Академический Документы
Профессиональный Документы
Культура Документы
Artigo Cientifico
Загружено:
Gaetano Di GiovanniОригинальное название
Авторское право
Доступные форматы
Поделиться этим документом
Поделиться или встроить документ
Этот документ был вам полезен?
Это неприемлемый материал?
Пожаловаться на этот документАвторское право:
Доступные форматы
Artigo Cientifico
Загружено:
Gaetano Di GiovanniАвторское право:
Доступные форматы
Bardia et al Perioperative Management
Preoperative chlorhexidine mouthwash to reduce
pneumonia after cardiac surgery: A systematic review and
meta-analysis
Amit Bardia, MBBS,a Daina Blitz, MD,a Feng Dai, MS, PhD,b Denise Hersey, MLS, MA,c
Sayuri Jinadasa, MD,d Mayanka Tickoo, MD,e and Robert B. Schonberger, MDa
ABSTRACT Preoperative Chlorhexidine Mouthwash to Reduce Pneumonia
after Cardiac Surgery: A Systematic Review and Meta-analysis.
Full text articles excluded for following reasons:
n = 15 (not prospective studies)
Studies excluded on screening n = 2 (Chlorhexidine not administered preoperatively)
Duplicate articles excluded (n = 181) n = 1 (Pediatric population)
Objective: Postoperative pneumonia is one of the most common complications
(n = 167)
Titles and abstracts identified through literature
after cardiac surgery, entailing increased patient morbidity, mortality, and health
search Titles and abstracts screened after duplicates Full text articles independently assessed for
Studies included in Meta-Analysis
(n = 371) removed eligibility
(n = 5)
PubMed = 94, Ovid/EMBASE = 83, (n = 204) (n = 23)
CINAHL = 48, SCOPUS = 146
care burden. The primary aim of this study was to assess whether preoperative
chlorhexidine mouthwash is associated with reduced postoperative pneumonia af- Study or Subgroup
DeRiso et al. 1996
Chlorhexidine
5
Control
Events Total Events Total
173 17 180 9.0%
Risk Ratio
Weight IV, Random, 95% Cl
0.31 [0.12, 0.81]
Year
1996
Risk Ratio
IV, Random, 95% Cl
Houston et al. 2002 4 270 9 291 6.3% 0.48 [0.15, 1.54] 2002
ter cardiac surgery. Segers et al. 2006
Nicolosi et al. 2014
Lin et al 2015
Total (95% Cl)
45
4
4
1125
485
150
47
74
13
11
1159 100.0%
491
150
47
70.2%
7.1%
7.4%
0.62 [0.43, 0.87]
0.31 [0.10, 0.92]
0.36 [0.12, 1.06]
0.52 [0.39, 0.70]
2006
2014
2015
Total events 62 124
Heterogeneity: Tau2 = 0.00; Chi2 = 3.36, df = 4 (P = .50); I2 = 0%
Test for overall effect: Z = 4.37 (P < .0001) 0.01 0.1 1 10 100
Methods: A comprehensive systematic search of NLM Pubmed, Embase, Sco- Favours [Chlorhexidine] Favours [Control]
pus, and Cumulative Index of Nursing and Allied Health was executed to include Postoperative pneumonia after cardiac surgery with
the studies since inception to June 27, 2017, which assessed the effects of preop- respect to chlorhexidine mouthwash.
erative chlorhexidine gluconate mouthwash on postoperative pneumonia. Studies
were identified by 2 independent reviewers, and data were extracted using a pre- Central Message
defined protocol. Random effects models were run to obtain risk ratios with 95% Preoperative chlorhexidine use is associated
confidence intervals. Quality of evidence was evaluated using Grading of Recom- with a reduction in postoperative pneumonia
after cardiac surgery.
mendations Assessment, Development and Evaluation criteria. Postoperative
PM
pneumonia after cardiac surgery was the primary outcome of the study.
Perspective
Results: Five studies including a cumulative of 2284 patients were included. A The findings of this paper suggest a reduction in
total of 1125 patients received preoperative chlorhexidine. Use of chlorhexidine postoperative pneumonia after cardiac surgery
gluconate was associated with reduced risk of postoperative pneumonia compared with the use of preoperative chlorhexidine.
Incorporation of this relatively simple maneu-
with the patients who did not receive it (risk ratio, 0.52; 95% confidence interval,
ver may significantly improve postoperative
0.39-0.70; P<.001). No adverse effects from chlorhexidine gluconate mouthwash outcomes in the cardiac surgery patient
were reported by any of these studies. population.
Conclusions: Among the patients receiving preoperative chlorhexidine mouth-
wash, the risk of postoperative pneumonia is reduced by approximately one- See Commentary on page XXX.
half; its adoption in preoperative protocols could help improve patient outcomes.
(J Thorac Cardiovasc Surg 2019;-:1-7)
Postoperative pneumonia is one of the most prevalent system, as it directly impacts ventilator days, length of
hospital-acquired infections after cardiac surgeries, attrib- stay in the intensive care unit (ICU), and total hospital
uting to a 4-fold increase in the risk of mortality.1 In addi- length of stay.2 Preventing pneumonia after cardiac surgery
tion, it incurs tremendous burden on the health care is especially challenging since the usual preventive maneu-
vers used in the ICU,3,4 such as semirecumbent positioning,
subglottic suctioning, and sedation interruption, are not
From the aDepartment of Anesthesiology and ePulmonary and Critical Care Medi- practical in the intraoperative period.
cine, Department of Internal Medicine, Yale School of Medicine, New Haven, Daily mouthwash with chlorhexidine gluconate, a broad-
Conn; bDepartment of Biostatistics, Yale School of Public Health, New Haven,
Conn; cScience Libraries, Scholarly Collections and Research Services, Princeton spectrum antimicrobial, has been shown to significantly
University, Princeton, NJ; and dDepartment of Surgery, Beth Israel Deaconess reduce the incidence of ventilator-associated pneumonia
Medical Center, Harvard Medical School, Boston, Mass.
Drs Bardia and Blitz contributed equally to this article.
Received for publication Aug 28, 2018; revisions received Dec 18, 2018; accepted for
publication Jan 6, 2019. Scanning this QR code will take
Address for reprints: Amit Bardia, MBBS, Department of Anesthesiology, Yale you to the article title page to
School of Medicine, New Haven, CT 06515 (E-mail: amit.bardia@yale.edu).
0022-5223/$36.00 access supplementary informa-
Copyright Ó 2019 by The American Association for Thoracic Surgery tion.
https://doi.org/10.1016/j.jtcvs.2019.01.014
The Journal of Thoracic and Cardiovascular Surgery c Volume -, Number - 1
Perioperative Management Bardia et al
Search and Selection Strategy
Abbreviations and Acronyms A comprehensive search using NLM Pubmed, Embase, Scopus, and Cu-
mulative Index of Nursing and Allied Health was performed. The Medical
CI ¼ confidence interval Subject Headings terms and key words are shown in the Online Data
ICU ¼ intensive care unit Supplement 1. To summarize in brief, the terms used included preopera-
RCT ¼ randomized controlled trial tive, chlorhexidine, mouthwash, cardiac surgery, heart surgery, pneumonia,
RR ¼ risk ratio prevent, and cardiovascular. All searches were run on June 27, 2017, by the
VAP ¼ ventilator-associated pneumonia institutional librarian. Study inclusion criteria were decided a priori. Only
human studies involving cardiac surgeries on adult patient populations that
tested the effect of chlorhexidine preoperatively on postoperative pneu-
monia were included. This included randomized control trials as well as
(VAP).5,6 Despite some evidence signaling its beneficial
studies using a pre-post intervention design with historical controls. No
effect,7 routine use of preoperative chlorhexidine mouth- language restrictions were imposed.
wash for preventing postoperative pneumonia after cardiac For articles meeting the initial screening, full-text articles were then
surgeries is not a universal practice. Data regarding the effi- independently evaluated to assess for eligibility by 2 investigators (D.B.
cacy and safety of chlorhexidine mouthwash in preventing and A.B.). The investigators (D.B. and A.B.) independently used a prede-
fined questionnaire for study evaluation. In the case of discrepancy, this
postoperative pneumonia may help health care providers to
was to be resolved by discussion with the senior author (R.S.). All the out-
improve postoperative outcomes. To address this, we con- comes were based on aggregated data that were extracted from results of
ducted a meta-analysis and systematic review to assess the eligible studies. No individual participant data were available for the
efficacy of preoperative chlorhexidine gluconate mouthwash meta-analysis. Data were independently extracted by 2 coauthors (A.B.
in reducing postoperative pneumonia after cardiac surgery. and D.B.) and compared to check for inconsistency/missing data. Data
were then analyzed according to our predefined statistical plan.
METHODS
Data Sources and Searches Outcomes
This systematic review is reported according to the Preferred Reporting The primary outcome was postoperative pneumonia after cardiac
PM
Items for Systematic Reviews and Meta-analyses statement for surgery. Secondary outcomes included postoperative mortality, gram-
meta-analysis.8 positive pneumonia, and gram-negative pneumonia in the 2 groups.
Titles and abstracts identified through literature
search
(n = 371)
PubMed = 94, Ovid/EMBASE = 83,
CINAHL = 48, SCOPUS = 146
Duplicate articles excluded
(n = 167)
Titles and abstracts screened after duplicates
removed
(n = 204)
Studies excluded on screening
(n = 181)
Full text articles independently assessed for
eligibility
(n = 23)
Full text articles excluded for following reasons:
n = 15 (not prospective studies)
n = 2 (Chlorhexidine not administered preoperatively)
n = 1 (Pediatric population)
Studies included in Meta-Analysis
(n = 5)
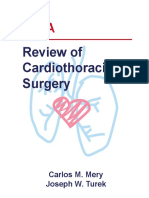
FIGURE 1. Preferred Reporting Items for Systematic Reviews and Meta-analyses flow diagram depicting study inclusion process. NLM Pubmed, Embase,
Scopus, and Cumulative Index of Nursing and Allied Health (CINAHL) databases were searched for key terms related to preoperative chlorhexidine mouth-
wash, postoperative pneumonia, and cardiac surgery. Five studies were included in the metanalysis after removal of duplicates and studies that did not meet
the inclusion criteria.
2 The Journal of Thoracic and Cardiovascular Surgery c - 2019
Bardia et al Perioperative Management
Quality of Evidence RESULTS
The quality of evidence was audited using the Grading of Study Characteristics
Recommendations Assessment, Development and Evaluation criteria Of the 371 citations, after assessment of full-text articles
for meta-analysis.9
and adjusting for duplicates, 5 articles met the inclusion
criteria.13-17 The Preferred Reporting Items for Systematic
Statistical Analysis
Statistical analysis and reporting were performed based on previous
Reviews and Meta-analyses flow diagram of the study se-
published guidelines by the journal.10-12 Random-effects model method lection process is shown in Figure 1.
was implemented in Review Manager (RevMan) software version 5.3 A total of 2284 cumulative subjects (26.7% women)
(The Nordic Cochrane Centre, The Cochrane Collaboration, Copenhagen, from the 5 articles were included in this study, of whom
Denmark, 2014). Risk ratio (RR) and 95% confidence intervals (CIs) were 1125 received preoperative chlorhexidine. Of these, only
used for reporting the magnitude of the effect size for binary outcomes. The
I2 statistic was used to assess heterogeneity, and Cochrane’s Q test statistic
1 study (Nicolosi and colleagues)16 was a pre-post study,
was used to assess its statistical significance. All P values <.05 were and the remaining 4 studies were RCTs. The key clinical
considered to be statistically significant. Sensitivity analysis was also per- characteristics of these studies are listed in Table 1.13-19
formed to include only data from randomized controlled trials (RCTs). The The majority of surgeries in all the studies comprised cor-
limited number of studies precluded the use of a funnel plot or meta- onary artery bypass grafting, valvular heart surgery, or both.
regression analyses.
None of the studies included ventricular assist device
TABLE 1. Clinical characteristics of the included studies
Sample size Criteria for
Type of cardiac (chlorhexidine vs Chlorhexidine diagnosing
Study (y) Location surgery control) regimen pneumonia
Lin et al, 201515 China All cardiac surgeries 94 (47 vs 47) Chlorhexidine vs Clinical Pulmonary
PM
normal saline Infection Score
(CPIS) criteria18
Nicolosi et al, 201416 Argentina Nonemergent cardiac 300 (150 vs 150) Chlorhexidine vs Evidence of a new
surgeries usual care lung infiltrate on
chest radiograph
and at least 2 of the
following:
leukocytosis, fever,
or purulent
tracheobronchial
secretion
Segers et al, 200617 The Netherlands Nonemergent cardiac 991 (500 vs 491) Chlorhexidine vs CDC criteria19
surgeries placebo of
comparable color,
taste, and smell
Houston et al, 200214 US CABG, valvular 561 (270 vs 291) Chlorhexidine vs Nature of
surgery, combined Listerine (McNeil tracheobronchial
CABG and valvular Consumer secretions, evidence
surgery Healthcare, Fort of fever, degree of
Washington, Penn) leukocytosis,
microbial culture
results, and
evidence of
pulmonary infiltrate
DeRiso et al, 199613 US CABG, valvular 353 (173 vs 180) Chlorhexidine vs base New or progressing
surgery, combined solution of pulmonary
CABG and valvular chlorhexidine infiltrate, fever,
surgery, septal leukocytosis, and
surgery, cardiac purulent
tumor excision tracheobronchial
secretions
CDC, Centers for Disease Control and Prevention; CABG, coronary artery bypass grafting.
The Journal of Thoracic and Cardiovascular Surgery c Volume -, Number - 3
Perioperative Management Bardia et al
colleagues)13 to rinses every 12 hours for 3 days preopera-
Blinding of participants and personnel (performance bias)
tively (Nicolisi and colleagues).16 Perioperative antimicro-
bial coverage by cephalosporins or vancomycin was used
Blinding of outcome assessment (detection bias)
by all the investigators (except Lin and colleagues,15 who
Random sequence generation (selection bias)
did not mention perioperative antibiotic coverage). Stan-
dard guidelines for diagnosing pneumonia were used by
Incomplete outcome data (attrition bias)
Allocation concealment (selection bias)
all the study groups, which included new or progressing
Selective reporting (reporting bias)
pulmonary infiltrates on chest radiograph, fever, leukocy-
tosis, purulent tracheobronchial secretions, and microbial
culture results.
Risk of Bias Assessment
The Cochrane risk of bias assessment tool was used for
assessment of the trials (Figure 2).9,20 Overall, 4 trials
(80%) had adequate sequence generation and 3 (60%)
had allocation concealment. Adequate blinding of study
personnel including outcome assessors was present in 3
(60%) of the trials. Two of the 5 studies were considered
De Riso et al. + + + ? ? +
to be at a low risk for incomplete outcomes data. In the
Houston et al. + ? ? + ? + cumulative assessment of bias, 3 of the 5 trials were
deemed to have an overall low risk of bias.
Lin et al. + + + + ? +
Primary Outcome
PM
Nicolisi et al. – – – ? + ?
Use of chlorhexidine was significantly associated with
Segars et al. + + + + + + reduced risk of postoperative pneumonia (RR, 0.52; 95%
CI, 0.39-0.70; P<.001) (Figure 3). There was minimal het-
FIGURE 2. Risk of bias summary for the included clinical studies. All the erogeneity among the reported trials, I2 ¼ 0%. We also per-
5 studies were assessed for risk of bias based on Cochrane’s Collaboration
formed a sensitivity analysis for the primary outcome by
tool. Green, yellow, and red colors signify low, unclear, and high risk of
including only RCTs. No significant change in the effect
bias, respectively.
or the overall outcome was observed (RR, 0.54; 95% CI,
0.40-0.73; P <.0001).
placement, and 1 study included 5 heart transplant surgeries
(Lin and colleagues15). Common exclusion criteria Secondary Outcomes
included preoperative infection, preoperative intubation, Postoperative pneumonia in the chlorhexidine group was
pregnancy, emergency surgery, and intraoperative death. significantly lower for gram-positive organisms (RR, 0.30;
Formulations containing 0.12% to 0.2% chlorhexidine 95% CI, 0.12-0.76; P ¼ .01; I2 ¼ 0%) (Figure 4). The asso-
were used for preoperative decontamination by the various ciation did not reach statistical significance in the gram-
study groups. The methodology used for oral decontamina- negative group (RR, 0.47; 95% CI, 0.22-1.02; P ¼ .06;
tion ranged from one preoperative rinse (DeRiso and I2 ¼ 56%). No significant difference in the in-hospital
Chlorhexidine Control Risk Ratio Risk Ratio
Study or Subgroup Events Total Events Total Weight IV, Random, 95% Cl Year IV, Random, 95% Cl
DeRiso et al. 1996 5 173 17 180 9.0% 0.31 [0.12, 0.81] 1996
Houston et al. 2002 4 270 9 291 6.3% 0.48 [0.15, 1.54] 2002
Segers et al. 2006 45 485 74 491 70.2% 0.62 [0.43, 0.87] 2006
Nicolosi et al. 2014 4 150 13 150 7.1% 0.31 [0.10, 0.92] 2014
Lin et al 2015 4 47 11 47 7.4% 0.36 [0.12, 1.06] 2015
Total (95% Cl) 1125 1159 100.0% 0.52 [0.39, 0.70]
Total events 62 124
Heterogeneity: Tau2 = 0.00; Chi2 = 3.36, df = 4 (P = .50); I2 = 0%
Test for overall effect: Z = 4.37 (P < .0001) 0.01 0.1 1 10 100
Favours [Chlorhexidine] Favours [Control]
FIGURE 3. Forest plot comparing postoperative pneumonia after cardiac surgery in patients with or without preoperative chlorhexidine mouthwash. Use of
chlorhexidine was significantly associated with reduced risk of postoperative pneumonia (risk ratio, 0.52; 95% CI, 0.39-0.70; P<.001). IV, Inverse variance
weighting; CI, confidence interval.
4 The Journal of Thoracic and Cardiovascular Surgery c - 2019
Bardia et al Perioperative Management
Gram Positive Pneumonia
Chlorhexidine Control Risk Ratio Risk Ratio
Study or Subgroup Events Total Events Total Weight IV, Random, 95% CI Year IV, Random, 95% CI
DeRiso et al. 1996 1 142 4 147 17.6% 0.26 [0.03, 2.29] 1996
Segers et al. 2006 3 485 12 469 52.8% 0.24 [0.07, 0.85] 2006
Nicolosi et al. 2014 2 150 4 150 29.6% 0.50 [0.09, 2.69] 2014
Total (95% CI) 777 766 100.0% 0.30 [0.12, 0.76]
Total events 6 20
Heterogeneity: Tau = 0.00; Chi = 0.48, df = 2 (P = .78); I2 = 0%
2 2
Test for overall effect: Z = 2.56 (P = .01) 0.01 0.1 1 10 100
A Favours [Chlorhexidine] Favours [Control]
Gram Negative Pneumonia
Chlorhexidine Control Risk Ratio Risk Ratio
Study or Subgroup Events Total Events Total Weight IV, Random, 95% CI Year IV, Random, 95% CI
DeRiso et al. 1996 5 173 16 180 30.2% 0.33 [0.12, 0.87] 1996
Segers et al. 2006 41 485 52 469 51.9% 0.76 [0.52, 1.13] 2006
Nicolosi et al. 2014 2 150 9 150 17.9% 0.22 [0.05, 1.01] 2014
Total (95% CI) 808 799 100.0% 0.47 [0.22, 1.02]
Total events 48 77
Heterogeneity: Tau2 = 0.26; Chi2 = 4.48, df = 2 (P = .11); I2 = 55%
Test for overall effect: Z = 1.92 (P = .06) 0.01 0.1 1 10 100
B Favours [Chlorhexidine] Favours [Control]
FIGURE 4. Forest plot comparing postoperative pneumonia with gram-positive organisms (A) and gram-negative organisms (B) after cardiac surgery in
patients with or without preoperative chlorhexidine mouthwash. Postoperative pneumonia in the chlorhexidine group was significantly lower for gram-
positive organisms (risk ratio, 0.30; 95% CI, 0.12-0.76; P ¼ .01; I2 ¼ 0%). The association did not reach statistical significance in the gram-negative group
PM
(risk ratio, 0.47; 95% CI, 0.22-1.02; P ¼ .06; I2 ¼ 55%). IV, Inverse variance weighting; CI, confidence interval.
mortality rates was observed (RR, 0.98; 95% CI, 0.43-2.23; mouthwash on postoperative pneumonia after cardiac
P ¼ .95; I2 ¼ 47%) (Figure 5). Other parameters such as surgeries. The study has several important findings. First,
duration of mechanical ventilation, length of ICU stay, postoperative pneumonia is a common postoperative
and length of hospital stay were not uniformly reported by complication after cardiac surgery, with a cumulative inci-
all the studies (Online Data Supplement 2). The studies by dence of about 8% among all studies combined. Second,
Nicolosi and colleagues and Segers and colleagues report chlorhexidine mouthwash was associated with significant
a small benefit in hospital stay with chlorhexidine mouth- reduction in the risk of postoperative pneumonia after car-
wash use, whereas DeRiso and colleagues report no such diac surgery. Third, this protective effect is particularly pro-
benefit. The studies report no significant differences in found for gram-positive organisms.
ventilator time between the 2 groups. None of the studies re- Chlorhexidine mouthwash to prevent VAP in the ICU
ported any adverse effects from chlorhexidine mouthwash. setting has been recognized.21-23 The findings of our
study resemble those by Hua and colleagues.24 In their
DISCUSSION metanalysis consisting of 6016 participants (37 RCTs)
In this systemic review and meta-analysis, direct evi- who were critically ill and expected to require mechanical
dence from 5 studies in 2284 patients was combined to ventilation for a minimum of 48 hours, use of chlorhexidine
assess the effect of preoperative chlorhexidine gluconate mouthwash was found to be associated with a decreased
Chlorhexidine Control Risk Ratio Risk Ratio
Study or Subgroup Events Total Events Total Weight IV, Random, 95% Cl Year IV, Random, 95% Cl
DeRiso et al. 1996 2 173 10 180 19.3% 0.21 [0.05, 0.94] 1996
Houston et al. 2002 6 270 3 291 21.6% 2.16 [0.54, 8.53] 2002
Segers et al. 2006 8 485 6 469 28.7% 1.29 [0.45, 3.69] 2006
Nicolosi et al. 2014 8 150 7 150 30.3% 1.14 [0.43, 3.07] 2014
Total (95% Cl) 1078 1090 100.0% 0.98 [0.43, 2.23]
Total events 24 26
Heterogeneity: Tau2 = 0.33; Chi2 = 5.67, df = 3 (P = .13); I2 = 47%
Test for overall effect: Z = 0.06 (P = .95) 0.01 0.1 1 10 100
Favours [Chlorhexidine] Favours [Control]
FIGURE 5. Forest plot comparing postoperative in-hospital mortality after cardiac surgery with respect to chlorhexidine mouthwash. No significant
difference in the in-hospital mortality rates was observed (risk ratio, 0.98; 95% CI, 0.43-2.23; P ¼ .95; I2 ¼ 47%). IV, Inverse variance weighting;
CI, confidence interval.
The Journal of Thoracic and Cardiovascular Surgery c Volume -, Number - 5
Perioperative Management Bardia et al
Our study has some limitations. First, as only a few
studies met the inclusion criteria, the small sample size
may influence the generalizability of these results to the
wider cardiac surgery population. Because of the small
number of studies, meta-regression analysis could also not
be performed. It is also important to note that the low value
of I2 statistic could be due to a small sample size. However,
we reported 95% CIs in addition to point estimates for addi-
tional characterization of the heterogenicity and chose a
random effects model that would be able to accommodate
differential effects of the intervention among studies.
VIDEO 1. Video abstract summarizing the systematic review and meta- Second, our study only examined cardiac surgeries, and
analysis of the use of preoperative chlorhexidine mouthwash to prevent thus its generalizability to noncardiac surgical populations
postoperative pneumonia after cardiac surgery. Video available at: http:// is unclear. The studies used differing protocols for preoper-
www.jtcvs.org.
ative chlorhexidine mouthwash. It is difficult to comment
whether a particular protocol was superior to another. Simi-
rate of VAPs (RR, 0.75; 95% CI, 0.62-0.91; P ¼ .004; larly, the control group did not have exactly the same expo-
I2 ¼ 35%). Similar to our findings, there was no mortality sure. This may be a source of heterogeneity of effects,
benefit with chlorhexidine mouthwash (RR, 1.09; 95% further justifying our choice of a random effects model to
CI, 0.96-1.23; P ¼ .20; I2 ¼ 0%). However, the role of pre- accommodate the potential for heterogeneity. Finally,
operative chlorhexidine in preventing postoperative pneu- although the study was not registered in PROSPERO, it
monia remains unclear. Our study highlights the was performed according to an a priori statistical plan as
protective effect of preoperative chlorhexidine mouthwash mentioned previously.
PM
for preventing postoperative pneumonia after cardiac
surgery. CONCLUSIONS
Microaspiration of microflora in the aero-digestive tract Preoperative chlorhexidine is associated with a signifi-
has been implicated for the pathophysiology of pneumonia cant reduction in postoperative pneumonia after cardiac sur-
in intubated patients. Oral decontamination by chlorhexi- gery. This relatively simple intervention was not associated
dine could possibly decrease this microbial burden and with any adverse events in the studies included in the meta-
hence exert its protective effect. This putative biological ba- analysis. Preoperative chlorhexidine mouthwash should be
sis for the protective effect of chlorhexidine was consistent considered in suitable patients undergoing cardiac surgeries
with the finding that its efficacy appears to be particularly (Video 1).
pronounced for preventing gram-positive pneumonia. The
predominant bacteria in this group are Staphylococcus spe- Conflicts of Interest
cies, which are known to frequently colonize the nasopha- Dr Schonberger holds an equity position in Johnson & John-
ryngeal region. Chlorhexidine mouthwash thus has a son. All other authors have nothing to disclose with regard
highly plausible biological basis to decrease the incidence to commercial support.
of postoperative pneumonia. The fact that a similar effect
was not seen for gram-negative organisms would be consis- We thank Suveen Angraal, MD, for his help with the statistical
tent with the notion that a majority of gram-negative pneu- inputs; Dr Manuel Fontes, Dr Chris Szabo, and Dr Arnar Geirsson
monia infections are likely secondary to aspiration of for the idea conception and departmental support; and Garrett
gastrointestinal contents in intubated patients, and it would Sendlewski for his extensive help with graphical abstract and
not be expected that mouthwash by chlorhexidine in isola- video summary creation. This publication was made possible by
tion would provide protection from the gastrointestinal CTSA Grant Number UL1 TR000142 from the National Center
for Advancing Translational Science (NCATS), a component of
microbiome.
the National Institutes of Health (NIH). Its contents are solely
Importantly, we did not observe a significant decrease in
the responsibility of the authors and do not necessarily represent
overall in hospital mortality. A possible reason for this the official view of NIH.
could be that in-hospital mortality occurs due to multiple
etiologies after cardiac surgery, with postoperative pneu-
References
monia being an important factor in only a minority of 1. Kinlin LM, Kirchner C, Zhang H, Daley J, Fisman DN. Derivation and validation
such cases. Another possible reason could be that our study of a clinical prediction rule for nosocomial pneumonia after coronary artery
was underpowered to detect a difference, since in-hospital bypass graft surgery. Clin Infect Dis. 2010;50:493-501.
2. He S, Chen B, Li W, Yan J, Chen L, Wang X, et al. Ventilator-associated pneu-
mortality was an infrequent outcome (2.3% among studies monia after cardiac surgery: a meta-analysis and systematic review. J Thorac
that reported the outcome). Cardiovasc Surg. 2014;148:3148-55.e3141-5.
6 The Journal of Thoracic and Cardiovascular Surgery c - 2019
Bardia et al Perioperative Management
3. Hellyer TP, Ewan V, Wilson P, Simpson AJ. The intensive care society recom- 15. Lin YJ, Xu L, Huang XZ, Jiang F, Li SL, Lin F, et al. Reduced occurrence of
mended bundle of interventions for the prevention of ventilator-associated pneu- ventilator-associated pneumonia after cardiac surgery using preoperative 0.2%
monia. J Intensive Care Soc. 2016;17:238-43. chlorhexidine oral rinse: results from a single-centre single-blinded randomized
4. Morris AC, Hay AW, Swann DG, Everingham K, McCulloch C, McNulty J, et al. trial. J Hosp Infect. 2015;91:362-6.
Reducing ventilator-associated pneumonia in intensive care: impact of imple- 16. Nicolosi LN, del Carmen Rubio M, Martinez CD, Gonzalez NN, Cruz ME. Effect
menting a care bundle. Crit Care Med. 2011;39:2218-24. of oral hygiene and 0.12% chlorhexidine gluconate oral rinse in preventing
5. Ozcaka O, Basoglu OK, Buduneli N, Tasbakan MS, Bacakoglu F, Kinane DF. ventilator-associated pneumonia after cardiovascular surgery. Respir Care.
Chlorhexidine decreases the risk of ventilator-associated pneumonia in intensive 2014;59:504-9.
care unit patients: a randomized clinical trial. J Periodontal Res. 2012;47:584-92. 17. Segers P, Speekenbrink RG, Ubbink DT, van Ogtrop ML, de Mol BA. Prevention
6. Fourrier F, Cau-Pottier E, Boutigny H, Roussel-Delvallez M, Jourdain M, of nosocomial infection in cardiac surgery by decontamination of the naso-
Chopin C. Effects of dental plaque antiseptic decontamination on bacterial colo- pharynx and oropharynx with chlorhexidine gluconate: a randomized controlled
nization and nosocomial infections in critically ill patients. Intensive Care Med. trial. JAMA. 2006;296:2460-6.
2000;26:1239-47. 18. Rosbolt MB, Sterling ES, Fahy BG. The utility of the clinical pulmonary infec-
7. Klompas M, Speck K, Howell MD, Greene LR, Berenholtz SM. Reappraisal of tion score. J Intensive Care Med. 2009;24:26-34.
routine oral care with chlorhexidine gluconate for patients receiving mechanical venti- 19. Tablan OC, Anderson LJ, Besser R, Bridges C, Hajjeh R, CDC; Healthcare Infec-
lation: systematic review and meta-analysis. JAMA Intern Med. 2014;174:751-61. tion Control Practices Advisory Committee. Guidelines for preventing health-
8. Moher D, Liberati A, Tetzlaff J, Altman DG, PRISMA Group. Preferred report- care–associated pneumonia, 2003: Recommendations of cdc and the healthcare
ing items for systematic reviews and meta-analyses: the PRISMA statement. infection control practices advisory committee. MMWR Recomm Rep. 2004;
BMJ. 2009;339:b2535. 53:1-36.
9. Sch€ unemann H, Bro_zek J, Guyatt G, Oxman A, eds. The GRADE handbook. 20. Higgins JP, Altman DG, Gotzsche PC, Juni P, Moher D, Oxman AD, et al.
Available at: http://gdt.guidelinedevelopment.org/app/handbook/handbook.html. Cochrane Statistical Methods Group. The Cochrane Collaboration’s tool for as-
Accessed August 10, 2018. sessing risk of bias in randomised trials. BMJ. 2011;343:d5928.
10. Blackstone EH, Weisel RD. The conclusion of papers published in the journal 21. Chan EY, Ruest A, Meade MO, Cook DJ. Oral decontamination for prevention
should be supported by an appropriate statistical analysis. J Thorac Cardiovasc of pneumonia in mechanically ventilated adults: systematic review and meta-
Surg. 2014;148:2479. analysis. BMJ. 2007;334:889.
11. Huebner M, Vach W, le Cessie S. A systematic approach to initial data analysis is 22. Feider LL, Mitchell P, Bridges E. Oral care practices for orally intubated criti-
good research practice. J Thorac Cardiovasc Surg. 2016;151:25-7. cally ill adults. Am J Crit Care. 2010;19:175-83.
12. Rajeswaran J, Blackstone EH. Patient-reported outcomes and importance of their 23. Krein SL, Kowalski CP, Hofer TP, Saint S. Preventing hospital-acquired infec-
appropriate statistical analyses. J Thorac Cardiovasc Surg. 2015;150:461-2. tions: a national survey of practices reported by U.S. hospitals in 2005 and
13. DeRiso AJ II, Ladowski JS, Dillon TA, Justice JW, Peterson AC. Chlorhexidine 2009. J Gen Intern Med. 2012;27:773-9.
PM
gluconate 0.12% oral rinse reduces the incidence of total nosocomial respiratory 24. Hua F, Xie H, Worthington HV, Furness S, Zhang Q, Li C. Oral hygiene care for
infection and nonprophylactic systemic antibiotic use in patients undergoing critically ill patients to prevent ventilator-associated pneumonia. Cochrane Data-
heart surgery. Chest. 1996;109:1556-61. base Syst Rev. 2016;10:CD008367.
14. Houston S, Hougland P, Anderson JJ, LaRocco M, Kennedy V, Gentry LO. Effec-
tiveness of 0.12% chlorhexidine gluconate oral rinse in reducing prevalence of
nosocomial pneumonia in patients undergoing heart surgery. Am J Crit Care. Key Words: preoperative, chlorhexidine, mouthwash, post-
2002;11:567-70. operative pneumonia, cardiac surgery
The Journal of Thoracic and Cardiovascular Surgery c Volume -, Number - 7
Perioperative Management Bardia et al
000 Preoperative chlorhexidine mouthwash to reduce pneumonia after cardiac
surgery: A systematic review and meta-analysis
Amit Bardia, MBBS, Daina Blitz, MD, Feng Dai, MS, PhD, Denise Hersey, MLS, MA, Sayuri
Jinadasa, MD, Mayanka Tickoo, MD, and Robert B. Schonberger, MD, New Haven, Conn,
Princeton, NJ, and Boston, Mass
Preoperative chlorhexidine use is associated with a reduction in postoperative pneumonia after
cardiac surgery.
PM
The Journal of Thoracic and Cardiovascular Surgery c - 2019
Вам также может понравиться
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (400)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5795)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (345)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- 5-Surgical Management of Ptosis and Brow PtosisДокумент21 страница5-Surgical Management of Ptosis and Brow PtosisJovan Z. Popović100% (1)
- Agitation and Delirium at The End of Life: "We Couldn't Manage Him"Документ15 страницAgitation and Delirium at The End of Life: "We Couldn't Manage Him"Ivonne Soledad Che PiñeiroОценок пока нет
- TSRA Review of Cardiothoracic PDFДокумент298 страницTSRA Review of Cardiothoracic PDFGaetano Di GiovanniОценок пока нет
- Current Concepts in BlepharoplastyДокумент11 страницCurrent Concepts in BlepharoplastyRajinder Kumar Bassan100% (1)
- Rheumatology SheetДокумент54 страницыRheumatology Sheetnachwaallam50% (2)
- Cardiac Enzyme StudiesДокумент4 страницыCardiac Enzyme StudiesDara VinsonОценок пока нет
- Pneumonia Case StudyДокумент12 страницPneumonia Case StudyCharisse Joy Cudal100% (7)
- Consult Pro Tips For All Consults: Do Your Own Work Up!!! PulmДокумент2 страницыConsult Pro Tips For All Consults: Do Your Own Work Up!!! PulmGaetano Di GiovanniОценок пока нет
- NCP Disturbed Body ImageДокумент5 страницNCP Disturbed Body ImageAira AlaroОценок пока нет
- High Alert MedicationsДокумент1 страницаHigh Alert MedicationsrsdsОценок пока нет
- ENEMAДокумент37 страницENEMAmftaganas100% (3)
- Panduan Praktik Klinis OsteomielitisДокумент4 страницыPanduan Praktik Klinis OsteomielitisAstri HapsariОценок пока нет
- Conduits For Coronary Bypass: Vein Grafts: Hendrick B Barner, M.D., Emily A Farkas, M.DДокумент12 страницConduits For Coronary Bypass: Vein Grafts: Hendrick B Barner, M.D., Emily A Farkas, M.DGaetano Di GiovanniОценок пока нет
- 12 Week Us Mle ScheduleДокумент5 страниц12 Week Us Mle ScheduleGaetano Di GiovanniОценок пока нет
- (ED, Our Service Etc) Complaining of - We Were Consulted ForДокумент5 страниц(ED, Our Service Etc) Complaining of - We Were Consulted ForGaetano Di GiovanniОценок пока нет
- Pediatrics 1951 Glicklich 859 76Документ20 страницPediatrics 1951 Glicklich 859 76Gaetano Di GiovanniОценок пока нет
- Clinical Questions, PICO, & Study DesignsДокумент3 страницыClinical Questions, PICO, & Study DesignsItan VillalpandoОценок пока нет
- EBNДокумент18 страницEBNRais HasanОценок пока нет
- 5.2 DR - Yusuf Assegaf SPJP - Syok KardiogenikДокумент33 страницы5.2 DR - Yusuf Assegaf SPJP - Syok KardiogenikAfdol Triatmojo SikumbangОценок пока нет
- 68W Perform A Medical Patient AssessmentДокумент6 страниц68W Perform A Medical Patient Assessmentsmith.kevin1420344Оценок пока нет
- Physiotherapy in Pakistan - An OverviewДокумент4 страницыPhysiotherapy in Pakistan - An Overviewicrs_aamir100% (1)
- Introduction To PathologyДокумент13 страницIntroduction To PathologyRhomizal MazaliОценок пока нет
- FluidotherapyДокумент21 страницаFluidotherapyProtantagonist67% (6)
- M5-Y12-OSCE Phase 1 Examiners FeedbackДокумент9 страницM5-Y12-OSCE Phase 1 Examiners FeedbackTanyaNganОценок пока нет
- Whocdscsreph200212 PDFДокумент72 страницыWhocdscsreph200212 PDFIcaii InfotechОценок пока нет
- Colonization V InfectionДокумент1 страницаColonization V InfectionVerina Logito LoОценок пока нет
- Management of Dengue FeverДокумент16 страницManagement of Dengue FeverSupriyati Rahayu0% (1)
- Images of Nurses in MediaДокумент8 страницImages of Nurses in MediaRufus Raj50% (2)
- Drug Accountability - An Important Aspect of Clinical ResearchДокумент15 страницDrug Accountability - An Important Aspect of Clinical ResearchTrialJoinОценок пока нет
- NCM 107 BДокумент3 страницыNCM 107 BGelain Joyce OrculloОценок пока нет
- Ethics and Medical CommunicationДокумент1 страницаEthics and Medical CommunicationZelffullОценок пока нет
- Bone Ring Autogenous GraftДокумент4 страницыBone Ring Autogenous GraftHub SciОценок пока нет
- TiotropiumДокумент3 страницыTiotropiumLinto JohnОценок пока нет
- Echocardiography (Cardiac Echography, Heart Sonography)Документ2 страницыEchocardiography (Cardiac Echography, Heart Sonography)Broc Il SerbatoioОценок пока нет
- Process of Healthcare For Hip-Surgery PatientsДокумент6 страницProcess of Healthcare For Hip-Surgery PatientsJosipaIvaMarićОценок пока нет
- 9.a Nationwide Evidence-Based Study of Factors Associated With Hospitalizations Due To Unintentional Poisoning and Poisoning Mortality in TaiwanДокумент8 страниц9.a Nationwide Evidence-Based Study of Factors Associated With Hospitalizations Due To Unintentional Poisoning and Poisoning Mortality in Taiwan小葉Оценок пока нет