Вам также может понравиться
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- Score:: Division of Taguig City and Pateros Diosdado Macapagal High School Unit Test Mapeh Grade 8Документ5 страницScore:: Division of Taguig City and Pateros Diosdado Macapagal High School Unit Test Mapeh Grade 8NinoОценок пока нет
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (399)
- The Game of Basketball Was Created December of 1891 by YMC Gym Teacher JAMES NAISMITH in SpringfieldДокумент2 страницыThe Game of Basketball Was Created December of 1891 by YMC Gym Teacher JAMES NAISMITH in SpringfieldJohnlord MangilaОценок пока нет
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Korean cagers clamp down on defenseДокумент53 страницыKorean cagers clamp down on defenseNymfa Balubar GacoОценок пока нет
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (894)
- Five Values Create Cornerstone of Tide's SuccessДокумент5 страницFive Values Create Cornerstone of Tide's Successjenkins4100% (1)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- Photocopiables (Smart Planet 1)Документ21 страницаPhotocopiables (Smart Planet 1)AlbaGP83Оценок пока нет
- Exercises Unit 3 4 5 and 6 AnswersДокумент3 страницыExercises Unit 3 4 5 and 6 AnswerscuauhtemocОценок пока нет
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
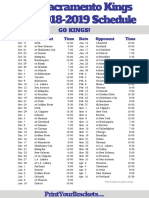
- Sacramento Kings 2018-19 Schedule GuideДокумент1 страницаSacramento Kings 2018-19 Schedule GuideMelchor BalolongОценок пока нет
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- 50+ Contoh Soal Latihan UN Dan UNBK Bahasa iNGGRIS SMK Paket BДокумент17 страниц50+ Contoh Soal Latihan UN Dan UNBK Bahasa iNGGRIS SMK Paket Bregina lampita sihombingОценок пока нет
- Final Archery Unit PlanДокумент32 страницыFinal Archery Unit Planapi-391472390Оценок пока нет
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (265)
- Achievement Test First SemesterДокумент3 страницыAchievement Test First SemestergretchelleОценок пока нет
- Sports Writing: Discussant: Maria Ariza C. RoqueДокумент30 страницSports Writing: Discussant: Maria Ariza C. RoqueMaria Ariza RoqueОценок пока нет
- Quick LinksДокумент63 страницыQuick LinksRodrigo Silva100% (1)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- Introduction to Philippine SportsДокумент19 страницIntroduction to Philippine Sportshee jakeuОценок пока нет
- 2017 NBA Manifesto - Mark DeeksДокумент340 страниц2017 NBA Manifesto - Mark DeeksEric Sidewater100% (1)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (344)
- Sportsfest ProposalДокумент5 страницSportsfest ProposalErica Dizon100% (5)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- Ped 201 Lab 3 Fall 2014Документ6 страницPed 201 Lab 3 Fall 2014api-272755646Оценок пока нет
- Hillcrest Indians (Fayetteville, Arkansas) 1961-62 Championship Basketball SeasonДокумент19 страницHillcrest Indians (Fayetteville, Arkansas) 1961-62 Championship Basketball SeasonDanWDurningОценок пока нет
- NBA 2K13 Playbook and SlidersДокумент241 страницаNBA 2K13 Playbook and SlidersMinn21tОценок пока нет
- Marilyn D. Mintz Created Her One of A Kind Art Prints: "The Art of Sports," With Poetry, Song and Art Print Calendar IncludedДокумент2 страницыMarilyn D. Mintz Created Her One of A Kind Art Prints: "The Art of Sports," With Poetry, Song and Art Print Calendar IncludedPR.comОценок пока нет
- 1v1 Dribbling and FinishingДокумент33 страницы1v1 Dribbling and FinishingJerson Daniel Alcaraz Uliambre100% (3)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- HIST303 Assessment 9Документ4 страницыHIST303 Assessment 9Kirana Rista PutriОценок пока нет
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2219)
- CCC Fall2010 LowresДокумент24 страницыCCC Fall2010 LowresfrontporОценок пока нет
- Rogerian EssayДокумент6 страницRogerian Essayapi-531381217Оценок пока нет
- Signed Off - Pe8 - q1 - Mod4 - Introductiontoteamsports - v2Документ29 страницSigned Off - Pe8 - q1 - Mod4 - Introductiontoteamsports - v2April Pearl CapiliОценок пока нет
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- Grade 11 HPE ExamДокумент3 страницыGrade 11 HPE ExamMiftah seidОценок пока нет
- Aecom Buffalo Site Opt Study - FINAL-141223Документ141 страницаAecom Buffalo Site Opt Study - FINAL-141223Mark Booker100% (1)
- Soccer Steps To SuccessДокумент272 страницыSoccer Steps To Successandyvtran100% (1)
- Mail : TaruhanДокумент1 страницаMail : Taruhanwira putraОценок пока нет
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (119)
- Optik Channel SelectionДокумент4 страницыOptik Channel SelectionDknightRTОценок пока нет
- Landscape Arch PPT 4 AssДокумент15 страницLandscape Arch PPT 4 AssJasbeer SharmaОценок пока нет