Вам также может понравиться
- Fracture Healing and BonegraftingДокумент76 страницFracture Healing and BonegraftingJio AmurОценок пока нет
- Week 6 Bone Case StudyДокумент7 страницWeek 6 Bone Case StudyAndriОценок пока нет
- 3 Bone Injury InflammationДокумент24 страницы3 Bone Injury InflammationGwyneth Koleen LopezОценок пока нет
- Ch6Bone StudentДокумент66 страницCh6Bone Studentbhattiareeba13Оценок пока нет
- Lec. 4 Bone FractureДокумент11 страницLec. 4 Bone Fracturebtwlalbwdy16Оценок пока нет
- Ch6Bone StudentДокумент67 страницCh6Bone Studentbhattiareeba13Оценок пока нет
- Complication of FractureДокумент18 страницComplication of FractureJoni NeohОценок пока нет
- Ossification: Ossification (Or Osteogenesis) in Bone Remodeling Is TheДокумент3 страницыOssification: Ossification (Or Osteogenesis) in Bone Remodeling Is TheAlan FosterОценок пока нет
- A Bone Fracture... ZarateДокумент8 страницA Bone Fracture... ZarateRose SalviejoОценок пока нет
- Orthopaedic SlidesДокумент163 страницыOrthopaedic SlidesVivian ChepkemeiОценок пока нет
- Chapter 13Документ27 страницChapter 13Zaky DavidiaОценок пока нет
- Avascular Necrosis: Necrosis Blood Supply JointДокумент9 страницAvascular Necrosis: Necrosis Blood Supply JointAyaba RoselynОценок пока нет
- Jurnal Bone DevelopmentДокумент24 страницыJurnal Bone DevelopmentBuramukanОценок пока нет
- Fracture Healing in Cortical and Cancellous BoneДокумент63 страницыFracture Healing in Cortical and Cancellous BonePramod Thottimane0% (1)
- Fracture: BY: Ma. Elizabeth C. JardiolinДокумент47 страницFracture: BY: Ma. Elizabeth C. JardiolinEdmonLagartoОценок пока нет
- Musculoskeletal Pathology NotesДокумент20 страницMusculoskeletal Pathology Notesdinia fitrianiОценок пока нет
- Musculoskeletal Pathology Notes PDFДокумент20 страницMusculoskeletal Pathology Notes PDFvevestephaniОценок пока нет
- Bones and Soft Tissue - Clinical GateДокумент10 страницBones and Soft Tissue - Clinical GateAkira MasumiОценок пока нет
- Pathology of Fructure & OsteoprosisДокумент3 страницыPathology of Fructure & OsteoprosisYogi drОценок пока нет
- Fracture HealingДокумент22 страницыFracture Healingsumitbhosale3Оценок пока нет
- DR Himanshu Gaur: Consultant Orthopaedic, Joint Replacement & Arthroscopy (Sports Injury) Surgeon BCIMS, New DelhiДокумент34 страницыDR Himanshu Gaur: Consultant Orthopaedic, Joint Replacement & Arthroscopy (Sports Injury) Surgeon BCIMS, New DelhiAnjani Kumar JhaОценок пока нет
- Fracture 01Документ42 страницыFracture 01api-19916399Оценок пока нет
- Fractures and Bone HealingДокумент39 страницFractures and Bone HealingAndreas RendraОценок пока нет
- Fracture Healing and FactorsДокумент29 страницFracture Healing and FactorsVivek ChОценок пока нет
- Pathology of JointsДокумент13 страницPathology of JointswobblegobbleОценок пока нет
- Bone Fracture": Jea N. Daligdig BSN-3Документ7 страницBone Fracture": Jea N. Daligdig BSN-3pjcolitaОценок пока нет
- Bone Healing, Regeneration and Repair: On BiomolecoulerДокумент26 страницBone Healing, Regeneration and Repair: On BiomolecoulerSarah Nabella PutriОценок пока нет
- Orthopedic: Compression FracturesДокумент7 страницOrthopedic: Compression FracturesArianne LaviñaОценок пока нет
- Fracture PresentationДокумент58 страницFracture Presentationshejila c hОценок пока нет
- Fracture HealingДокумент40 страницFracture Healingmohammad farhanОценок пока нет
- Fracture Healing - Basic Science - Orthobullets PDFДокумент2 страницыFracture Healing - Basic Science - Orthobullets PDFMelAcostaОценок пока нет
- 2) Development and Growth of The BonesДокумент3 страницы2) Development and Growth of The BonesAris PaparisОценок пока нет
- Bone FractureДокумент26 страницBone FractureNiningRahmaОценок пока нет
- Normal Bone Anatomy and PhysiologyДокумент9 страницNormal Bone Anatomy and PhysiologyElsa GonçalvesОценок пока нет
- Safari - Feb 21, 2024 at 12:17 PM 3Документ1 страницаSafari - Feb 21, 2024 at 12:17 PM 3syansyncОценок пока нет
- BSE Viva v1.0 PDFДокумент173 страницыBSE Viva v1.0 PDFKavivarma Raj RajendranОценок пока нет
- Fracture and Joint Injuries-General FeaturesДокумент19 страницFracture and Joint Injuries-General Featuresngurah123456789Оценок пока нет
- Disorders of BonesДокумент3 страницыDisorders of BonesAnonymous 0pSLjJYОценок пока нет
- Fractures BasicДокумент10 страницFractures BasicAnish BishwakarmaОценок пока нет
- Bilateral OsteoarthritisДокумент58 страницBilateral OsteoarthritisMaya VilОценок пока нет
- Pathological FracturesДокумент48 страницPathological FracturesHafidah RakhmatinaОценок пока нет
- Orthopaedics DocumentДокумент131 страницаOrthopaedics DocumentRazvan NegritasОценок пока нет
- Bones As A Living Dynamic TissueДокумент13 страницBones As A Living Dynamic TissueSanish Basnet100% (1)
- Bone Fracture HealingДокумент13 страницBone Fracture HealingMustafa HasanОценок пока нет
- Stages of Fracture HealingДокумент5 страницStages of Fracture HealingNnaa LlppОценок пока нет
- Bone FracturesДокумент26 страницBone FracturesgwynОценок пока нет
- Arnett, T.Документ10 страницArnett, T.Alex AmorimОценок пока нет
- LID201112052004Документ10 страницLID201112052004Gia BảoОценок пока нет
- Bone Development: Osteogenesis (Ossification) Endochondral OssificationДокумент2 страницыBone Development: Osteogenesis (Ossification) Endochondral OssificationVanshika SethiОценок пока нет
- Bone Healing Radiology of Normal and Diseased BoneДокумент40 страницBone Healing Radiology of Normal and Diseased BoneAhmed SalmanОценок пока нет
- All About FractureДокумент59 страницAll About FractureJohn John Torres100% (1)
- Lo MSK 2-2Документ14 страницLo MSK 2-2FirmanHidayatОценок пока нет
- Salter Chapter XVДокумент16 страницSalter Chapter XVSamuel Pola Karta SembiringОценок пока нет
- FRACTURESДокумент85 страницFRACTURESSteven OdhiamboОценок пока нет
- Avn On ScriptДокумент13 страницAvn On Scriptclaire.deveraОценок пока нет
- Os 1 251Документ7 страницOs 1 251mukhlis akmalОценок пока нет
- Cartilage Forming TumorsДокумент10 страницCartilage Forming TumorsRavikiran NandirajuОценок пока нет
- K32 - Pathology of Bone (Dr. Dody)Документ60 страницK32 - Pathology of Bone (Dr. Dody)faris100% (1)
- Orthopaedics and Trauma for Medical Students and Junior ResidentsОт EverandOrthopaedics and Trauma for Medical Students and Junior ResidentsРейтинг: 5 из 5 звезд5/5 (3)
- Table 55.: Percentage According To The Type of Seminar/TrainingДокумент6 страницTable 55.: Percentage According To The Type of Seminar/TrainingJaysellePuguonTabijeОценок пока нет
- Generic Name: Indications: Adverse EffectsДокумент6 страницGeneric Name: Indications: Adverse EffectsJaysellePuguonTabijeОценок пока нет
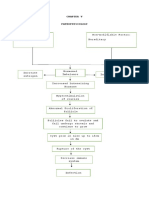
- Pathophysiology of Alzheimers DiseaseДокумент2 страницыPathophysiology of Alzheimers DiseaseJaysellePuguonTabijeОценок пока нет
- Tang Nang EnglishДокумент7 страницTang Nang EnglishJaysellePuguonTabijeОценок пока нет
- C. Expense BudgetДокумент2 страницыC. Expense BudgetJaysellePuguonTabijeОценок пока нет
- TABIJEdiagnosticДокумент2 страницыTABIJEdiagnosticJaysellePuguonTabijeОценок пока нет
- Tabije, Arvie Jayselle PДокумент8 страницTabije, Arvie Jayselle PJaysellePuguonTabijeОценок пока нет
- Bio DataДокумент2 страницыBio DataJaysellePuguonTabijeОценок пока нет
- Mr. Alinger: Mr. Hamza Mr. Marco Mr. Ken Mr. DanielДокумент4 страницыMr. Alinger: Mr. Hamza Mr. Marco Mr. Ken Mr. DanielJaysellePuguonTabijeОценок пока нет
- TABIJEact 7Документ1 страницаTABIJEact 7JaysellePuguonTabijeОценок пока нет
- Educating The Next Generation of Nurses To Be Innovators and Change AgentsДокумент3 страницыEducating The Next Generation of Nurses To Be Innovators and Change AgentsJaysellePuguonTabijeОценок пока нет
- Bio DataДокумент2 страницыBio DataJaysellePuguonTabijeОценок пока нет
- The 4 AДокумент3 страницыThe 4 AJaysellePuguonTabijeОценок пока нет
- APF HandoutsДокумент2 страницыAPF HandoutsJaysellePuguonTabijeОценок пока нет
- Pathophysiology of Heart FailureДокумент2 страницыPathophysiology of Heart FailureJaysellePuguonTabijeОценок пока нет
- Surgical Ward ExamДокумент8 страницSurgical Ward ExamJaysellePuguonTabijeОценок пока нет
- Drug Study: Tabije, Arvie Jayselle P. Marbella, IvyДокумент15 страницDrug Study: Tabije, Arvie Jayselle P. Marbella, IvyJaysellePuguonTabijeОценок пока нет
- Acute Pulmonary Failure: Symptoms and Signs AreДокумент2 страницыAcute Pulmonary Failure: Symptoms and Signs AreJaysellePuguonTabijeОценок пока нет
- Tabije, Arvie Jayselle P. Ncenhl07: Drug Data Drug Action Nursing InterventionsДокумент3 страницыTabije, Arvie Jayselle P. Ncenhl07: Drug Data Drug Action Nursing InterventionsJaysellePuguonTabijeОценок пока нет
- Chapter VДокумент1 страницаChapter VJaysellePuguonTabijeОценок пока нет
- Tabije, Arvie Jayselle P.: Ncenho3 - NcaДокумент3 страницыTabije, Arvie Jayselle P.: Ncenho3 - NcaJaysellePuguonTabijeОценок пока нет
- Case Pres AutosavedДокумент21 страницаCase Pres AutosavedJaysellePuguonTabijeОценок пока нет
- Ramilo, Sheena Patricia M. Ncenh06Документ4 страницыRamilo, Sheena Patricia M. Ncenh06JaysellePuguonTabijeОценок пока нет
- This Is It PancitДокумент50 страницThis Is It PancitJaysellePuguonTabijeОценок пока нет
- 'THE 4 A's OF Alzheimer'S Disease'': Tabije, Arvie Jayselle P. NCB-, BSN-3 Ma'Am Ivy MarbellaДокумент3 страницы'THE 4 A's OF Alzheimer'S Disease'': Tabije, Arvie Jayselle P. NCB-, BSN-3 Ma'Am Ivy MarbellaJaysellePuguonTabijeОценок пока нет
- Name of Drug Mechanism of Action Indications Side Effects Nursing ConsiderationsДокумент9 страницName of Drug Mechanism of Action Indications Side Effects Nursing ConsiderationsJaysellePuguonTabije100% (1)
- TIONGSANДокумент1 страницаTIONGSANJaysellePuguonTabijeОценок пока нет
- Urinary System and Disorders IntroductionДокумент23 страницыUrinary System and Disorders IntroductionHananya ManroeОценок пока нет
- Sample Test Questions For The CPC ExamДокумент8 страницSample Test Questions For The CPC ExamHarikaSabbineniОценок пока нет
- Final 2016 ResumeДокумент4 страницыFinal 2016 Resumeapi-311457885Оценок пока нет
- Ventilation: Kinematics and Kinetics.: Thorax Structure and FunctionДокумент52 страницыVentilation: Kinematics and Kinetics.: Thorax Structure and FunctionAlejandra RomeroОценок пока нет
- Hyperspectral Plant Disease Forecasting Using Generative Adversarial NetworksДокумент4 страницыHyperspectral Plant Disease Forecasting Using Generative Adversarial NetworksaОценок пока нет
- Case Study: Ang Kwento Ni RosarioДокумент2 страницыCase Study: Ang Kwento Ni RosarioVerloren MorgensternОценок пока нет
- Objectives: Terms of Use Privacy Policy Notice AccessibilityДокумент16 страницObjectives: Terms of Use Privacy Policy Notice AccessibilityJuan Sebas OspinaОценок пока нет
- Tapping Into Body Joy PDFДокумент18 страницTapping Into Body Joy PDFKaren McLaughlin100% (13)
- Laboratory Procedure Protocols For Parasitological Sample Collection ProcessingДокумент36 страницLaboratory Procedure Protocols For Parasitological Sample Collection ProcessingDr.Kedar Karki ,M.V.Sc.Preventive Vet.Medicine CLSU Philippines100% (4)
- Genu Valgum Treatment & SurgeryДокумент17 страницGenu Valgum Treatment & SurgeryRanadaPrasadSahaОценок пока нет
- 2019 ACC AHA Guidelines For Primary Prevention of CV DiseaseДокумент39 страниц2019 ACC AHA Guidelines For Primary Prevention of CV DiseaseArdel RomeroОценок пока нет
- Review of Related LiteratureДокумент9 страницReview of Related LiteratureJean Calubag CatalanОценок пока нет
- Summer 2122 Aubf Lab Periodical Test 2Документ38 страницSummer 2122 Aubf Lab Periodical Test 2RuchieОценок пока нет
- Nursing Skills (Vital Signs) PDFДокумент48 страницNursing Skills (Vital Signs) PDFkhizer hayatОценок пока нет
- Sadp Mangosteen Report - 111109Документ23 страницыSadp Mangosteen Report - 111109Ulysses J. Lustria Jr.100% (2)
- Pathophysiology: United StatesДокумент11 страницPathophysiology: United StatesNurullia RahmawatiОценок пока нет
- CVBD Easy-To-Digest No 4 BabesiosisДокумент12 страницCVBD Easy-To-Digest No 4 BabesiosisDocОценок пока нет
- Phylum PlatyhelminthesДокумент19 страницPhylum PlatyhelminthesBudi AfriyansyahОценок пока нет
- Sabutamol SalbutamolДокумент2 страницыSabutamol SalbutamolAnanda Felton FalconОценок пока нет
- RCSI Bahrain ConnectED Newsletter Winter 2022-23Документ32 страницыRCSI Bahrain ConnectED Newsletter Winter 2022-23Yousif YousifОценок пока нет
- Toxoplasma GondiiДокумент7 страницToxoplasma GondiiDedy SavradinataОценок пока нет
- Laboratory Tests InterpretationДокумент12 страницLaboratory Tests InterpretationKaloy Kamao100% (1)
- NRC Guidelines GujrathДокумент68 страницNRC Guidelines GujrathNirajkumar KondekarОценок пока нет
- Health Crisis Slams Disney, But More Bloodletting Ahead: For Personal, Non-Commercial Use OnlyДокумент30 страницHealth Crisis Slams Disney, But More Bloodletting Ahead: For Personal, Non-Commercial Use OnlyMiguel DiazОценок пока нет
- Autoimmune Abnormalities of Postpartum Thyroid DiseasesДокумент8 страницAutoimmune Abnormalities of Postpartum Thyroid DiseasesIpan MahendriyansaОценок пока нет
- The Chemical Composition and Pharmaceutical Effect of Celosia Cristata A Review On Nutritional AspectДокумент6 страницThe Chemical Composition and Pharmaceutical Effect of Celosia Cristata A Review On Nutritional AspectInternational Journal of Innovative Science and Research TechnologyОценок пока нет
- Air PalutionДокумент13 страницAir PalutionArabinda ParidaОценок пока нет
- Pa Tho Physiology of Hemorrhagic StrokeДокумент2 страницыPa Tho Physiology of Hemorrhagic StrokeMerlash MerlaОценок пока нет
- SaponinesДокумент3 страницыSaponinesCorinaОценок пока нет