Вам также может понравиться
- Vaccine Handbook Process Br5237en MKДокумент26 страницVaccine Handbook Process Br5237en MKhadeer100% (2)
- Hematology & Immune SystemДокумент81 страницаHematology & Immune SystemAmanuel Maru100% (1)
- Nip Mop Booklet 3Документ36 страницNip Mop Booklet 3Tin Timban Gamos100% (1)
- HPV Vaksin 11 Maret 2023 - Dr. Cindy Rani SpOG KFER PDFДокумент35 страницHPV Vaksin 11 Maret 2023 - Dr. Cindy Rani SpOG KFER PDFYuliyanahОценок пока нет
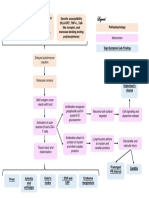
- Acute Ischemic Stroke Concept MapДокумент6 страницAcute Ischemic Stroke Concept MapMoonyeen Jann Casera Balic100% (2)
- Vaccines Science PharmaДокумент30 страницVaccines Science PharmaGanesh V GaonkarОценок пока нет
- VaccinationДокумент28 страницVaccinationM AQIB ASLAMОценок пока нет
- Active and Passive ImmunizationДокумент11 страницActive and Passive ImmunizationNgakanОценок пока нет
- Pulmonary Tuberculosis 2016Документ17 страницPulmonary Tuberculosis 2016Nikka Moreen Dagdag100% (1)
- Bacteriology HandoutДокумент30 страницBacteriology HandoutMoonyeen Jann Casera BalicОценок пока нет
- Principles of Epidemiology - Lesson 1 - Section 8Документ4 страницыPrinciples of Epidemiology - Lesson 1 - Section 8Faria bukhariОценок пока нет
- Vaccine Production (L1F17PHMD0174)Документ22 страницыVaccine Production (L1F17PHMD0174)Faizah Khalid100% (1)
- Immunitization and VaccinationДокумент46 страницImmunitization and VaccinationMazhar RehmanОценок пока нет
- Chapter 12 Basic ImmunologyДокумент39 страницChapter 12 Basic ImmunologyTofikОценок пока нет
- Imunizarea Si Vaccinologia: ImunitateaДокумент13 страницImunizarea Si Vaccinologia: ImunitateaLoredana CîrlanОценок пока нет
- ImmunizationДокумент28 страницImmunizationTusvendran Pillai100% (1)
- Antigen Body.: Classification VaccinesДокумент9 страницAntigen Body.: Classification VaccinesMohamed AlsaabОценок пока нет
- Split PDF 030224 7.37.42Документ11 страницSplit PDF 030224 7.37.42ayushi693shindeОценок пока нет
- VaccinationДокумент35 страницVaccinationmuneebazmat1123Оценок пока нет
- Immunotherapy and PreventionДокумент41 страницаImmunotherapy and PreventionCorina BoghiuОценок пока нет
- CHN 1 Immunization ProgramДокумент12 страницCHN 1 Immunization ProgramKyle VargasОценок пока нет
- Vaccines: Properties of Ideal VaccineДокумент5 страницVaccines: Properties of Ideal VaccinelujihaneОценок пока нет
- Lecture - Immunization and VaccinesДокумент40 страницLecture - Immunization and Vaccinesrockyrawat01012003Оценок пока нет
- L1 OcrДокумент12 страницL1 OcrMohamed AlsaabОценок пока нет
- Anti-Viral ChemotherapyДокумент39 страницAnti-Viral Chemotherapyjolan.freedomОценок пока нет
- Communicable Disease (Introduction Part 2) : Period of DeclineДокумент6 страницCommunicable Disease (Introduction Part 2) : Period of Declinefiel borataОценок пока нет
- Group 3 - ImmunizationДокумент74 страницыGroup 3 - ImmunizationNathanieGequilloОценок пока нет
- Adult ImmunizationДокумент48 страницAdult ImmunizationMangesh JadhavОценок пока нет
- Vaccine Cold Chain Aefi Immunization CardДокумент109 страницVaccine Cold Chain Aefi Immunization Carddhruv kathuriaОценок пока нет
- Social Pharmacy Practical 1Документ35 страницSocial Pharmacy Practical 1Devam VanjariОценок пока нет
- 20C. Vaccinology IIДокумент17 страниц20C. Vaccinology IIEssington BeloОценок пока нет
- 5.14 Immunoprophylaxis ImmunotherapyДокумент60 страниц5.14 Immunoprophylaxis ImmunotherapyAlberto MayorgaОценок пока нет
- MED2 2.01b - Adult ImmunizationДокумент11 страницMED2 2.01b - Adult ImmunizationJorem Paulo LabaoОценок пока нет
- Immunization and VaccinesДокумент21 страницаImmunization and VaccinesMaiga Ayub HusseinОценок пока нет
- ImmunizationДокумент61 страницаImmunizationBro CraftОценок пока нет
- VaccineДокумент12 страницVaccineNickОценок пока нет
- Community Health Nursing Doh Related Programs: Epi - Types of VaccinesДокумент32 страницыCommunity Health Nursing Doh Related Programs: Epi - Types of VaccinesAngelaОценок пока нет
- Principles of ImmunizationДокумент4 страницыPrinciples of ImmunizationDoc Prince CaballeroОценок пока нет
- Current Concepts of ImmunoprophylaxisДокумент31 страницаCurrent Concepts of ImmunoprophylaxisTina Ong SinagaОценок пока нет
- ImmunizationДокумент55 страницImmunizationHafsah ShoaibОценок пока нет
- VaccineДокумент14 страницVaccineAman HoodaОценок пока нет
- Vaccines & Its Types: Ms Saajida Sultaana MahusookДокумент16 страницVaccines & Its Types: Ms Saajida Sultaana MahusookGayathri deviОценок пока нет
- MMR ImmunizationДокумент43 страницыMMR ImmunizationkukuruziОценок пока нет
- Unit 11 ImmunizationДокумент45 страницUnit 11 ImmunizationBikash Kandel100% (1)
- Chapter 18 VaccinesДокумент29 страницChapter 18 Vaccineshusseinabdullahahmad99Оценок пока нет
- Vaccines.: Abdulkadir Mohamed Hussein Nymambura Peris Moureen JepleenДокумент36 страницVaccines.: Abdulkadir Mohamed Hussein Nymambura Peris Moureen Jepleenodhiambo samwelОценок пока нет
- Immunity & Principles of VaccinationДокумент27 страницImmunity & Principles of VaccinationAniruddha RoyОценок пока нет
- Community Health Nursing Doh Related Programs: Epi - Types of VaccinesДокумент32 страницыCommunity Health Nursing Doh Related Programs: Epi - Types of VaccinesAngelaОценок пока нет
- Immunity & Principles of VaccinationДокумент27 страницImmunity & Principles of VaccinationReynaldiSanjayaОценок пока нет
- Vaccine & Principle of ImmunizationДокумент23 страницыVaccine & Principle of ImmunizationSindhu Babu100% (1)
- Immunity EPIДокумент37 страницImmunity EPIluttomiayvonneОценок пока нет
- ImmunizationДокумент24 страницыImmunizationAhmed Azeez100% (1)
- ImD-Med L4 (Immunization)Документ33 страницыImD-Med L4 (Immunization)VancopОценок пока нет
- COVID-19 Vaccine - RBДокумент15 страницCOVID-19 Vaccine - RBRajОценок пока нет
- Vaccines and Immunization Summer 2020Документ48 страницVaccines and Immunization Summer 2020Gia LeОценок пока нет
- PertussisДокумент3 страницыPertussiscyrelleОценок пока нет
- IMMUNIZATIONДокумент35 страницIMMUNIZATIONAkshay H.Оценок пока нет
- AEFIДокумент35 страницAEFIMisha ModiОценок пока нет
- Rakib L3 VaccinesДокумент23 страницыRakib L3 VaccinesSadia Afrin OshinОценок пока нет
- Vaccina Tion: By: Group 4Документ77 страницVaccina Tion: By: Group 4Angela ReyesОценок пока нет
- The Expanded Program On Immunization (EPI)Документ54 страницыThe Expanded Program On Immunization (EPI)Edna Uneta RoblesОценок пока нет
- Immunoprophylaxis and Immunotherapy: Dr. Mejbah Uddin AhmedДокумент19 страницImmunoprophylaxis and Immunotherapy: Dr. Mejbah Uddin Ahmedapi-19969058Оценок пока нет
- MODULE 2: Types of Vaccine and Adverse ReactionsДокумент29 страницMODULE 2: Types of Vaccine and Adverse ReactionsnandaОценок пока нет
- BscNR20 - Topic 8 - VaccinesДокумент6 страницBscNR20 - Topic 8 - Vaccinesakoeljames8543Оценок пока нет
- Nature's Answer to Viral Threats: Understanding the Potency of Plant-Based AntiviralsОт EverandNature's Answer to Viral Threats: Understanding the Potency of Plant-Based AntiviralsОценок пока нет
- LeukemiasДокумент8 страницLeukemiasMoonyeen Jann Casera BalicОценок пока нет
- CPG Acute Infectious Diarrhea Pocket Guide v2Документ21 страницаCPG Acute Infectious Diarrhea Pocket Guide v2Moonyeen Jann Casera BalicОценок пока нет
- Pharmgkb Summary: Very Important Pharmacogene Information For Ugt1A1Документ7 страницPharmgkb Summary: Very Important Pharmacogene Information For Ugt1A1Moonyeen Jann Casera BalicОценок пока нет
- Acute Rheumatic Fever PathophysiologyДокумент1 страницаAcute Rheumatic Fever PathophysiologyMoonyeen Jann Casera BalicОценок пока нет
- Lupus Power Point Fact SheetДокумент21 страницаLupus Power Point Fact Sheetacmarcus89Оценок пока нет
- Case On Acute Rheumatoid ArthritisДокумент15 страницCase On Acute Rheumatoid ArthritisdeepakОценок пока нет
- VS TL - Protein - L1 29261 2303 3Документ7 страницVS TL - Protein - L1 29261 2303 3Hadi BitarОценок пока нет
- The Disinfection Methods Used For Cryptosporidium Parvum: By: Pinar EryuvaДокумент15 страницThe Disinfection Methods Used For Cryptosporidium Parvum: By: Pinar EryuvaSabina BojadžićОценок пока нет
- 2000 Microbiology MCQs With KeyДокумент100 страниц2000 Microbiology MCQs With KeyAbdurrahman ZahidОценок пока нет
- 0161212感染小核心 CellulitisДокумент47 страниц0161212感染小核心 Cellulitis馮宥忻Оценок пока нет
- BY: Moses Kazevu (BSC Human Biology)Документ40 страницBY: Moses Kazevu (BSC Human Biology)Moses Jr KazevuОценок пока нет
- Imunologi Infeksi VirusДокумент27 страницImunologi Infeksi VirusHendika Ariyo SОценок пока нет
- Antiprotozoal and Antihelminthic Drugs - HandoutДокумент21 страницаAntiprotozoal and Antihelminthic Drugs - HandoutdonzОценок пока нет
- Jurnal Difteri English PDFДокумент9 страницJurnal Difteri English PDFLisbet Anita SimamoraОценок пока нет
- Implications Pathogenesis: GingivalДокумент30 страницImplications Pathogenesis: GingivalI Gede MahardikaОценок пока нет
- Modul #3 - Student Activity Sheet - CUTANEOUS MYCOSESДокумент7 страницModul #3 - Student Activity Sheet - CUTANEOUS MYCOSESYlia MastarsОценок пока нет
- Immunisation Schedule Victoria-November 2021Документ6 страницImmunisation Schedule Victoria-November 2021Julie PanditОценок пока нет
- Enseval Examination of Bacterial Contamination in Blood Components Biomerieux PDFДокумент21 страницаEnseval Examination of Bacterial Contamination in Blood Components Biomerieux PDFCik KahadiОценок пока нет
- DR Meenakshi MDS Oral PathologyДокумент29 страницDR Meenakshi MDS Oral PathologyDr. Meenakshi SinghalОценок пока нет
- Pa Tho PhysiologyДокумент3 страницыPa Tho Physiologyaprilkow07Оценок пока нет
- Catalogue DengueElisaRangeДокумент6 страницCatalogue DengueElisaRangeedrinsneОценок пока нет
- MT - Maleria (1) Rupesh KumarДокумент12 страницMT - Maleria (1) Rupesh KumarTopeshwar TpkОценок пока нет
- Hamlet Act 3 Vocabulary Sheet PDFДокумент2 страницыHamlet Act 3 Vocabulary Sheet PDFLuisОценок пока нет
- Wuchereria Bancrofti, Brugia Malayi, Brugia TimoriДокумент3 страницыWuchereria Bancrofti, Brugia Malayi, Brugia TimoriJurel GaoatОценок пока нет
- AnaisДокумент272 страницыAnaisJean Gabriel V. Coutinho100% (2)
- TB Fact Sheet - TB STOP EnglishДокумент2 страницыTB Fact Sheet - TB STOP Englishmaria halogОценок пока нет
- Ecologic ModelДокумент2 страницыEcologic Modelchardy101Оценок пока нет
- Maklumat Vaksinasi: Vaccination DetailsДокумент1 страницаMaklumat Vaksinasi: Vaccination DetailsazlanОценок пока нет
- EUA NanoEntek Frend Ifu PDFДокумент15 страницEUA NanoEntek Frend Ifu PDFHandoko HalimОценок пока нет
- Treatment Approaches in MSДокумент15 страницTreatment Approaches in MSSnezana MihajlovicОценок пока нет