Вам также может понравиться
- Ncma 113Документ4 страницыNcma 113Wonie booОценок пока нет
- Chapter 15: Respiratory System MC 1Документ6 страницChapter 15: Respiratory System MC 1guadalupedeamargaretОценок пока нет
- Respiratory SystemДокумент8 страницRespiratory SystemDeeza Joice CastañedaОценок пока нет
- Breathing and Exchange of GasesДокумент41 страницаBreathing and Exchange of Gases538 varsha vishnoiОценок пока нет
- Ca - MS (Respiratory)Документ4 страницыCa - MS (Respiratory)kyleОценок пока нет
- OXYGENATIONДокумент8 страницOXYGENATIONJo Marchianne Pigar0% (1)
- Nayli Bio SBP 2019 EseiДокумент5 страницNayli Bio SBP 2019 EseiEqis AlfiesyaОценок пока нет
- Breathing and Exchange of GasesДокумент3 страницыBreathing and Exchange of GasesChirag RajpalОценок пока нет
- Ncma113 Lec Lab FinalДокумент24 страницыNcma113 Lec Lab FinalJulla GalangОценок пока нет
- Lung Diseases: Obstructive Airway Disease Restrictive Airway DiseasesДокумент49 страницLung Diseases: Obstructive Airway Disease Restrictive Airway Diseasesq2ndzg5rjxОценок пока нет
- Breathing and Exchange of GasesДокумент43 страницыBreathing and Exchange of GasesChinmaya SОценок пока нет
- NCM 112 Lecture Notes (Respiratory System and Its Diseases)Документ9 страницNCM 112 Lecture Notes (Respiratory System and Its Diseases)Kyle FernandezОценок пока нет
- Pulmnonary SystemДокумент13 страницPulmnonary Systemnatalie muyengwaОценок пока нет
- Respiratory System TransesДокумент5 страницRespiratory System Transesadrielvamos28Оценок пока нет
- Poe 4Документ5 страницPoe 4martinrestrepobateroОценок пока нет
- WK4 - OxygenationДокумент3 страницыWK4 - Oxygenationbstudent136Оценок пока нет
- A&P Chapter 15 Respiratory SystemДокумент21 страницаA&P Chapter 15 Respiratory SystemKarl RobleОценок пока нет
- MTPX Care SemiДокумент7 страницMTPX Care SemirusselpageОценок пока нет
- Chapter 20 OxygenationДокумент31 страницаChapter 20 OxygenationHannah Lat VillavicencioОценок пока нет
- CAOLBOY Module 15 Activity Worksheet On Respiratory SystemДокумент10 страницCAOLBOY Module 15 Activity Worksheet On Respiratory SystemAnton LeoncitoОценок пока нет
- Respiratory PhysiologyДокумент16 страницRespiratory PhysiologyYsabel Salvador DychincoОценок пока нет
- Pulmonary PhysioДокумент52 страницыPulmonary PhysiodjokerОценок пока нет
- Anatomy Final pt.2Документ8 страницAnatomy Final pt.2Gladys Mae S. BañesОценок пока нет
- RESPIRATORY SYSTEM Post LabДокумент3 страницыRESPIRATORY SYSTEM Post LabVeronica AsuncionОценок пока нет
- Anaphy ReviewerДокумент16 страницAnaphy ReviewerPauleen FejeОценок пока нет
- Respiratory PhysiologyДокумент55 страницRespiratory PhysiologyANDRES GUARDIA CAYOОценок пока нет
- Anaphy Lab ReviewerДокумент12 страницAnaphy Lab ReviewerCamille ParedesОценок пока нет
- Respiratory SystemДокумент3 страницыRespiratory SystemCookies AndcreamОценок пока нет
- Respiratory System 1Документ33 страницыRespiratory System 1Arianne Jen Genotiva100% (1)
- QDQDQDQDQDQWQDДокумент17 страницQDQDQDQDQDQWQDTL GianОценок пока нет
- Allows You To Talk and Make Sounds When Air Moves in and OutДокумент3 страницыAllows You To Talk and Make Sounds When Air Moves in and OutchelliОценок пока нет
- EXTRA NotesДокумент26 страницEXTRA NotesAhmad HasanОценок пока нет
- zpms1207 Respiratory-SystemДокумент4 страницыzpms1207 Respiratory-Systemamysong772Оценок пока нет
- Finals Quiz 1 TransДокумент14 страницFinals Quiz 1 Transjade jaymeОценок пока нет
- Resp Yamashita Ventilation NotesДокумент9 страницResp Yamashita Ventilation Notes1233211qwerasdОценок пока нет
- Giu 2986 62 16130 2024-02-22T14 46 59Документ18 страницGiu 2986 62 16130 2024-02-22T14 46 59amoraaloushОценок пока нет
- Responses To Altered Respiratory FunctionДокумент19 страницResponses To Altered Respiratory FunctionKoleen KirstenОценок пока нет
- MEDSRUG Respiratory System NotesДокумент6 страницMEDSRUG Respiratory System NotesMichaela Katrice MacabangunОценок пока нет
- Med SurgДокумент3 страницыMed SurgShaira Mae GordoraОценок пока нет
- 2.1 Respiratory SystemДокумент2 страницы2.1 Respiratory Systemsmart guysОценок пока нет
- Respiratory Physiology PostedДокумент25 страницRespiratory Physiology PostedYeni PuspitaОценок пока нет
- Apec Schools 1 Quarter S.Y. 2019 - 2020 Science 9 Lesson Handout #3: Coordinated Function - The Human Respiratory SystemДокумент2 страницыApec Schools 1 Quarter S.Y. 2019 - 2020 Science 9 Lesson Handout #3: Coordinated Function - The Human Respiratory SystemEy ChuaОценок пока нет
- Respiratory System To Be ContinueДокумент5 страницRespiratory System To Be ContinueRose Ann CammagayОценок пока нет
- Ncma113-Respiratory and Nursing CareДокумент5 страницNcma113-Respiratory and Nursing Careroldanmarygrace023Оценок пока нет
- Week 27-COPD PDFДокумент2 страницыWeek 27-COPD PDFJaimie Charlotte Marie LangilleОценок пока нет
- Breathing and Exchange of GasesДокумент5 страницBreathing and Exchange of Gaseslpc4944Оценок пока нет
- Respiratory SystemДокумент72 страницыRespiratory SystemElaine Victoria ElizanОценок пока нет
- Practical PhysiologyДокумент14 страницPractical PhysiologyOmar AymanОценок пока нет
- Ventilatory Assistance Study GuideДокумент9 страницVentilatory Assistance Study GuideBrianna RorickОценок пока нет
- Respiratory System: Dr. Agung Kurniawan, MkesДокумент31 страницаRespiratory System: Dr. Agung Kurniawan, MkesJojo BodhoОценок пока нет
- L1 2 PDFДокумент32 страницыL1 2 PDFMiles HuiОценок пока нет
- The Respiratory SystemДокумент61 страницаThe Respiratory SystemLuna JadeОценок пока нет
- ACFrOgC7mxGaX9liXL4MXhyIib2My7OJ2fZppJtUXaiwHAXPWv6byWDD3pHlmU1oEOp6KBWon7YU jkOlWtd JuFuLgT1S2gy3uqt5qGGQC - XMeRzHD ILMtafpI6OCKEmRORkbnWIkeZVIfnbmДокумент22 страницыACFrOgC7mxGaX9liXL4MXhyIib2My7OJ2fZppJtUXaiwHAXPWv6byWDD3pHlmU1oEOp6KBWon7YU jkOlWtd JuFuLgT1S2gy3uqt5qGGQC - XMeRzHD ILMtafpI6OCKEmRORkbnWIkeZVIfnbmCenitserОценок пока нет
- Introduction To Respiratory System-2020Документ27 страницIntroduction To Respiratory System-2020Izlan AidilОценок пока нет
- L - 2 Physiology of Respiration IIДокумент25 страницL - 2 Physiology of Respiration IIkaukab azimОценок пока нет
- 04 OxygenationДокумент4 страницы04 Oxygenationbunso padillaОценок пока нет
- Respiratory Phisiology: Dr. Haryo PrabowoДокумент60 страницRespiratory Phisiology: Dr. Haryo Praboworahmat feryadiОценок пока нет
- Week 11 Anph 111Документ6 страницWeek 11 Anph 111itsmearonsupanОценок пока нет
- MODULE 22 HANDOUTS Repiratory SystemДокумент3 страницыMODULE 22 HANDOUTS Repiratory SystemMichaela PoОценок пока нет
- Pathophysiology of CushingДокумент3 страницыPathophysiology of CushingAj MacotoОценок пока нет
- Wound Care and Wound DressingДокумент46 страницWound Care and Wound DressingAj Macoto50% (2)
- Nursing Care PlanДокумент1 страницаNursing Care PlanAj MacotoОценок пока нет
- NCP InsomniaДокумент2 страницыNCP InsomniaAj MacotoОценок пока нет
- Nursing Care For A High Risk NewbornДокумент16 страницNursing Care For A High Risk NewbornAj MacotoОценок пока нет
- Intervention Plan Evaluation Nursing Interventions Method of Nurse Family Contact Resources RequiredДокумент1 страницаIntervention Plan Evaluation Nursing Interventions Method of Nurse Family Contact Resources RequiredAj MacotoОценок пока нет
- Scale For Ranking Health ConditionsДокумент3 страницыScale For Ranking Health ConditionsAj MacotoОценок пока нет
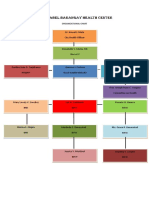
- Org ChartДокумент1 страницаOrg ChartAj MacotoОценок пока нет
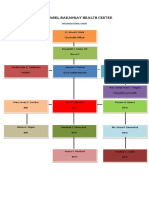
- Org ChartДокумент1 страницаOrg ChartAj MacotoОценок пока нет
- ECOMAPДокумент1 страницаECOMAPAj MacotoОценок пока нет
- CASE STUDY PEDIA - SaavedraДокумент15 страницCASE STUDY PEDIA - SaavedraChryst Louise SaavedraОценок пока нет
- Recommendations For Rescue of A Submerged Unresponsive Compressed-Gas DiverДокумент10 страницRecommendations For Rescue of A Submerged Unresponsive Compressed-Gas Diverwyma01Оценок пока нет
- GI Bleeding in Patients Receiving Antiplatelets and Anticoagulant TherapyДокумент11 страницGI Bleeding in Patients Receiving Antiplatelets and Anticoagulant TherapyTony LeeОценок пока нет
- Identification of High Risk PregnanciesДокумент15 страницIdentification of High Risk PregnanciesVidya Ganesh100% (12)
- Pharmacology of Drugs For PPHДокумент55 страницPharmacology of Drugs For PPHFaye CagayanОценок пока нет
- Australian Biology Olympiad 2009Документ41 страницаAustralian Biology Olympiad 2009Science Olympiad Blog100% (1)
- Cyriax HandoutДокумент43 страницыCyriax HandoutMeenakshiputraeashwarprasad MacherlaОценок пока нет
- Jewish Genetic DiseasesДокумент2 страницыJewish Genetic DiseasesReformJudaismОценок пока нет
- Sterile Parenteral Products: A Narrative Approach: Journal of Drug Delivery and TherapeuticsДокумент8 страницSterile Parenteral Products: A Narrative Approach: Journal of Drug Delivery and TherapeuticsArinta Purwi SuhartiОценок пока нет
- Grade 8 Health Summative Test Alcohol and CigaretteДокумент3 страницыGrade 8 Health Summative Test Alcohol and CigaretteAlbert Ian Casuga100% (1)
- Positive and Negative Filipino ValuesДокумент2 страницыPositive and Negative Filipino ValuesBrenty TablateОценок пока нет
- CDF NAC ProtocolДокумент247 страницCDF NAC ProtocolFrorefare LarcenerОценок пока нет
- Anchor Speech On WorkshopДокумент6 страницAnchor Speech On WorkshopPabhat Kumar100% (2)
- Rheumatology: With Kartik Rangaraj MDДокумент39 страницRheumatology: With Kartik Rangaraj MDNailahRahmahОценок пока нет
- DS - Aseptoman® Plus - Pif - en - 1711Документ2 страницыDS - Aseptoman® Plus - Pif - en - 1711Serbanica RazvanОценок пока нет
- Graves DiseaseДокумент13 страницGraves DiseaseGerald John PazОценок пока нет
- Answer: 1Документ4 страницыAnswer: 1Jeffrey ViernesОценок пока нет
- Systematic Review Pelaksanaan Programmatic Management of Drug-Resistant Tuberculosis Pada Pasien Tuberkulosis Resistan ObatДокумент8 страницSystematic Review Pelaksanaan Programmatic Management of Drug-Resistant Tuberculosis Pada Pasien Tuberkulosis Resistan ObatAdinda Pramesthi RiadyaniОценок пока нет
- MRCPCH q15Документ30 страницMRCPCH q15Galaleldin AliОценок пока нет
- (NH4) 2co3Документ5 страниц(NH4) 2co3MuhafiОценок пока нет
- RLE Module 2M - Chest Physiotherapy, Postural Drainage, Nebulization, Chest Tube Drainage Systems, Blood TransfusionДокумент57 страницRLE Module 2M - Chest Physiotherapy, Postural Drainage, Nebulization, Chest Tube Drainage Systems, Blood TransfusionAlexa GoteraОценок пока нет
- ChickenpoxДокумент5 страницChickenpoxShan MunozОценок пока нет
- CM2-CU10-Modification of Mendelian RatiosДокумент17 страницCM2-CU10-Modification of Mendelian RatiosClaire GonoОценок пока нет
- Pollution SlidesДокумент5 страницPollution Slidessaba_786Оценок пока нет
- Cells - 1 V2 (Euks, Proks & Viruses)Документ9 страницCells - 1 V2 (Euks, Proks & Viruses)mormerodОценок пока нет
- Ludwig's AnginaДокумент22 страницыLudwig's AnginaDevavrat SinghОценок пока нет
- Caring For Injured Reptiles2004Документ40 страницCaring For Injured Reptiles2004SujayJainОценок пока нет
- Circulatory System Review WorksheetДокумент2 страницыCirculatory System Review WorksheetCatherine JacksonОценок пока нет
- Journal of Clinical and Diagnostic ResearchДокумент5 страницJournal of Clinical and Diagnostic ResearchBoedyОценок пока нет
- Lucid Dreaming Tips OWДокумент9 страницLucid Dreaming Tips OWarlikОценок пока нет
- Instant Loss On a Budget: Super-Affordable Recipes for the Health-Conscious CookОт EverandInstant Loss On a Budget: Super-Affordable Recipes for the Health-Conscious CookРейтинг: 3.5 из 5 звезд3.5/5 (2)
- Glucose Revolution: The Life-Changing Power of Balancing Your Blood SugarОт EverandGlucose Revolution: The Life-Changing Power of Balancing Your Blood SugarРейтинг: 5 из 5 звезд5/5 (351)
- The Beck Diet Solution Weight Loss Workbook: The 6-Week Plan to Train Your Brain to Think Like a Thin PersonОт EverandThe Beck Diet Solution Weight Loss Workbook: The 6-Week Plan to Train Your Brain to Think Like a Thin PersonРейтинг: 3.5 из 5 звезд3.5/5 (33)
- The End of Craving: Recovering the Lost Wisdom of Eating WellОт EverandThe End of Craving: Recovering the Lost Wisdom of Eating WellРейтинг: 4.5 из 5 звезд4.5/5 (82)
- The Diabetes Code: Prevent and Reverse Type 2 Diabetes NaturallyОт EverandThe Diabetes Code: Prevent and Reverse Type 2 Diabetes NaturallyРейтинг: 4.5 из 5 звезд4.5/5 (3)
- The Arm: Inside the Billion-Dollar Mystery of the Most Valuable Commodity in SportsОт EverandThe Arm: Inside the Billion-Dollar Mystery of the Most Valuable Commodity in SportsРейтинг: 4 из 5 звезд4/5 (49)
- Find Your Path: Honor Your Body, Fuel Your Soul, and Get Strong with the Fit52 LifeОт EverandFind Your Path: Honor Your Body, Fuel Your Soul, and Get Strong with the Fit52 LifeРейтинг: 4 из 5 звезд4/5 (3)
- Sugar Crush: How to Reduce Inflammation, Reverse Nerve Damage, and Reclaim Good HealthОт EverandSugar Crush: How to Reduce Inflammation, Reverse Nerve Damage, and Reclaim Good HealthРейтинг: 4 из 5 звезд4/5 (6)
- Metabolism Revolution: Lose 14 Pounds in 14 Days and Keep It Off for LifeОт EverandMetabolism Revolution: Lose 14 Pounds in 14 Days and Keep It Off for LifeОценок пока нет
- Body Love Every Day: Choose Your Life-Changing 21-Day Path to Food FreedomОт EverandBody Love Every Day: Choose Your Life-Changing 21-Day Path to Food FreedomРейтинг: 4 из 5 звезд4/5 (1)
- The Diet Trap Solution: Train Your Brain to Lose Weight and Keep It Off for GoodОт EverandThe Diet Trap Solution: Train Your Brain to Lose Weight and Keep It Off for GoodОценок пока нет
- Glucose Goddess Method: A 4-Week Guide to Cutting Cravings, Getting Your Energy Back, and Feeling AmazingОт EverandGlucose Goddess Method: A 4-Week Guide to Cutting Cravings, Getting Your Energy Back, and Feeling AmazingРейтинг: 5 из 5 звезд5/5 (61)
- Eat to Lose, Eat to Win: Your Grab-n-Go Action Plan for a Slimmer, Healthier YouОт EverandEat to Lose, Eat to Win: Your Grab-n-Go Action Plan for a Slimmer, Healthier YouОценок пока нет
- Grit & Grace: Train the Mind, Train the Body, Own Your LifeОт EverandGrit & Grace: Train the Mind, Train the Body, Own Your LifeРейтинг: 4 из 5 звезд4/5 (3)
- Ultrametabolism: The Simple Plan for Automatic Weight LossОт EverandUltrametabolism: The Simple Plan for Automatic Weight LossРейтинг: 4.5 из 5 звезд4.5/5 (28)
- The Body Book: The Law of Hunger, the Science of Strength, and Other Ways to Love Your Amazing BodyОт EverandThe Body Book: The Law of Hunger, the Science of Strength, and Other Ways to Love Your Amazing BodyОценок пока нет
- Hungry for Change: Ditch the Diets, Conquer the Cravings, and Eat Your Way to Lifelong HealthОт EverandHungry for Change: Ditch the Diets, Conquer the Cravings, and Eat Your Way to Lifelong HealthРейтинг: 4 из 5 звезд4/5 (7)
- The Food Lover's Cleanse: 140 Delicious, Nourishing Recipes That Will Tempt You Back into Healthful EatingОт EverandThe Food Lover's Cleanse: 140 Delicious, Nourishing Recipes That Will Tempt You Back into Healthful EatingРейтинг: 4 из 5 звезд4/5 (3)
- Foods That Cause You to Lose Weight: The Negative Calorie EffectОт EverandFoods That Cause You to Lose Weight: The Negative Calorie EffectРейтинг: 3 из 5 звезд3/5 (5)
- How to Be Well: The 6 Keys to a Happy and Healthy LifeОт EverandHow to Be Well: The 6 Keys to a Happy and Healthy LifeРейтинг: 5 из 5 звезд5/5 (1)
- Keto Friendly Recipes: Easy Keto For Busy PeopleОт EverandKeto Friendly Recipes: Easy Keto For Busy PeopleРейтинг: 3.5 из 5 звезд3.5/5 (2)
- Summary: Fast Like a Girl: A Woman’s Guide to Using the Healing Power of Fasting to Burn Fat, Boost Energy, and Balance Hormones: Key Takeaways, Summary and AnalysisОт EverandSummary: Fast Like a Girl: A Woman’s Guide to Using the Healing Power of Fasting to Burn Fat, Boost Energy, and Balance Hormones: Key Takeaways, Summary and AnalysisРейтинг: 3 из 5 звезд3/5 (2)
- Secrets From the Eating Lab: The Science of Weight Loss, the Myth of Willpower, and Why You Should Never Diet AgainОт EverandSecrets From the Eating Lab: The Science of Weight Loss, the Myth of Willpower, and Why You Should Never Diet AgainРейтинг: 3.5 из 5 звезд3.5/5 (38)
- The Candida Cure: The 90-Day Program to Balance Your Gut, Beat Candida, and Restore Vibrant HealthОт EverandThe Candida Cure: The 90-Day Program to Balance Your Gut, Beat Candida, and Restore Vibrant HealthОценок пока нет
- Summary of Mary Claire Haver's The Galveston DietОт EverandSummary of Mary Claire Haver's The Galveston DietРейтинг: 5 из 5 звезд5/5 (2)