Вам также может понравиться
- Lipid Treatments in Cardiologic, Metabolic and Diabetics: From Guideline To Clinical PracticeДокумент65 страницLipid Treatments in Cardiologic, Metabolic and Diabetics: From Guideline To Clinical PracticeRoby KieranОценок пока нет
- Gender Difference in Coronary Events in Relation To Risk Factors in Japanese Hypercholesterolemic Patients Treated With Low-Dose SimvastatinДокумент5 страницGender Difference in Coronary Events in Relation To Risk Factors in Japanese Hypercholesterolemic Patients Treated With Low-Dose SimvastatinasfwegereОценок пока нет
- Secondary Prevention Slide Set: AHA Stroke Guideline 2006Документ42 страницыSecondary Prevention Slide Set: AHA Stroke Guideline 2006NEuRoLoGisT CoFFeeCuP100% (1)
- Cardio Metabolic Risk in DiabetesДокумент29 страницCardio Metabolic Risk in DiabetesoctoindradjajaОценок пока нет
- Metabolic Syndrome, Diabetes, and Cardiovascular Disease: Implications For Preventive CardiologyДокумент36 страницMetabolic Syndrome, Diabetes, and Cardiovascular Disease: Implications For Preventive CardiologyAlvianridersОценок пока нет
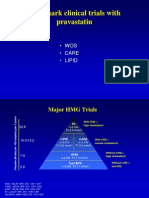
- Wos Care LipidДокумент55 страницWos Care LipidJuliana FeronОценок пока нет
- MRCP 2 Clinical Trial Data MRCP 2Документ5 страницMRCP 2 Clinical Trial Data MRCP 2Yong Fang YueОценок пока нет
- Cardiometabolic Syndrome: & DR Dhafir A. MahmoodДокумент62 страницыCardiometabolic Syndrome: & DR Dhafir A. MahmoodJacob AlphaОценок пока нет
- 27 FullДокумент6 страниц27 FullKrishna R KhanalОценок пока нет
- Sample Journal Club 1Документ2 страницыSample Journal Club 1aguocha1Оценок пока нет
- Dyslipidemia 2018Документ8 страницDyslipidemia 2018R JannahОценок пока нет
- Statins in CVD Management: Is Just Lipid Lowering Enough?Документ37 страницStatins in CVD Management: Is Just Lipid Lowering Enough?SriОценок пока нет
- Atorvastatin Statin in CVD ManagementДокумент37 страницAtorvastatin Statin in CVD ManagementSriОценок пока нет
- Raza2004 PDFДокумент12 страницRaza2004 PDFIvana RuseskaОценок пока нет
- Kuliah Dislipidemia UpdateДокумент44 страницыKuliah Dislipidemia UpdateYudy Hardiyansah100% (1)
- Metabolik SindromeДокумент46 страницMetabolik SindromePAn Lover'zОценок пока нет
- Atherosclerosis, Dyslipidaemia and Diabetes SlidesДокумент83 страницыAtherosclerosis, Dyslipidaemia and Diabetes SlidesWee DaliОценок пока нет
- New Treatments of Hypercholesterolemia: Jason A. Logan Family Medicine Clerkship Presentation 4/27/01Документ41 страницаNew Treatments of Hypercholesterolemia: Jason A. Logan Family Medicine Clerkship Presentation 4/27/01Saad MotawéaОценок пока нет
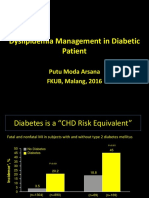
- Dyslipidemia Management in Diabetic Patient: Putu Moda Arsana FKUB, Malang, 2016Документ31 страницаDyslipidemia Management in Diabetic Patient: Putu Moda Arsana FKUB, Malang, 2016aprinaaaОценок пока нет
- JNC VIII Hypertension SaudiДокумент47 страницJNC VIII Hypertension SaudiDavid Chandra EriksonОценок пока нет
- Cerebrovscular DiseasesДокумент28 страницCerebrovscular DiseasesbagussofianОценок пока нет
- Lecture 25 - Plasma Ins 3 - 2006Документ31 страницаLecture 25 - Plasma Ins 3 - 2006api-3703352Оценок пока нет
- Dislipid 2 PDFДокумент4 страницыDislipid 2 PDFWahyuningsih HamidОценок пока нет
- Pattern of Dyslipidemia in Type Diabetic Subjects in Eastern NepalДокумент3 страницыPattern of Dyslipidemia in Type Diabetic Subjects in Eastern NepalDR VENKATARAMANA MurthyОценок пока нет
- Lopid: (Gemfibrozil Tablets, USP)Документ13 страницLopid: (Gemfibrozil Tablets, USP)Nisadiyah Faridatus ShahihОценок пока нет
- Lipid-Lowering Agents: Critical FactsДокумент22 страницыLipid-Lowering Agents: Critical Factsjyothi100% (1)
- Building A Diabetes Alliance: The Role of Provider EducationДокумент32 страницыBuilding A Diabetes Alliance: The Role of Provider EducationMark ReinhardtОценок пока нет
- Pharm 316 Case Presentation: Statins in The Golden Years - Statin For Primary Prevention in ElderlyДокумент37 страницPharm 316 Case Presentation: Statins in The Golden Years - Statin For Primary Prevention in ElderlyKevin JiaОценок пока нет
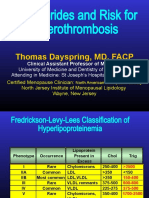
- Triglycerides and Risk For Atherothrombosis: Thomas Dayspring, MD, FACPДокумент92 страницыTriglycerides and Risk For Atherothrombosis: Thomas Dayspring, MD, FACPيونس حسينОценок пока нет
- TX LipidosДокумент14 страницTX Lipidosxander trujilloОценок пока нет
- Efficacy and Safety of High-Density Lipoprotein Cholesterol-Increasing CompoundsДокумент13 страницEfficacy and Safety of High-Density Lipoprotein Cholesterol-Increasing CompoundsAdityasekar WangiОценок пока нет
- Liberal Vs Tight Glycemic ControlДокумент41 страницаLiberal Vs Tight Glycemic ControlShihan HuqОценок пока нет
- Aztor Cme NewДокумент59 страницAztor Cme NewSheikh Sharfuddin RajeevОценок пока нет
- EMPA KIDNEY SGLT2 and Meta Analysis FINALДокумент1 страницаEMPA KIDNEY SGLT2 and Meta Analysis FINALThoraya AhmedОценок пока нет
- DyslipidemiaДокумент53 страницыDyslipidemiaRey AlwiwikhОценок пока нет
- CvotДокумент29 страницCvotakash kondapalliОценок пока нет
- Acute Myocard Ial Infarction in Young AdultДокумент57 страницAcute Myocard Ial Infarction in Young Adultshafiyah82Оценок пока нет
- Lipid Management in DMДокумент33 страницыLipid Management in DMSheung WongОценок пока нет
- Hypertension&Diabetes Mellitus: Fahmi Razi Darkuthni SMF Internal Medicine RSUD AmpanaДокумент54 страницыHypertension&Diabetes Mellitus: Fahmi Razi Darkuthni SMF Internal Medicine RSUD AmpanaadminabОценок пока нет
- Dyslipdiemia 2022Документ75 страницDyslipdiemia 2022LeeОценок пока нет
- Understanding The Needs of The High Productive DyslipidemiaДокумент47 страницUnderstanding The Needs of The High Productive DyslipidemiachchchchkОценок пока нет
- Stroke Topic DiscussionДокумент19 страницStroke Topic Discussionapi-648714317Оценок пока нет
- Diagnosis and Managment of Peripheral Artery Disease Gore Updated DR KrolickДокумент88 страницDiagnosis and Managment of Peripheral Artery Disease Gore Updated DR KrolickLeo OoОценок пока нет
- Prevalence of Dyslipidemia and Other Cardiovascular Risk Factors (Hypertension and Diabetes) in Medical ProfessionalsДокумент5 страницPrevalence of Dyslipidemia and Other Cardiovascular Risk Factors (Hypertension and Diabetes) in Medical ProfessionalsTirth NathwaniОценок пока нет
- Diagnosis and Managment of Peripheral Artery Disease Gore Updated DR KrolickДокумент88 страницDiagnosis and Managment of Peripheral Artery Disease Gore Updated DR KrolickLeo OoОценок пока нет
- Diamicron MRДокумент50 страницDiamicron MROmar Kamel Rayyan33% (3)
- Can The Ketogenic Diet Favorably Modify Cardiovascular Disease Risk Factors?Документ27 страницCan The Ketogenic Diet Favorably Modify Cardiovascular Disease Risk Factors?Prav GrewalОценок пока нет
- Prevalence of Dyslipidemia in Patients With Acute Coronary Syndrome Admitted at Tertiary Care Hospital in Nepal: A Descriptive Cross-Sectional StudyДокумент10 страницPrevalence of Dyslipidemia in Patients With Acute Coronary Syndrome Admitted at Tertiary Care Hospital in Nepal: A Descriptive Cross-Sectional StudybilahalvirayuОценок пока нет
- Mbs127 Slide DislipidemiaДокумент45 страницMbs127 Slide DislipidemiaDaru KristiyonoОценок пока нет
- Triglyceride Profile in Dyslipidaemia of Type 2 Diabetes MellitusДокумент4 страницыTriglyceride Profile in Dyslipidaemia of Type 2 Diabetes MellitusTanveerОценок пока нет
- Jurnal 4 WordДокумент20 страницJurnal 4 WordSri MaryatiОценок пока нет
- Edit Virtual HR Managing Dyslipidemia in Special PopulationДокумент38 страницEdit Virtual HR Managing Dyslipidemia in Special PopulationIkmah FauzanОценок пока нет
- Empagliflozin in Prevention of Cardiovascular Disease Among Patients With Diabetes Mellitus Type 2Документ4 страницыEmpagliflozin in Prevention of Cardiovascular Disease Among Patients With Diabetes Mellitus Type 2tb9Оценок пока нет
- S 21 Trejtnar AntidyslipidemicsДокумент47 страницS 21 Trejtnar AntidyslipidemicsCarlo MaxiaОценок пока нет
- Slide Curriculum Diabetes and CardiologyДокумент52 страницыSlide Curriculum Diabetes and CardiologyNazmul Hasan MahmudОценок пока нет
- 3 - Statin Primary Secondary MelaДокумент57 страниц3 - Statin Primary Secondary MelaKurniadin YayanОценок пока нет
- New Developments in The Management of Dyslipidemia: Widjanarko. W MDДокумент62 страницыNew Developments in The Management of Dyslipidemia: Widjanarko. W MDyulanda fitrianaОценок пока нет
- Clinical Surgery Review 2023: For USMLE Step 2 CK and COMLEX-USA Level 2От EverandClinical Surgery Review 2023: For USMLE Step 2 CK and COMLEX-USA Level 2Оценок пока нет
- They Help in CholesterolДокумент82 страницыThey Help in CholesterolEileen del RosarioОценок пока нет
- Overcoming Heart FailureДокумент71 страницаOvercoming Heart FailureEileen del Rosario100% (1)
- Atlas of Dialysis Vascular Access: Tushar J. Vachharajani, MD, FASN, FACPДокумент75 страницAtlas of Dialysis Vascular Access: Tushar J. Vachharajani, MD, FASN, FACPEileen del RosarioОценок пока нет
- Hemodialysis in ChildrenДокумент5 страницHemodialysis in ChildrenEileen del RosarioОценок пока нет
- Cardiac Rehabilitation: Nurse Talking Tip SheetДокумент3 страницыCardiac Rehabilitation: Nurse Talking Tip SheetEileen del RosarioОценок пока нет
- Edema: Yu-Hong Jia, PH.D Pathophysiological Department Dalian Medical UniversityДокумент29 страницEdema: Yu-Hong Jia, PH.D Pathophysiological Department Dalian Medical UniversityEileen del RosarioОценок пока нет
- Nurse - Cardiac Rehab FinalДокумент3 страницыNurse - Cardiac Rehab FinalEileen del RosarioОценок пока нет
- Nutrition For Patients With Heart Failure.5Документ5 страницNutrition For Patients With Heart Failure.5Eileen del RosarioОценок пока нет
- Ucm 309068Документ61 страницаUcm 309068Eileen del RosarioОценок пока нет
- 2017 Esc PadДокумент60 страниц2017 Esc PadEileen del RosarioОценок пока нет
- Coronary AngiographyДокумент71 страницаCoronary AngiographyEileen del Rosario100% (2)
- 2016 ESC CV PreventionДокумент78 страниц2016 ESC CV PreventionEileen del RosarioОценок пока нет
- Cancer Treatments & Cardiovascular Toxicity 2016 (Position Paper)Документ34 страницыCancer Treatments & Cardiovascular Toxicity 2016 (Position Paper)RESCATEURОценок пока нет
- Artifacts and Pitfalls in Doppler VelocimetryДокумент39 страницArtifacts and Pitfalls in Doppler VelocimetryEileen del RosarioОценок пока нет
- 2.11.08 Aspiration PNA GabbardДокумент25 страниц2.11.08 Aspiration PNA GabbardEileen del RosarioОценок пока нет
- HeadachehelpsheetДокумент1 страницаHeadachehelpsheetapi-219567017Оценок пока нет
- Dietary Diversity Score and Associated Factors Among High School Adolescent Girls in Gurage Zone, Southwest EthiopiaДокумент5 страницDietary Diversity Score and Associated Factors Among High School Adolescent Girls in Gurage Zone, Southwest EthiopiaFadhila NurrahmaОценок пока нет
- Listening Sample Test 3 Question PaperДокумент5 страницListening Sample Test 3 Question PaperjeznerОценок пока нет
- Hydrocephalus: I Dewa Ketut Gede Herry Oka Pembimbing: Dr. Dr. I Wayan Niryana, Sp. BS (K)Документ40 страницHydrocephalus: I Dewa Ketut Gede Herry Oka Pembimbing: Dr. Dr. I Wayan Niryana, Sp. BS (K)Dewa Oka100% (1)
- NEEM As Mosquito ExpellantДокумент59 страницNEEM As Mosquito Expellantknixau100% (2)
- Lit Review FinalДокумент2 страницыLit Review Finalapi-294212644Оценок пока нет
- Laryngeal Amyloidosis: ReviewДокумент8 страницLaryngeal Amyloidosis: ReviewLuis De jesus SolanoОценок пока нет
- Hydrochloric Acid Solution 6.0M 333.00Документ2 страницыHydrochloric Acid Solution 6.0M 333.00AnonОценок пока нет
- 1 s2.0 S014067362300569X MainДокумент11 страниц1 s2.0 S014067362300569X MainAldo Amed Montaño SalinasОценок пока нет
- Diagnostic and Therapeutic Approaches To HepatocelДокумент5 страницDiagnostic and Therapeutic Approaches To HepatocelrahmaОценок пока нет
- Jurnal Reading PanumДокумент28 страницJurnal Reading PanumIdris MohammadОценок пока нет
- Toxicology Q-Bank Updated VersionДокумент18 страницToxicology Q-Bank Updated VersionAhmed Mohamed100% (1)
- Denali Individual Dental All Other States - AETNAДокумент10 страницDenali Individual Dental All Other States - AETNAJohn BerkowitzОценок пока нет
- SpedДокумент5 страницSpedJessica BrownОценок пока нет
- Biotech Bo SeriesДокумент2 страницыBiotech Bo SeriesArlinda Friyanti CallistaОценок пока нет
- Spinal Cord InjuryДокумент16 страницSpinal Cord Injuryjohnlester_jlf100% (2)
- Drug Calcu 2014Документ2 страницыDrug Calcu 2014Paul Anthony LoricaОценок пока нет
- Uroradiology Tutorial For Medical Students: Lesson 1: Ultrasound - Part 1 American Urological AssociationДокумент68 страницUroradiology Tutorial For Medical Students: Lesson 1: Ultrasound - Part 1 American Urological AssociationDavid CiempkaОценок пока нет
- MSDS 8420 - PMMДокумент7 страницMSDS 8420 - PMMRAZA MEHDIОценок пока нет
- FST 225Документ63 страницыFST 225Karthikeyan BalakrishnanОценок пока нет
- Brushing Technique: Development of ToothbrushesДокумент70 страницBrushing Technique: Development of Toothbrushesgauravparakh100% (2)
- Principles of SterilityДокумент25 страницPrinciples of SterilityjuliusromatolentinoОценок пока нет
- Sarao 2015Документ120 страницSarao 2015Francisco AcostaОценок пока нет
- Drug CardsДокумент4 страницыDrug CardsBrittany Lynn MyersОценок пока нет
- Kroll CV 26 March 2018Документ92 страницыKroll CV 26 March 2018wolf woodОценок пока нет
- 1 s2.0 S0883540320304605 MainДокумент4 страницы1 s2.0 S0883540320304605 MainSavОценок пока нет
- Urinary Tract InfectionДокумент64 страницыUrinary Tract Infectionmiguel mendezОценок пока нет
- Pro BioticsДокумент15 страницPro BioticsAnna MohОценок пока нет
- Eating Disorder RecoveryДокумент4 страницыEating Disorder RecoveryDevotedrecoveryОценок пока нет
- Running Head: As Good As It Gets: An Analysis 1Документ11 страницRunning Head: As Good As It Gets: An Analysis 1Yassi FernandezОценок пока нет