMAhmad Nur Fikri AbrorОценок пока нет
- Epidemiology Osteoporosis Middle East and North AfricaДокумент14 страницEpidemiology Osteoporosis Middle East and North AfricaanassОценок пока нет
- Ijerph 19 10510Документ15 страницIjerph 19 10510Victor CristianОценок пока нет
- Musculo-Skeletal Disorders - Polymalagia ArthritisДокумент22 страницыMusculo-Skeletal Disorders - Polymalagia ArthritisKyle J. NortonОценок пока нет
- 2016 Article 89Документ20 страниц2016 Article 89soylahijadeunvampiroОценок пока нет
- Best Practice & Research Clinical RheumatologyДокумент10 страницBest Practice & Research Clinical RheumatologyLis Setiyo NingrumОценок пока нет
- John McKnight ABCD - The Essentials - 2Документ4 страницыJohn McKnight ABCD - The Essentials - 2lindapramusintaОценок пока нет
- Template Life Science BaruДокумент10 страницTemplate Life Science BarulindapramusintaОценок пока нет
- BMI Relationship to Rheumatoid ArthritisДокумент5 страницBMI Relationship to Rheumatoid ArthritislindapramusintaОценок пока нет
- Core Stability Exercise PrinciplesДокумент6 страницCore Stability Exercise Principlesphysioali0% (2)
- Anwar, 2009Документ11 страницAnwar, 2009Fauziah MrdОценок пока нет
- Core Stability Exercise PrinciplesДокумент6 страницCore Stability Exercise Principlesphysioali0% (2)
- PDFДокумент7 страницPDFlindapramusintaОценок пока нет
- Stanford HAQ 20-Item Disability Scale: at This Moment, Are You Able ToДокумент4 страницыStanford HAQ 20-Item Disability Scale: at This Moment, Are You Able TolindapramusintaОценок пока нет
- Relacion Entre Trabajo de CORE y Rendimiento en Futbolistas PDFДокумент5 страницRelacion Entre Trabajo de CORE y Rendimiento en Futbolistas PDFlindapramusintaОценок пока нет
- Core Stability InternasionalДокумент8 страницCore Stability InternasionallindapramusintaОценок пока нет
- Core Stability Training Applications To Sports Conditioning ProgramsДокумент8 страницCore Stability Training Applications To Sports Conditioning ProgramsPhillipa Louise Kimberley100% (1)
- S&C J Article Integrated Approach To Training Core Stability ArticleДокумент12 страницS&C J Article Integrated Approach To Training Core Stability ArticlelindapramusintaОценок пока нет
- Core Stability Training Applications To Sports Conditioning ProgramsДокумент8 страницCore Stability Training Applications To Sports Conditioning ProgramsPhillipa Louise Kimberley100% (1)
- Core StabilityДокумент8 страницCore StabilitylindapramusintaОценок пока нет
- Cardiovascular SytemДокумент56 страницCardiovascular SytemlindapramusintaОценок пока нет
- Jurnal 10 - Ganda Sigalingging1Документ10 страницJurnal 10 - Ganda Sigalingging1umamfazlurrahmanОценок пока нет
- IntegumentaryДокумент8 страницIntegumentaryRamon Carlo AlmiranezОценок пока нет
- JKPT 31 317Документ5 страницJKPT 31 317Sofia VarguezОценок пока нет
- экзамДокумент65 страницэкзамShubham PandeyОценок пока нет
- The Adrenal Thyroid Revolution Supplement Guide: SOS RX: Daily Dose SupplementsДокумент8 страницThe Adrenal Thyroid Revolution Supplement Guide: SOS RX: Daily Dose SupplementsPetra JobovaОценок пока нет
- Biomecanica Da ObesidadeДокумент9 страницBiomecanica Da ObesidadehgtrainerОценок пока нет
- Varmam UsesДокумент34 страницыVarmam UsesVasuthaОценок пока нет
- RMT KLSF DR Blondina 2009Документ21 страницаRMT KLSF DR Blondina 2009Fadhly SharimanОценок пока нет
- Medical Translation PDFДокумент29 страницMedical Translation PDFkltm azzОценок пока нет
- Case Study 3 - Knee PainДокумент12 страницCase Study 3 - Knee PainElizabeth Ho100% (9)
- To Study The Effects of Muscle Energy Technique With Conventional Treatment Along With Cellular Nutrition in Patients With Knee OsteoarthritisДокумент5 страницTo Study The Effects of Muscle Energy Technique With Conventional Treatment Along With Cellular Nutrition in Patients With Knee OsteoarthritisZickey MaryaОценок пока нет
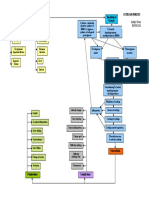
- Osteoarthritis Concept MapДокумент1 страницаOsteoarthritis Concept Mapnursing concept maps0% (1)
- Treatment of Canine OsteoarthritisДокумент7 страницTreatment of Canine OsteoarthritissatyadwiparthaОценок пока нет
- MEDICAL COLLEGE EXAM COVERS KEY TERMSДокумент7 страницMEDICAL COLLEGE EXAM COVERS KEY TERMSFev BanataoОценок пока нет
- Nursing Lecture OrthopedicДокумент24 страницыNursing Lecture OrthopedicAedge010100% (2)
- Rotator CuffДокумент11 страницRotator CuffineedsheetzОценок пока нет
- Hydrotherapy Application PhysiotherapyДокумент21 страницаHydrotherapy Application PhysiotherapyavetvuОценок пока нет
- 12 Health Benefits of PomegranateДокумент10 страниц12 Health Benefits of Pomegranateparajms8778Оценок пока нет
- Simple FixesДокумент3 страницыSimple FixessanimaidinОценок пока нет
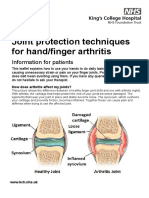
- Joint protection techniques for arthritisДокумент5 страницJoint protection techniques for arthritisXouya SuizenОценок пока нет
- Pantoja Et Al. - 2019 - Prevalence of Degenerative Joint Disease of The TeДокумент14 страницPantoja Et Al. - 2019 - Prevalence of Degenerative Joint Disease of The TeMarco Saavedra BurgosОценок пока нет
- DDGFДокумент5 страницDDGFUtkaRsh ShArmaОценок пока нет
- Case On Osteo Arthritis COORECTEDДокумент29 страницCase On Osteo Arthritis COORECTEDjohnleeeОценок пока нет
- Kevin J. Bozic, MD, MBA: Harry E. Rubash, MDДокумент48 страницKevin J. Bozic, MD, MBA: Harry E. Rubash, MDHervis FantiniОценок пока нет
- Organisation of The Motor Cortex Differs OaДокумент11 страницOrganisation of The Motor Cortex Differs OaThiago LoureiroОценок пока нет
- The 2020 NBA Orthobiologics Consensus Statement (2021)Документ9 страницThe 2020 NBA Orthobiologics Consensus Statement (2021)Nuno PaisОценок пока нет
- OSTEOARTHRITISДокумент36 страницOSTEOARTHRITISHzm Mus83% (12)
- Ayurvedic-Herbal Medicine For OSTEOARTHRITIS (Sandhivata)Документ3 страницыAyurvedic-Herbal Medicine For OSTEOARTHRITIS (Sandhivata)Anonymous AMmNGgPОценок пока нет
- Aaa - THAMARA - Comparing Hot Pack, Short-Wave Diathermy, Ultrasound, and Tens On Isokinetic Strength, Pain and Functional StatusДокумент9 страницAaa - THAMARA - Comparing Hot Pack, Short-Wave Diathermy, Ultrasound, and Tens On Isokinetic Strength, Pain and Functional StatusBruno FellipeОценок пока нет
- Total Knee Replacement SurgeryДокумент8 страницTotal Knee Replacement SurgeryAnuj KhuranaОценок пока нет
- Osteoarthritis Information BookletДокумент27 страницOsteoarthritis Information BookletRiyan mulya sukma 094Оценок пока нет