Вам также может понравиться
- Integrative Dual Diagnosis Treatment Approach to an Individual with Alcoholism and Coexisting Endogenous DepressionОт EverandIntegrative Dual Diagnosis Treatment Approach to an Individual with Alcoholism and Coexisting Endogenous DepressionРейтинг: 2 из 5 звезд2/5 (1)
- Psychiatric Diagnosis: Challenges and ProspectsОт EverandPsychiatric Diagnosis: Challenges and ProspectsIhsan M. SalloumРейтинг: 5 из 5 звезд5/5 (1)
- Nursing Care of The Patient With Schizophrenia & Psychosis F20Документ47 страницNursing Care of The Patient With Schizophrenia & Psychosis F20nidhi PatelОценок пока нет
- Emotional Competence: The Fountain of personal, professional and private SuccessОт EverandEmotional Competence: The Fountain of personal, professional and private SuccessОценок пока нет
- Racism and Psychiatry: Contemporary Issues and InterventionsОт EverandRacism and Psychiatry: Contemporary Issues and InterventionsMorgan M. MedlockОценок пока нет
- Fome - Family Dynamics PDFДокумент21 страницаFome - Family Dynamics PDFfarhanomeОценок пока нет
- Hereditary Hemochromatosis? and Vitamin D Deficiency from Uvb Radiation (Sunlight) Originating from Northern Europe: The Cause of Multiple SclerosisОт EverandHereditary Hemochromatosis? and Vitamin D Deficiency from Uvb Radiation (Sunlight) Originating from Northern Europe: The Cause of Multiple SclerosisОценок пока нет
- 2b - Personality DisordersДокумент27 страниц2b - Personality DisordersaldreinОценок пока нет
- Cognitive and Behavioral Interventions in the Schools: Integrating Theory and Research into PracticeОт EverandCognitive and Behavioral Interventions in the Schools: Integrating Theory and Research into PracticeRosemary FlanaganОценок пока нет
- The Slim Book of Health Pearls: Hormones, Nerves, and StressОт EverandThe Slim Book of Health Pearls: Hormones, Nerves, and StressОценок пока нет
- Personality and Arousal: A Psychophysiological Study of Psychiatric DisorderОт EverandPersonality and Arousal: A Psychophysiological Study of Psychiatric DisorderОценок пока нет
- Privacy and Confidentiality Standards in Forensic PsychologyДокумент12 страницPrivacy and Confidentiality Standards in Forensic PsychologyBonnieОценок пока нет
- Disorders of the Patellofemoral Joint: Diagnosis and ManagementОт EverandDisorders of the Patellofemoral Joint: Diagnosis and ManagementОценок пока нет
- Medical Conditions Associated with Suicide Risk: Suicide and Spinal Cord InjuryОт EverandMedical Conditions Associated with Suicide Risk: Suicide and Spinal Cord InjuryОценок пока нет
- Group Medical Appointments: An Introduction for Health ProfessionalsОт EverandGroup Medical Appointments: An Introduction for Health ProfessionalsРейтинг: 5 из 5 звезд5/5 (1)
- Alzheimeru2019s DiseaseДокумент17 страницAlzheimeru2019s Diseaseapi-262538456100% (1)
- Guilt and ChildrenОт EverandGuilt and ChildrenJane BybeeОценок пока нет
- Amnesia: Clinical, Psychological and Medicolegal AspectsОт EverandAmnesia: Clinical, Psychological and Medicolegal AspectsC. W. M. WhittyОценок пока нет
- Defense Mechanism PracticeДокумент3 страницыDefense Mechanism PracticeLaura MОценок пока нет
- Test Bank For Psychiatric Mental Health Nursing 1st Edition by PotterДокумент38 страницTest Bank For Psychiatric Mental Health Nursing 1st Edition by Potterlionelhuynhg7cОценок пока нет
- Teenage Health Concerns: How Parents Can Manage Eating Disorders In Teenage ChildrenОт EverandTeenage Health Concerns: How Parents Can Manage Eating Disorders In Teenage ChildrenОценок пока нет
- Mental DisordersДокумент12 страницMental DisordersCiara C.Оценок пока нет
- Treatment and Prevention of Alcohol Problems: A Resource ManualОт EverandTreatment and Prevention of Alcohol Problems: A Resource ManualОценок пока нет
- Stages of DevelopmentДокумент2 страницыStages of Developmentdi na babalikОценок пока нет
- Assessment of Personality DisorderДокумент9 страницAssessment of Personality DisorderTauqeer AhmedОценок пока нет
- The Wiley-Blackwell Handbook of Addiction PsychopharmacologyОт EverandThe Wiley-Blackwell Handbook of Addiction PsychopharmacologyОценок пока нет
- Schizophrenia: Depression, Hallucinations, Symptoms, and SolutionsОт EverandSchizophrenia: Depression, Hallucinations, Symptoms, and SolutionsОценок пока нет
- Ganser SyndromeДокумент3 страницыGanser Syndromesomebody_maОценок пока нет
- PSYB32 Final Exam ReviewДокумент29 страницPSYB32 Final Exam Reviewraeesah9171Оценок пока нет
- Defense Mechanism: Drvksahu Resident PsychiatryДокумент74 страницыDefense Mechanism: Drvksahu Resident PsychiatryMudassar HussainОценок пока нет
- Doctrine of Double Effect Stanford Encyclopedia of PhilosophyДокумент9 страницDoctrine of Double Effect Stanford Encyclopedia of PhilosophyCarlos TrОценок пока нет
- Schizophrenia: Vaisnvi Muthoovaloo 102011430Документ18 страницSchizophrenia: Vaisnvi Muthoovaloo 102011430Vaisnavi MuthoovalooОценок пока нет
- Developing Images: Mind Development, Hallucinations and All Mind Disorders Including AutismОт EverandDeveloping Images: Mind Development, Hallucinations and All Mind Disorders Including AutismОценок пока нет
- 2013 History Taking - and Examination For UGДокумент75 страниц2013 History Taking - and Examination For UGsmitha manjunathОценок пока нет
- Maladaptive Patterns of BehaviorДокумент97 страницMaladaptive Patterns of BehaviorKimTot OctavianoОценок пока нет
- Introduction To Psychiatric Nursing: Mercedes A Perez-Millan MSN, ARNPДокумент33 страницыIntroduction To Psychiatric Nursing: Mercedes A Perez-Millan MSN, ARNPSachiko Yosores100% (1)
- Schizophrenia and Biblical Counseling Notes Doc-DrДокумент4 страницыSchizophrenia and Biblical Counseling Notes Doc-DrJulio Cezar de Pinho Jr.Оценок пока нет
- Terminology of PsychiatryДокумент6 страницTerminology of PsychiatryHassan.shehri100% (1)
- Mental Status EvaluationДокумент7 страницMental Status Evaluationmunir houseОценок пока нет
- Maximizing Pain Management in Cancer Patients - DR Ungku KamariahДокумент36 страницMaximizing Pain Management in Cancer Patients - DR Ungku Kamariahmalaysianhospicecouncil6240Оценок пока нет
- List of PhobiasДокумент5 страницList of PhobiasRyan SanchezОценок пока нет
- New Disorder - 1Документ148 страницNew Disorder - 1max lifeОценок пока нет
- The Biological and Evolutionary Bases of BehaviorДокумент77 страницThe Biological and Evolutionary Bases of Behaviorbill100% (1)
- Neurotransmitters: A. Paracrine Regulators (Tissue Hormones)Документ11 страницNeurotransmitters: A. Paracrine Regulators (Tissue Hormones)Prasana100% (1)
- Phobias LectureДокумент28 страницPhobias Lectureanon_473291823100% (1)
- Varcarolis CH 1Документ21 страницаVarcarolis CH 1Catlyn ChatpmanОценок пока нет
- Lea - Materials Police Org 2021Документ12 страницLea - Materials Police Org 2021Lloyd Rafael EstabilloОценок пока нет
- Industrial Security Management: Arete Review & Tutorial CenterДокумент8 страницIndustrial Security Management: Arete Review & Tutorial CenterLloyd Rafael EstabilloОценок пока нет
- 1st 1000 Days PDFДокумент36 страниц1st 1000 Days PDFLloyd Rafael EstabilloОценок пока нет
- CHN - Module 1Документ10 страницCHN - Module 1Lloyd Rafael EstabilloОценок пока нет
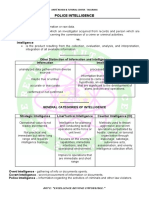
- Lea Police Intelligence FinalДокумент9 страницLea Police Intelligence FinalLloyd Rafael EstabilloОценок пока нет
- Growth and DevelopmentДокумент96 страницGrowth and DevelopmentLloyd Rafael EstabilloОценок пока нет
- Medical Surgical NursingДокумент179 страницMedical Surgical NursingLloyd Rafael EstabilloОценок пока нет
- Nursing Practice VДокумент9 страницNursing Practice VLloyd Rafael Estabillo100% (1)
- Basic Nursing PharmacologyДокумент78 страницBasic Nursing PharmacologyLloyd Rafael EstabilloОценок пока нет
- Funda - NursingДокумент29 страницFunda - NursingLloyd Rafael EstabilloОценок пока нет
- Ms Simulated 1Документ18 страницMs Simulated 1Lloyd Rafael Estabillo100% (1)
- Fluids and Electrolytes DrillsДокумент7 страницFluids and Electrolytes DrillsLloyd Rafael EstabilloОценок пока нет
- PsychiaДокумент12 страницPsychiaLloyd Rafael EstabilloОценок пока нет
- Copar: Community Organizing Participatory Action ResearchДокумент21 страницаCopar: Community Organizing Participatory Action ResearchLloyd Rafael EstabilloОценок пока нет
- COPARДокумент21 страницаCOPARLloyd Rafael EstabilloОценок пока нет
- BacteriaДокумент3 страницыBacteriaLloyd Rafael EstabilloОценок пока нет
- Lloyd Rafael Estabillo, RN: Prepared byДокумент13 страницLloyd Rafael Estabillo, RN: Prepared byLloyd Rafael EstabilloОценок пока нет
- IMCIДокумент148 страницIMCILloyd Rafael EstabilloОценок пока нет
- IFC Core CompetencyДокумент7 страницIFC Core CompetencyLloyd Rafael EstabilloОценок пока нет
- You Can Classify That A Child Aged 2 Years Has Fast Breathing If He Has A Respiratory Rate ofДокумент44 страницыYou Can Classify That A Child Aged 2 Years Has Fast Breathing If He Has A Respiratory Rate ofLloyd Rafael Estabillo100% (1)
- Therapeutic CommunicationДокумент4 страницыTherapeutic CommunicationLloyd Rafael Estabillo100% (1)
- Psychiatric NursingДокумент12 страницPsychiatric NursingLloyd Rafael Estabillo100% (1)
- Cdi TrafficДокумент101 страницаCdi TrafficLloyd Rafael EstabilloОценок пока нет
- A Cultural Approach To Male - Female MiscommunicationДокумент10 страницA Cultural Approach To Male - Female MiscommunicationTrần Thục UyênОценок пока нет
- Consumer BehaviourДокумент17 страницConsumer Behaviouradv_jОценок пока нет
- AI & Digital ForensicsДокумент4 страницыAI & Digital ForensicsDery WalieriОценок пока нет
- Mohamed Amine Ichou: ContactДокумент1 страницаMohamed Amine Ichou: ContactMohammed AmineОценок пока нет
- Plural NounsДокумент3 страницыPlural Nounsapi-440080904Оценок пока нет
- Schueler Et Al-2018-Journal of PersonalityДокумент20 страницSchueler Et Al-2018-Journal of PersonalityKasture ManimaranОценок пока нет
- Psychology 3rd Edition Ciccarelli Test BankДокумент6 страницPsychology 3rd Edition Ciccarelli Test Bankrowanariel26r2100% (25)
- Literacy PolicyДокумент5 страницLiteracy PolicyBCCCSОценок пока нет
- How We Express Ourselves - Play 2016-17.PDF UpdatedДокумент11 страницHow We Express Ourselves - Play 2016-17.PDF UpdatedSneha Mishra100% (1)
- Dokumen - Tips Ielts OrientationДокумент33 страницыDokumen - Tips Ielts OrientationblominoqueОценок пока нет
- Interpret SopДокумент2 страницыInterpret SopbjihuhОценок пока нет
- Mathematics Anxiety Kecemasan MatematikaДокумент15 страницMathematics Anxiety Kecemasan MatematikaDodi IsranОценок пока нет
- Quotes - Habits of MindДокумент146 страницQuotes - Habits of MindSudipta BoseОценок пока нет
- Teaching Reading ScoreДокумент3 страницыTeaching Reading Scoreapi-403448804Оценок пока нет
- Diagnostic Test Pract Res 2Документ2 страницыDiagnostic Test Pract Res 2pablito l. suico100% (2)
- EssayДокумент11 страницEssaypopovicanastasia011Оценок пока нет
- This Study Resource WasДокумент1 страницаThis Study Resource WasKyralle Nan AndolanaОценок пока нет
- Guided Reading Plans Dra 50Документ2 страницыGuided Reading Plans Dra 50api-277767090Оценок пока нет
- The Oxford Wordlist Top 500: High Frequency Words in Young Children's Writing and Reading DevelopmentДокумент20 страницThe Oxford Wordlist Top 500: High Frequency Words in Young Children's Writing and Reading DevelopmentFarah MazherОценок пока нет
- Final Requirement - Org DevtДокумент46 страницFinal Requirement - Org Devtjocelyn delgadoОценок пока нет
- Title of The Activity: Emotions: Name: Date - Grade/Section: ScoreДокумент11 страницTitle of The Activity: Emotions: Name: Date - Grade/Section: Scorejeric m. gutierrezОценок пока нет
- 07.2-Belbins Team RolesДокумент22 страницы07.2-Belbins Team RolesibrahimОценок пока нет
- DLP 4.1 - 4.2Документ4 страницыDLP 4.1 - 4.2MlynОценок пока нет
- Planet ProjectДокумент2 страницыPlanet ProjectGreici J. BuzziОценок пока нет
- 3 Theories of Social InstitutionsДокумент16 страниц3 Theories of Social InstitutionsSze Yinn PikaaОценок пока нет
- Name: - Year Level/grade & Section: - SexДокумент1 страницаName: - Year Level/grade & Section: - SexCmc Corpuz AbrisОценок пока нет
- Briefing Note - Assignment Details & RubricДокумент5 страницBriefing Note - Assignment Details & RubricAlwalid WalidОценок пока нет
- Peer Graded AssignmentДокумент3 страницыPeer Graded Assignmentpadma100% (1)
- Teaching Introductory Physics Arnold B AronsДокумент5 страницTeaching Introductory Physics Arnold B AronsGanesh KumarОценок пока нет
- San Pasqual Academy English 9 and 10 - Ms. Priester Future Plans ProjectДокумент12 страницSan Pasqual Academy English 9 and 10 - Ms. Priester Future Plans ProjectdaaiyahnaimОценок пока нет