Вам также может понравиться
- Ni Komang Saraswita Laksmi: Puskesmas Mendoyo I, Bali, IndonesiaДокумент6 страницNi Komang Saraswita Laksmi: Puskesmas Mendoyo I, Bali, IndonesiaRirhy SaragihОценок пока нет
- Management of TetanusДокумент7 страницManagement of TetanusamutiarОценок пока нет
- Tetanus PresentationДокумент16 страницTetanus PresentationKennedy Ng'andweОценок пока нет
- Tetanus (Clostridium Tetani)Документ29 страницTetanus (Clostridium Tetani)ped medОценок пока нет
- 54 TetanusДокумент25 страниц54 Tetanusghofran001997Оценок пока нет
- TetanusДокумент37 страницTetanusMuwanga faizoОценок пока нет
- TetanusДокумент18 страницTetanusRohan TejaОценок пока нет
- TetanusДокумент5 страницTetanusales_sandriОценок пока нет
- What Is Tetanus?: Clostridium Tetani or The Tetanus Bacillus Is A Slender, Gram-Positive, Anaerobic Rod That MayДокумент5 страницWhat Is Tetanus?: Clostridium Tetani or The Tetanus Bacillus Is A Slender, Gram-Positive, Anaerobic Rod That MayraechcmОценок пока нет
- TetanusДокумент4 страницыTetanusAjay Pal NattОценок пока нет
- Tet AnusДокумент27 страницTet AnusJarkey SawkneeОценок пока нет
- TetanusДокумент7 страницTetanusArnella HutagalungОценок пока нет
- Tetanus As A Childhood Disease Common in Children Under Age 5Документ12 страницTetanus As A Childhood Disease Common in Children Under Age 5Adediran DolapoОценок пока нет
- Tetanus NeonatorumДокумент6 страницTetanus Neonatorumeagame gamersОценок пока нет
- Tetanus DeviДокумент25 страницTetanus DeviRisal MujahidinОценок пока нет
- Tetanus: DefinisiДокумент9 страницTetanus: DefinisiRiz Sanfebrian AdiatmaОценок пока нет
- The Pa Tho Physiology of TetanusДокумент3 страницыThe Pa Tho Physiology of Tetanusmai_serpicОценок пока нет
- C. Tetani FinalДокумент3 страницыC. Tetani FinalSajjad Hossain ShuvoОценок пока нет
- TetanusДокумент27 страницTetanusMohammed FareedОценок пока нет
- Neonatal TetanusДокумент44 страницыNeonatal TetanusJake MillerОценок пока нет
- Tetanus: Eu MBCHB 3 DR D M KillingoДокумент44 страницыTetanus: Eu MBCHB 3 DR D M KillingoArjay VisitacionОценок пока нет
- !tetanus MДокумент22 страницы!tetanus MWendo yayahОценок пока нет
- Signs and SymptomsДокумент6 страницSigns and Symptomsdareine22Оценок пока нет
- Tetanus PDFДокумент10 страницTetanus PDFVina MuspitaОценок пока нет
- K6 - Tetanus PEDIATRICДокумент23 страницыK6 - Tetanus PEDIATRICbanuperiahОценок пока нет
- Tetanus AДокумент3 страницыTetanus ASadaqat KhanОценок пока нет
- Management of Tetanus ComplicationДокумент6 страницManagement of Tetanus ComplicationsusiОценок пока нет
- TetanusДокумент23 страницыTetanusDhynie Soesila WahyudiОценок пока нет
- 351255266-Tetanus Id enДокумент14 страниц351255266-Tetanus Id enRezki IndriyantiyusufОценок пока нет
- Kepaniteraan Klinik Rsms - FK Upn "Veteran" Jakarta: Penguji: Dr. Hernawan, SP.SДокумент32 страницыKepaniteraan Klinik Rsms - FK Upn "Veteran" Jakarta: Penguji: Dr. Hernawan, SP.SOktaviano Satria PОценок пока нет
- Pathogenesis of TetanusДокумент2 страницыPathogenesis of TetanusKarun BhattaraiОценок пока нет
- Tetanus in Dogs Clinical Signs and ManagementДокумент10 страницTetanus in Dogs Clinical Signs and ManagementLonely WolfОценок пока нет
- Tetanus EmedicineДокумент19 страницTetanus EmedicineSapto SutardiОценок пока нет
- TetanusДокумент11 страницTetanusalief akbar RafsanjaniОценок пока нет
- TetanusДокумент3 страницыTetanusRoma Nova Pascual CabarrubiasОценок пока нет
- Tetanus PDFДокумент10 страницTetanus PDFIzzatul YazidahОценок пока нет
- TetanusДокумент4 страницыTetanuseagame gamersОценок пока нет
- 420 080 Guideline TetanusДокумент9 страниц420 080 Guideline TetanusFebrian TanОценок пока нет
- Lovely Professional University: Term Paper of Advanced MicrobiologyДокумент11 страницLovely Professional University: Term Paper of Advanced Microbiology27AlokKumarОценок пока нет
- TetanusДокумент12 страницTetanustinkerbell03Оценок пока нет
- Tetanus: BackgroundДокумент19 страницTetanus: BackgroundYovita Devi KornelinОценок пока нет
- Tetanus: HistoryДокумент15 страницTetanus: HistorydanielleОценок пока нет
- Tetanus: Surgery Lecture OnДокумент23 страницыTetanus: Surgery Lecture OnJasonWalkerОценок пока нет
- Titration of High Dose Sedation Is Effective inДокумент16 страницTitration of High Dose Sedation Is Effective inchandra ristiadiОценок пока нет
- Tetanus-Dr. A.M IyagbaДокумент32 страницыTetanus-Dr. A.M IyagbaDr. Amb. Monday ZaccheausОценок пока нет
- TetanusДокумент47 страницTetanusSyamsul Arifin100% (3)
- Status InternusДокумент12 страницStatus InternusPriscaОценок пока нет
- Uncommon Progressive Systemic Tetanus A CaseДокумент7 страницUncommon Progressive Systemic Tetanus A Casepedro.romagnoliОценок пока нет
- TetanusДокумент23 страницыTetanusNadya Noor Mulya Putri100% (1)
- Meningitis, Tetanus, LeprosyДокумент39 страницMeningitis, Tetanus, LeprosyKhemz Dalde LimОценок пока нет
- TetanusДокумент31 страницаTetanusreresОценок пока нет
- Pa Tho GenesisДокумент11 страницPa Tho GenesisBeth AvelinoОценок пока нет
- New Trend Management TetanusДокумент0 страницNew Trend Management TetanuschayankkuОценок пока нет
- Current Management of TetanusДокумент11 страницCurrent Management of TetanusRajiv100% (8)
- Tetanus in The Intensive Care UnitДокумент125 страницTetanus in The Intensive Care UnitechadrОценок пока нет
- Snake Bites NotesДокумент22 страницыSnake Bites NotesgosegomangОценок пока нет
- TetanusДокумент35 страницTetanusWaNda GrОценок пока нет
- Tetanus Pathophysiology, Clinical Signs, DiagnosisДокумент9 страницTetanus Pathophysiology, Clinical Signs, DiagnosisJuris Isaac Perez VianaОценок пока нет
- Brucellosis: The Short Textbook of PediatricsДокумент3 страницыBrucellosis: The Short Textbook of PediatricsHosny M IsseОценок пока нет
- Carpal Tunnel Syndrome, A Simple Guide To The Condition, Treatment And Related ConditionsОт EverandCarpal Tunnel Syndrome, A Simple Guide To The Condition, Treatment And Related ConditionsРейтинг: 5 из 5 звезд5/5 (1)
- Anticipatory Guidance Newborn 2 MonthsДокумент4 страницыAnticipatory Guidance Newborn 2 MonthsLenard BangugОценок пока нет
- Divine Intervention Step 2CK Podcasts Notes - Read Only FileДокумент533 страницыDivine Intervention Step 2CK Podcasts Notes - Read Only FileKakha100% (5)
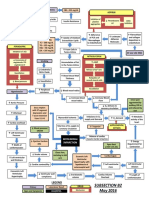
- B2 Concept Map - FinalДокумент1 страницаB2 Concept Map - FinalLenard BangugОценок пока нет
- 16 - Venous ThromboembolismДокумент2 страницы16 - Venous ThromboembolismLenard BangugОценок пока нет
- Visceral Pain Somatic Pain Referred Pain: 9. Acute AbdomenДокумент4 страницыVisceral Pain Somatic Pain Referred Pain: 9. Acute AbdomenLenard BangugОценок пока нет
- 25 - RabiesДокумент2 страницы25 - RabiesLenard BangugОценок пока нет
- Step 1 Study Strategies 2015-2 PDFДокумент13 страницStep 1 Study Strategies 2015-2 PDFLenard BangugОценок пока нет
- Script JPДокумент1 страницаScript JPLenard BangugОценок пока нет
- 21 - Adrenal CrisisДокумент5 страниц21 - Adrenal CrisisLenard BangugОценок пока нет
- GuideДокумент5 страницGuideLenard BangugОценок пока нет
- Cannot Stand Alone, Pulls To Stand, Indiscriminate Papa and Mama, Gesture Language, Discriminate Papa and Mama, Speak Few WordsДокумент1 страницаCannot Stand Alone, Pulls To Stand, Indiscriminate Papa and Mama, Gesture Language, Discriminate Papa and Mama, Speak Few WordsLenard BangugОценок пока нет
- Path To 250 Webinar v3Документ34 страницыPath To 250 Webinar v3Lenard BangugОценок пока нет
- Study Timeline Usmle Step1 PDGДокумент1 страницаStudy Timeline Usmle Step1 PDGLenard BangugОценок пока нет
- Study Timeline Usmle Step1 PDGДокумент1 страницаStudy Timeline Usmle Step1 PDGLenard BangugОценок пока нет
- Picmonic Step 1 Study PlanДокумент32 страницыPicmonic Step 1 Study PlanrammyttaОценок пока нет
- Connections Issue 11Документ21 страницаConnections Issue 11Victoria University, Melbourne, AustraliaОценок пока нет
- Jamie's Story 15q21.3-22.2 DeletionДокумент1 страницаJamie's Story 15q21.3-22.2 DeletionNatasha RadcliffeОценок пока нет
- PLLДокумент24 страницыPLLjagannnathdОценок пока нет
- LAS10 Week 4 7 2nd QuarterДокумент4 страницыLAS10 Week 4 7 2nd QuarterGleamor DaagОценок пока нет
- InterbarkadaДокумент8 страницInterbarkadaJay Vincent DiamanteОценок пока нет
- What Does A QHSE Engineer or Safety Officer Job Description Include?Документ2 страницыWhat Does A QHSE Engineer or Safety Officer Job Description Include?Sohail Ayub ButtОценок пока нет
- Tuskegee ExperimentДокумент2 страницыTuskegee ExperimentAniya LewisОценок пока нет
- Course 1.2: What You Should KnowДокумент27 страницCourse 1.2: What You Should KnowGeorgios MilitsisОценок пока нет
- Pediatric TransfusionДокумент82 страницыPediatric TransfusionMia Lesaca-Medina100% (2)
- Mediclaim 2009 AutumnДокумент46 страницMediclaim 2009 AutumngopalpaulОценок пока нет
- Plazma Ionizarot CP 212 Eng ManualДокумент1 страницаPlazma Ionizarot CP 212 Eng ManualVladimirDulaОценок пока нет
- BinderДокумент13 страницBinderisabel carreauОценок пока нет
- Is Iso 10555 1 1995Документ21 страницаIs Iso 10555 1 1995Hemant SharmaОценок пока нет
- Tiger Paint Remover SDSДокумент10 страницTiger Paint Remover SDSBernard YongОценок пока нет
- Fundamentals of Nursing Part 1Документ8 страницFundamentals of Nursing Part 1Evergreen Verds100% (1)
- Civil Engineering & Its BranchesДокумент37 страницCivil Engineering & Its BranchesMohammad JavedОценок пока нет
- Shofa Aji Setyoko (N101 12 051)Документ4 страницыShofa Aji Setyoko (N101 12 051)ShofaajiОценок пока нет
- Nutrilite Reset 30 Program GuideДокумент14 страницNutrilite Reset 30 Program GuideRoseОценок пока нет
- SP - Sindy MilaДокумент2 страницыSP - Sindy MilaSindy MelindaОценок пока нет
- Economics Assignment (AP)Документ20 страницEconomics Assignment (AP)Hemanth YenniОценок пока нет
- Bulletin 201215 (HTML Edition)Документ128 страницBulletin 201215 (HTML Edition)DonnieОценок пока нет
- BingggДокумент12 страницBingggZulham YahyaОценок пока нет
- Mh25 Borderline Personality GuidelineДокумент182 страницыMh25 Borderline Personality GuidelineAbdul Hakim Abdul KadirОценок пока нет
- Monkeypox: VirusДокумент18 страницMonkeypox: Virusdiela dwi lestariОценок пока нет
- Common Causes of Paediatric Alopecia: EpidemiologyДокумент5 страницCommon Causes of Paediatric Alopecia: EpidemiologyLiya SuwarniОценок пока нет
- New Form 6 Leave Form TEACHERSДокумент2 страницыNew Form 6 Leave Form TEACHERSmarites mercedОценок пока нет
- Master Form JSAДокумент2 страницыMaster Form JSAAgung PrasetyooОценок пока нет
- Test I. True or False. Write TRUE If The Statement Is Correct and FALSE If The Statement Is IncorrectДокумент2 страницыTest I. True or False. Write TRUE If The Statement Is Correct and FALSE If The Statement Is IncorrectMariecris Barayuga Duldulao-AbelaОценок пока нет
- Qi - Magazine Nº48Документ41 страницаQi - Magazine Nº48Carvalho100% (4)
- GayДокумент15 страницGayjulyerwanni100% (2)