Вам также может понравиться
- Item 6f - Acute Management of Hyperosmolar Hyperglycaemic StateДокумент1 страницаItem 6f - Acute Management of Hyperosmolar Hyperglycaemic StateStef AnОценок пока нет
- Dka CalculatorДокумент1 страницаDka CalculatordelfiaОценок пока нет
- DKA Guidelines Version 4.0 28 Dec 2016FINALДокумент4 страницыDKA Guidelines Version 4.0 28 Dec 2016FINALbenОценок пока нет
- DKACalculatorДокумент1 страницаDKACalculatorRitch BassОценок пока нет
- Kuwait PICU Taskforce DKA V1 5 June 2022Документ2 страницыKuwait PICU Taskforce DKA V1 5 June 2022Emad MashaalОценок пока нет
- TWU Anesthesia Cheat SheetДокумент2 страницыTWU Anesthesia Cheat Sheetinvading_jam7582100% (5)
- Hyperglycaemic Emergencies Inpatient Draft-1-3Документ13 страницHyperglycaemic Emergencies Inpatient Draft-1-3Cik JaaОценок пока нет
- Fluid and Electrolytes ManagementДокумент21 страницаFluid and Electrolytes ManagementRasYa DIОценок пока нет
- Management of Anesthesia: Diabetes MellitusДокумент29 страницManagement of Anesthesia: Diabetes MellitusHari PrasadОценок пока нет
- Electrolyte Disturbance Quick GuideДокумент11 страницElectrolyte Disturbance Quick GuideTianaОценок пока нет
- DM Diabetic Ketoacidosis DKA Management Algorithm Adult Patients 2019Документ1 страницаDM Diabetic Ketoacidosis DKA Management Algorithm Adult Patients 2019Hendra AfrilaОценок пока нет
- Adult Diabetic Ketoacidosis DKA Guideline South WestДокумент6 страницAdult Diabetic Ketoacidosis DKA Guideline South Westshada aaaОценок пока нет
- DKA Management-2Документ7 страницDKA Management-2NisaОценок пока нет
- Acid Base 7 2Документ31 страницаAcid Base 7 2sarvathaqaryОценок пока нет
- ENDOCRINE-BOARD REVIEW Dr. SchearДокумент57 страницENDOCRINE-BOARD REVIEW Dr. SchearNayara PataroОценок пока нет
- Fluitest Glu HK: Glucose Hexokinase 100+1Документ4 страницыFluitest Glu HK: Glucose Hexokinase 100+1akaweadeОценок пока нет
- Acute Metabolic Complications of Diabetes MellitusДокумент54 страницыAcute Metabolic Complications of Diabetes MellitusPrincewill SeiyefaОценок пока нет
- 205 Management of Hypo Kala Emi AДокумент11 страниц205 Management of Hypo Kala Emi AGresonОценок пока нет
- DKA PosterДокумент2 страницыDKA PosterainizatiОценок пока нет
- Dka AlgorithmДокумент1 страницаDka AlgorithmAbhinav AggarwalОценок пока нет
- Diabetes MellitusДокумент20 страницDiabetes MellitusNICHOLAS KAUMBAОценок пока нет
- Adult: Diabetic Emergencies: Care Protocol and ChartДокумент4 страницыAdult: Diabetic Emergencies: Care Protocol and ChartvladhdОценок пока нет
- DKA ModifiedДокумент25 страницDKA ModifiedSujit KoiralaОценок пока нет
- Guideline For The Management of Hypokalaemia in Adults: Signs & SymptomsДокумент2 страницыGuideline For The Management of Hypokalaemia in Adults: Signs & SymptomsmuzakiОценок пока нет
- Hypokalaemia PDFДокумент2 страницыHypokalaemia PDFManuela KarinaaОценок пока нет
- Hypokalaemia PDFДокумент2 страницыHypokalaemia PDFRisaОценок пока нет
- Hypokalaemia PDFДокумент2 страницыHypokalaemia PDFjenna1213Оценок пока нет
- Hypokalaemia PDFДокумент2 страницыHypokalaemia PDFIulia RoxanaОценок пока нет
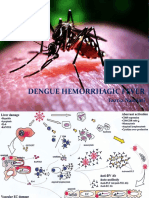
- Dengue Hemorrhagic Fever: Fazria NasriatiДокумент19 страницDengue Hemorrhagic Fever: Fazria NasriatiElsa KarinasariОценок пока нет
- Acute Diabetic Ketoacidosis (DKA)Документ21 страницаAcute Diabetic Ketoacidosis (DKA)Madhu Sudhan Pandeya0% (1)
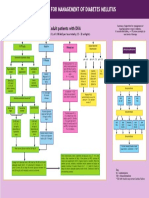
- Guideline For The Management of Adults Patients With DKA or HHSДокумент3 страницыGuideline For The Management of Adults Patients With DKA or HHSJonard GiloОценок пока нет
- Guideline Title: Management of Diabetic KetoacidosisДокумент9 страницGuideline Title: Management of Diabetic KetoacidosisJorge Salazar GomezОценок пока нет
- Commonly Prescribed Medications in Surgical Ed Sivakami Ver 5.0Документ23 страницыCommonly Prescribed Medications in Surgical Ed Sivakami Ver 5.0Suiweng WongОценок пока нет
- Inpatient Electrolyte RepletionДокумент3 страницыInpatient Electrolyte Repletionapi-648757084Оценок пока нет
- Coma Hyperglycemic Hyperosmolar NonketoticДокумент10 страницComa Hyperglycemic Hyperosmolar NonketoticD An0% (1)
- Early Symptoms: Insidious Increase in Polydipsia and PolyuriaДокумент3 страницыEarly Symptoms: Insidious Increase in Polydipsia and Polyuriabes3rkerОценок пока нет
- Revised DKA 2015 PDFДокумент6 страницRevised DKA 2015 PDFDr AhmedОценок пока нет
- JBDS 02 Single Page Pathway Amended June 2021Документ2 страницыJBDS 02 Single Page Pathway Amended June 2021Oliverio MéndezОценок пока нет
- Ed Adult and PaedsДокумент2 страницыEd Adult and PaedsPrashin RocharamОценок пока нет
- Treatment of Acute Hypokalaemia in AdultsДокумент4 страницыTreatment of Acute Hypokalaemia in AdultsEmaОценок пока нет
- Icu Adult and PaedsДокумент2 страницыIcu Adult and PaedsPrashin RocharamОценок пока нет
- Mayo Clinic Laboratories Critical Values / Critical Results ListДокумент4 страницыMayo Clinic Laboratories Critical Values / Critical Results ListCarl DonaireОценок пока нет
- Hyperkalemia - ClinicalKeyДокумент19 страницHyperkalemia - ClinicalKeyBejinaruOanaSiCristiОценок пока нет
- Diabetic Ketoacidosis Dka Hyperglycemic Hyperosmolar State Hhs Adult PDFДокумент4 страницыDiabetic Ketoacidosis Dka Hyperglycemic Hyperosmolar State Hhs Adult PDFyayaОценок пока нет
- Acute Complications of DM ESS 2016Документ41 страницаAcute Complications of DM ESS 2016teodordragnev1Оценок пока нет
- Chol PDFДокумент1 страницаChol PDFTaqien AbscОценок пока нет
- Hyperglycemia, HHS, DKAДокумент30 страницHyperglycemia, HHS, DKAFirdausОценок пока нет
- DKA Handout1Документ59 страницDKA Handout1aleОценок пока нет
- Pass Critical Care Endocrine Frcem ResourcesДокумент41 страницаPass Critical Care Endocrine Frcem ResourcesYoussef SaadОценок пока нет
- Calcio Ca A IiiДокумент4 страницыCalcio Ca A IiiCristian LaraОценок пока нет
- Map DkaДокумент1 страницаMap DkaSH PrageethОценок пока нет
- Electrolyte Prescribe Gline AdultДокумент2 страницыElectrolyte Prescribe Gline AdultMirelaОценок пока нет
- Treating and Monitoring Hypomagnesaemia For Non-Critical Areas of TrustДокумент3 страницыTreating and Monitoring Hypomagnesaemia For Non-Critical Areas of Trustramy.elantaryОценок пока нет
- 173 CT10360Документ2 страницы173 CT10360thureinwinnОценок пока нет
- Pediatric Diabetic Ketoacidosis (DKA) Algorithm (Page 1-ED) : DKA Diagnosed DKA Not DiagnosedДокумент2 страницыPediatric Diabetic Ketoacidosis (DKA) Algorithm (Page 1-ED) : DKA Diagnosed DKA Not Diagnosedrolland_arrizaОценок пока нет
- Condition Formula IV Fluid Acute Gastroenteritis A. Severe Acute Malnutrition (SAM) Source: WHO?? 1. in ShockДокумент4 страницыCondition Formula IV Fluid Acute Gastroenteritis A. Severe Acute Malnutrition (SAM) Source: WHO?? 1. in ShockJohnPaulOliverosОценок пока нет
- Penatalaksanan Intensif Pasien Dengan Penyakit Tropik Berat Di ICUДокумент24 страницыPenatalaksanan Intensif Pasien Dengan Penyakit Tropik Berat Di ICUedelinОценок пока нет
- Diabetic Ketoacidosis PathwayДокумент22 страницыDiabetic Ketoacidosis PathwaySri Nath100% (1)
- Diabetic Ketoacidosis (D.K.A) Beaumont Hospital Protocol: DiagnosisДокумент1 страницаDiabetic Ketoacidosis (D.K.A) Beaumont Hospital Protocol: Diagnosislouglee9174100% (1)
- The Smart Chiropractor A Guide To Marketing Your PracticeДокумент43 страницыThe Smart Chiropractor A Guide To Marketing Your PracticeAaron DriverОценок пока нет
- Protocolo Cochrane REHABILITACIÓN COGNITIVA en Demencia (2019)Документ17 страницProtocolo Cochrane REHABILITACIÓN COGNITIVA en Demencia (2019)Sara Daoudi FuentesОценок пока нет
- Gingival Biotype and Its Clinical Significance A ReviewДокумент5 страницGingival Biotype and Its Clinical Significance A ReviewMilton Castillo CaceresОценок пока нет
- Jason Case StudyДокумент2 страницыJason Case StudyLLLJJJОценок пока нет
- Medical Prefixes and Suffixes and English Roots - 2003Документ28 страницMedical Prefixes and Suffixes and English Roots - 2003Nada SaviraОценок пока нет
- Jurnal Remifentanyl For Pain LaborДокумент11 страницJurnal Remifentanyl For Pain LaborAshadi CahyadiОценок пока нет
- Pathophysiology of Pain in BiliodigestiДокумент19 страницPathophysiology of Pain in Biliodigestiprabowoaji12Оценок пока нет
- Who NMH Nvi 18.3 EngДокумент41 страницаWho NMH Nvi 18.3 EngZenard de la CruzОценок пока нет
- Impact On Employee Workplace Organization of Covid 19Документ90 страницImpact On Employee Workplace Organization of Covid 19salmanОценок пока нет
- 3A - Hospital PharmacyДокумент13 страниц3A - Hospital PharmacyekramОценок пока нет
- Sexually Transmitted Infections StisДокумент2 страницыSexually Transmitted Infections Stisapi-646865632Оценок пока нет
- Psychiatric TriageДокумент30 страницPsychiatric TriageastroirmaОценок пока нет
- (Ped-W1) (Dr. Zuhair M. Al Musawi) Repiratory 2Документ43 страницы(Ped-W1) (Dr. Zuhair M. Al Musawi) Repiratory 2Haider Nadhem AL-rubaiОценок пока нет
- How Well Are You Thinking?: Self Administered Gerocognitive Examination - SAGEДокумент5 страницHow Well Are You Thinking?: Self Administered Gerocognitive Examination - SAGEJhon LockeОценок пока нет
- Ca BladderДокумент11 страницCa Bladdersalsabil aurellОценок пока нет
- Clinical Avian Medicine - 2 Volume Set PDFДокумент1 057 страницClinical Avian Medicine - 2 Volume Set PDFSilvana Martinez100% (3)
- Forensic MedicineДокумент21 страницаForensic Medicineritika100% (3)
- MTY1215 Hematology 2 (Lec) HandoutsДокумент7 страницMTY1215 Hematology 2 (Lec) HandoutsDarren Gabriel NicolasОценок пока нет
- Sujok Global MagazineДокумент52 страницыSujok Global MagazineNidhi ShahОценок пока нет
- OligohydramniosДокумент4 страницыOligohydramniossalamredОценок пока нет
- 2011 Complete Journals Catalog (Incl Open Access Journals)Документ292 страницы2011 Complete Journals Catalog (Incl Open Access Journals)mourighoshОценок пока нет
- Hipertensi PBLДокумент56 страницHipertensi PBLVandra PrinosaОценок пока нет
- General Paper September 2020Документ26 страницGeneral Paper September 2020Kumah Wisdom100% (1)
- Anti Dumping DietДокумент3 страницыAnti Dumping DietFelixDrummaruОценок пока нет
- Comm Dent MCQДокумент8 страницComm Dent MCQoss-20502745Оценок пока нет
- Office of The Information and Privacy Commissioner of Alberta - Public Inquiry 005994, University of Alberta Freedom of Information RequestДокумент60 страницOffice of The Information and Privacy Commissioner of Alberta - Public Inquiry 005994, University of Alberta Freedom of Information RequestWilliam Makis100% (3)
- The Reconstruction of Pink and White Esthetics: ClinicalДокумент4 страницыThe Reconstruction of Pink and White Esthetics: ClinicalPreventiva HRACОценок пока нет
- Family Centered CareДокумент7 страницFamily Centered CareSirisha ChelvaОценок пока нет
- HemolysisДокумент22 страницыHemolysisMohamoud MohamedОценок пока нет