Вам также может понравиться
- Hyper-coagulation, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsОт EverandHyper-coagulation, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsОценок пока нет
- Ninja - Antianginal Drugs PDFДокумент2 страницыNinja - Antianginal Drugs PDFErica Hyeyeon LeeОценок пока нет
- Ninja - Anemias PDFДокумент1 страницаNinja - Anemias PDFErica Hyeyeon LeeОценок пока нет
- GI Drugs PDFДокумент6 страницGI Drugs PDFErica Hyeyeon Lee100% (1)
- Differentials For Finals: - Pleuritic Chest Pain - Pulmonary Embolism - Pneumothorax PneumoniaДокумент9 страницDifferentials For Finals: - Pleuritic Chest Pain - Pulmonary Embolism - Pneumothorax PneumoniaOlivia MoranОценок пока нет
- ECG Interpretations GoodДокумент104 страницыECG Interpretations GoodaymenОценок пока нет
- 0.5. ANS Quicksheet PDFДокумент1 страница0.5. ANS Quicksheet PDFErica Hyeyeon LeeОценок пока нет
- Heart FailureДокумент1 страницаHeart FailureTrisha VergaraОценок пока нет
- Internal Medicine #1Документ167 страницInternal Medicine #1Nikhil RayarakulaОценок пока нет
- Ninja - Antiarrhythmic Drugs PDFДокумент7 страницNinja - Antiarrhythmic Drugs PDFErica Hyeyeon Lee100% (1)
- Pharm Fall Cardiovascular Pharmacology Study Guide-106Документ47 страницPharm Fall Cardiovascular Pharmacology Study Guide-106sean liyanageОценок пока нет
- Renal Guide and Charts: AlbuminДокумент16 страницRenal Guide and Charts: AlbuminYaima JimenezОценок пока нет
- Sphere: These DiarrheaДокумент3 страницыSphere: These Diarrheamed testОценок пока нет
- Pharm Expansion 17 NDFДокумент1 страницаPharm Expansion 17 NDFNokz M. Raki-inОценок пока нет
- ANS DrugsДокумент2 страницыANS Drugsmed testОценок пока нет
- Acid BaseДокумент89 страницAcid BaseEdouinaОценок пока нет
- Https:Jetmapp - orbundsis.com:Einstein-freshair:Videos::102793DigitalDownload LabValues NurseInTheMaking 2pagesДокумент5 страницHttps:Jetmapp - orbundsis.com:Einstein-freshair:Videos::102793DigitalDownload LabValues NurseInTheMaking 2pagesamazonian005100% (1)
- Antibiotics Chart 1Документ7 страницAntibiotics Chart 1Vee MendОценок пока нет
- Spinal Cord CompressionДокумент4 страницыSpinal Cord Compressionian3yeung-2Оценок пока нет
- Electrolyte ImbalanceДокумент3 страницыElectrolyte ImbalancemewilkinОценок пока нет
- Ninja - Anti-Coagulants PDFДокумент3 страницыNinja - Anti-Coagulants PDFErica Hyeyeon Lee100% (1)
- Pain 2. Pallor Poikylothermia Parasthesia Pulselessness Factor V Leiden (Activated Protein C Resistance)Документ3 страницыPain 2. Pallor Poikylothermia Parasthesia Pulselessness Factor V Leiden (Activated Protein C Resistance)Ryan TurnerОценок пока нет
- CardionotesДокумент5 страницCardionotesNichole Coletta100% (1)
- CVPR Prototype Drugs TableДокумент27 страницCVPR Prototype Drugs TablethommyvaОценок пока нет
- Antihypotensive Drugs: Roger Joseph Ii Ramos Jecino, RN, M.DДокумент28 страницAntihypotensive Drugs: Roger Joseph Ii Ramos Jecino, RN, M.DFranz Earl Niño AlbesaОценок пока нет
- Ninja - Anti-HTN PDFДокумент6 страницNinja - Anti-HTN PDFErica Hyeyeon Lee100% (2)
- Amboss Hemolytic AnemiaДокумент16 страницAmboss Hemolytic AnemiaAhmed Ali100% (2)
- Labs Electrolyte ChartДокумент1 страницаLabs Electrolyte ChartmdcmepОценок пока нет
- Pharmacology Main DrugsДокумент14 страницPharmacology Main DrugsSabir KhanОценок пока нет
- Clinical KardexДокумент2 страницыClinical KardexJackie Frey100% (2)
- Antibiotics Chart 2Документ10 страницAntibiotics Chart 2Vee MendОценок пока нет
- Renal Chart 2Документ21 страницаRenal Chart 2fortheloveofmedicineОценок пока нет
- Electrolyte Imbalance Cause Signs and Symptoms Intervention ConnectionДокумент6 страницElectrolyte Imbalance Cause Signs and Symptoms Intervention ConnectionmkninnyОценок пока нет
- Musculoskeletal PharmacologyДокумент18 страницMusculoskeletal PharmacologyBLEEMAGE100% (2)
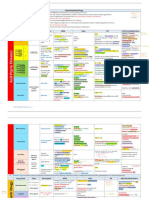
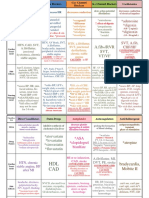
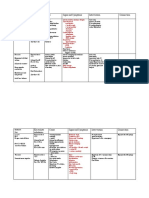
- Internal Medicine Table SummaryДокумент31 страницаInternal Medicine Table SummaryShazaan Nadeem100% (1)
- Genetic Conditions For USMLEДокумент2 страницыGenetic Conditions For USMLEkcxieОценок пока нет
- Cardiac Drugs HypertensionДокумент5 страницCardiac Drugs HypertensionEciOwnsMeОценок пока нет
- Pharmacology - Use of Beta-Blockers & Arbs in Cardiovascular Disease Treating HypertensionДокумент5 страницPharmacology - Use of Beta-Blockers & Arbs in Cardiovascular Disease Treating HypertensionDana20SОценок пока нет
- Rhythm Interpretation and Its ManagementДокумент6 страницRhythm Interpretation and Its Managementjh_ajjОценок пока нет
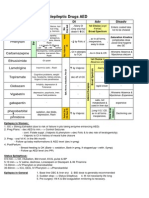
- Antiepileptic Drugs AED: D' DI Disadv SE AdvДокумент1 страницаAntiepileptic Drugs AED: D' DI Disadv SE Advrayooona88Оценок пока нет
- Comprehensive Nclex Notes Easy To Read PDFДокумент97 страницComprehensive Nclex Notes Easy To Read PDFKenia GeorgesОценок пока нет
- Antiseizure, Sedative & HypnoticsДокумент8 страницAntiseizure, Sedative & HypnoticsThulasi tootsieОценок пока нет
- 1) Misc: Neuro HY PearlsДокумент2 страницы1) Misc: Neuro HY Pearlsdsfan86Оценок пока нет
- Immunopharmacology PDFДокумент2 страницыImmunopharmacology PDFErica Hyeyeon LeeОценок пока нет
- Antianginal DrugsДокумент3 страницыAntianginal DrugsyukariОценок пока нет
- Cardiovascular Drug IntroductionДокумент3 страницыCardiovascular Drug IntroductionSamah Khan100% (1)
- Bam Slam Drug CardДокумент4 страницыBam Slam Drug CardLeticia GonzalezОценок пока нет
- Gastro MnemonicsДокумент8 страницGastro MnemonicsRufina SoomroОценок пока нет
- GI Signs and SymptomsДокумент40 страницGI Signs and SymptomsJohnny BeeОценок пока нет
- SyncopeДокумент3 страницыSyncopeanishdОценок пока нет
- MS Myasthenia Gravis Gillian-Barre Syndrome Parkinson's: Ascending Reversible ParalysisДокумент5 страницMS Myasthenia Gravis Gillian-Barre Syndrome Parkinson's: Ascending Reversible ParalysishaxxxessОценок пока нет
- Acid Base Handout RevisedДокумент3 страницыAcid Base Handout RevisedKaren HutchinsonОценок пока нет
- Lab Values and Vital SignsДокумент4 страницыLab Values and Vital SignsWole Olaluwoye100% (1)
- Heart Rhythms S SДокумент3 страницыHeart Rhythms S SGloryJane100% (1)
- Notes ImДокумент5 страницNotes Imsharmee sarmientaОценок пока нет
- Hierarchy of O2 Delivery SystemsДокумент1 страницаHierarchy of O2 Delivery SystemsRevОценок пока нет
- 3 Treatment of HypertensionДокумент7 страниц3 Treatment of HypertensiontiaraОценок пока нет
- Chapter 1 Compatible ModeДокумент93 страницыChapter 1 Compatible ModeJyha KhariОценок пока нет
- Opioids PDFДокумент2 страницыOpioids PDFErica Hyeyeon LeeОценок пока нет
- Immunopharmacology PDFДокумент2 страницыImmunopharmacology PDFErica Hyeyeon LeeОценок пока нет
- Asthma - Respiratory PDFДокумент1 страницаAsthma - Respiratory PDFErica Hyeyeon Lee0% (1)
- Ninja - Anti-Coagulants PDFДокумент3 страницыNinja - Anti-Coagulants PDFErica Hyeyeon Lee100% (1)
- Ninja - Antiarrhythmic Drugs PDFДокумент7 страницNinja - Antiarrhythmic Drugs PDFErica Hyeyeon Lee100% (1)
- Ninja - Autacoids PDFДокумент3 страницыNinja - Autacoids PDFErica Hyeyeon LeeОценок пока нет
- Ninja - Anti-HTN PDFДокумент6 страницNinja - Anti-HTN PDFErica Hyeyeon Lee100% (2)
- Ninja - Cholinergic Drugs PDFДокумент4 страницыNinja - Cholinergic Drugs PDFErica Hyeyeon Lee100% (2)
- 0.5. ANS Quicksheet PDFДокумент1 страница0.5. ANS Quicksheet PDFErica Hyeyeon LeeОценок пока нет
- Written Report Coronary Heart DiseaseДокумент5 страницWritten Report Coronary Heart DiseaseJade WushuОценок пока нет
- The Cholesterol Time BombДокумент464 страницыThe Cholesterol Time BombSophia NadalОценок пока нет
- PATHOLOGY Mendelian DisordersДокумент8 страницPATHOLOGY Mendelian DisordersAmna BaigОценок пока нет
- Bios Life Slim On PDRДокумент1 страницаBios Life Slim On PDRTemitayo BewajiОценок пока нет
- Guidelines For The Diagnosis and Management of Heterozygous Familial Hypercholesterolemia PDFДокумент14 страницGuidelines For The Diagnosis and Management of Heterozygous Familial Hypercholesterolemia PDFai_tОценок пока нет
- Meta-Analyses of Statin Therapy For Primary Prevention Do Not Answer Key Questions: An Empirical Appraisal of 5 Years of Statin Meta-AnalysesДокумент8 страницMeta-Analyses of Statin Therapy For Primary Prevention Do Not Answer Key Questions: An Empirical Appraisal of 5 Years of Statin Meta-AnalysesJulio JuarezОценок пока нет
- Becker Red Yeast Rice 2009Документ13 страницBecker Red Yeast Rice 2009Miin ChanОценок пока нет
- How Cholesterol WorksДокумент7 страницHow Cholesterol WorksVishal Kumar ShawОценок пока нет
- Reabilitare Dupa AvcДокумент91 страницаReabilitare Dupa AvcDiana StancaОценок пока нет
- Pengaruh Pemberian Sari Tebu Terhadap Kadar Kolesterol Darah Pada MencitДокумент7 страницPengaruh Pemberian Sari Tebu Terhadap Kadar Kolesterol Darah Pada MencitGaluhFahmiОценок пока нет
- Kanukula 2019Документ7 страницKanukula 2019Dianne GalangОценок пока нет
- 33 Side Effects of FoodsДокумент13 страниц33 Side Effects of FoodsFrankDicksonОценок пока нет
- Liver TransplantДокумент16 страницLiver TransplantNephrology On-DemandОценок пока нет
- RX - Citicoline, Kalium, Ketosteril, Methycobal, Myonal, Lipolin GelДокумент6 страницRX - Citicoline, Kalium, Ketosteril, Methycobal, Myonal, Lipolin GelntootОценок пока нет
- Cwe Nephrotic SnydromeДокумент12 страницCwe Nephrotic SnydromeFariezuan HamidОценок пока нет
- Heart AttackДокумент12 страницHeart AttackPaul NeedhamОценок пока нет
- Midterms Group 5Документ25 страницMidterms Group 5Karina MadriagaОценок пока нет
- DSS - Bridging The Gaps Tackling Inequalities in Cardiovascular DiseaseДокумент19 страницDSS - Bridging The Gaps Tackling Inequalities in Cardiovascular DiseaseEduard MoraruОценок пока нет
- Drug Study CHFДокумент13 страницDrug Study CHFALIANA KIMBERLY MALQUESTOОценок пока нет
- Annotated BibliographyДокумент4 страницыAnnotated Bibliographyapi-348925782Оценок пока нет
- 2-Unicity Balance PDFДокумент17 страниц2-Unicity Balance PDFLuis A Gil PantojaОценок пока нет
- Dislipidemia Lancet Durrington PDFДокумент15 страницDislipidemia Lancet Durrington PDFAlphaJulissa JuarezОценок пока нет
- Medical Hazards of Obesity: Ann Intern Med. 1993 119 (7 PT 2) :655-660Документ6 страницMedical Hazards of Obesity: Ann Intern Med. 1993 119 (7 PT 2) :655-660David WheelerОценок пока нет
- BIOS LIFE - Cleveland Clinic Trial by Dr. Dennis SprecherДокумент5 страницBIOS LIFE - Cleveland Clinic Trial by Dr. Dennis SprecherHisWellnessОценок пока нет
- Statin Drug StudyДокумент3 страницыStatin Drug StudyNikael Patun-ogОценок пока нет
- Bandana Chatterjee Et Al.Документ4 страницыBandana Chatterjee Et Al.International Journal of Clinical and Biomedical Research (IJCBR)Оценок пока нет
- Cholesterol TCM PDFДокумент6 страницCholesterol TCM PDFMartijn JohanОценок пока нет
- Health7 4TH Quarter ModuleДокумент20 страницHealth7 4TH Quarter Modulearmand bayoranОценок пока нет
- Malunggay MonographДокумент9 страницMalunggay Monographkiara4decenaОценок пока нет
- Biologia Celular y Moleculas - TallerДокумент2 страницыBiologia Celular y Moleculas - TallerJulieth Karina Mendoza AcostaОценок пока нет