Академический Документы
Профессиональный Документы
Культура Документы
Tetanus, Botulism, and Diphtheria
Загружено:
night.shadowОригинальное название
Авторское право
Доступные форматы
Поделиться этим документом
Поделиться или встроить документ
Этот документ был вам полезен?
Это неприемлемый материал?
Пожаловаться на этот документАвторское право:
Доступные форматы
Tetanus, Botulism, and Diphtheria
Загружено:
night.shadowАвторское право:
Доступные форматы
Tetanus, Botulism, REVIEW ARTICLE
and Diphtheria C O N T I N U UM A U D I O
I NT E R V I E W A V A I L AB L E
ONLINE
By Aaron L. Berkowitz, MD, PhD
ABSTRACT
PURPOSE OF REVIEW: This article reviews the pathophysiology, epidemiology,
clinical manifestations, diagnosis, and treatment of tetanus, botulism, and
diphtheric neuropathy.
RECENT FINDINGS: Tetanus is most common in lower-income settings, but rare
Downloaded from http://journals.lww.com/continuum by BhDMf5ePHKbH4TTImqenVAHxkFJp/XpPnRCHYLXWr7IoaYaYGhGAx/3d3LgBEn+n on 10/02/2018
cases are seen in higher-income settings because of the inadequate
maintenance of vaccination status. Foodborne botulism remains rare, but
botulism can also be caused by IV drug use (wound botulism) and medical
use of botulinum toxin (iatrogenic botulism); botulinum toxin has also been
considered a potential agent of bioterrorism. Diphtheric neuropathy is rare
but has been seen in recent epidemics in the former Soviet Union, and
vaccination status is inadequate in a significant proportion of older
individuals, creating the potential for subsequent epidemics.
SUMMARY: Tetanus, botulism, and diphtheric neuropathy are rare in
higher-resource settings where most neurologists practice; however,
familiarity with the unique clinical manifestations of and laboratory
evaluation for these disorders is essential for the rapid diagnosis and
treatment of patients with these conditions.
CITE AS:
CONTINUUM (MINNEAP MINN)
2018;24(5, NEUROINFECTIOUS
DISEASE):1459–1488.
INTRODUCTION
T
etanus, botulism, and diphtheric neuropathy are neuromuscular Address correspondence to
Dr Aaron L. Berkowitz,
syndromes caused by bacterial toxins produced by gram-positive
Department of Neurology,
anaerobic bacilli (TABLE 10-1). Tetanus and botulism are primary Brigham and Women’s Hospital,
neurologic disorders, whereas diphtheric neuropathy can occur as a 60 Fenwood Rd, Boston, MA,
02115, aberkowitz3@bwh.
sequela of respiratory diphtheria. The distinct clinical manifestations harvard.edu.
of these three disorders arise from the unique locations of action of their
respective toxins along the neuraxis: tetanus toxin acts at inhibitory interneurons RELATIONSHIP DISCLOSURE:
Dr Berkowitz receives publishing
in the brainstem and spinal cord, botulinum toxin acts at the presynaptic royalties from McGraw-Hill
terminals of the neuromuscular junction (FIGURE 10-1,1 FIGURE 10-21), and Education, MedMaster Inc, and
diphtheria toxin affects protein synthesis in Schwann cells, leading to demyelination Oxford University Press.
of peripheral nerves. Tetanus and diphtheria are vaccine-preventable illnesses, UNLABELED USE OF
whereas botulism is largely preventable through proper food preparation PRODUCTS/INVESTIGATIONAL
USE DISCLOSURE:
practices. Diphtheria is the only contagious illness of the three. Dr Berkowitz reports no
Although rare in high-income countries, tetanus, botulism, and diphtheria disclosure.
continue to occur in lower-income countries. Awareness of the unique features,
management, and prevention of these three conditions is of importance for © 2018 American Academy
neurologists because of the waning vaccine-induced immunity of an aging of Neurology.
CONTINUUMJOURNAL.COM 1459
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
TETANUS, BOTULISM, AND DIPHTHERIA
TABLE 10-1 Comparison of Features of Tetanus, Botulism, and Diphtheric Neuropathy
Tetanus Botulism Diphtheric Neuropathy
Bacterium Clostridium tetani Clostridium botulinum Corynebacterium diphtheriae
Toxin Tetanospasmin Botulinum toxin (types A–G) Diphtheria toxin
Location of Inhibitory interneurons in spinal Presynaptic terminals of Protein synthesis in Schwann cells
toxin action cord and brainstem neuromuscular junction (leading to peripheral nerve
demyelination)
Mode of Wound; operation; injection; Home-canned food, inadequately Human-to-human respiratory
acquisition unhygienic birth, abortion, or refrigerated or cooked food, transmission
umbilical cord practices injection drug use (wound
botulism), honey (infant
botulism), iatrogenic, adult
intestinal colonization
Major clinical Muscular rigidity, painful Classic pentad: dry mouth, Exudative pharyngitis followed
features spasms, trismus, risus nausea/vomiting, dysphagia, weeks later by dysphagia,
sardonicus, opisthotonos, diplopia, fixed dilated pupils; dysphonia; followed weeks later
autonomic instability followed rapidly by extremity by weakness and sensory changes
weakness in the extremities
Diagnosis Clinical Serum or stool culture, toxin Throat culture
identification by mouse-based
assay or enzyme-linked
immunosorbent assay
(ELISA), EMG
Nerve conduction Continuous involuntary Decreased compound muscle Demyelinating polyneuropathy:
study and EMG spontaneous motor activity, action potential (CMAP) slowed conduction velocities,
findings increased F-wave amplitude, amplitudes, decremental prolonged distal latencies,
absence of silent period response to low-frequency conduction block, prolonged F
following peripheral stimulation repetitive stimulation, incremental waves, preserved sensory and
response (facilitation) to motor amplitudes
high-frequency repetitive
stimulation, persistence
of post-tetanic facilitation,
short-duration low-amplitude
motor unit potentials, increased
jitter on single fiber EMG, normal
velocities/latencies
Treatment Antibiotics (metronidazole Antitoxin (infant: human-derived Antibiotics, antitoxin
preferred), tetanus antitoxin, botulism immunoglobulin [BIG-IV];
toxoid vaccination, diazepam adult: heptavalent botulinum
or other benzodiazepine for antitoxin), antibiotics for wound
spasms (neuromuscular botulism only, supportive care
blockade if inadequate), wound
debridement, supportive care
Prevention Vaccination and boosters, Proper food preparation and Vaccination and boosters
wound prophylaxis (refer canning techniques, avoidance
to TABLE 10-2) of honey for infants
EMG = electromyography.
1460 OCTOBER 2018
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
population (tetanus and diphtheria),2 migration from areas with lower KEY POINTS
vaccination rates (tetanus and diphtheria) and unsafe food preparation practices
● Neonatal tetanus is most
(botulism), increasing injection drug use in the setting of the opioid epidemic often due to infection of the
(risk for tetanus and wound botulism), increasing work of neurologists in umbilical stump in infants
resource-limited settings, and concerns for use of botulinum toxin as an agent born to unvaccinated
of bioterrorism.3 women.
● Maternal tetanus is most
TETANUS commonly due to unhygienic
Clostridium tetani is a gram-positive, anaerobic, spore-forming bacillus that birth or abortion practices.
produces a plasmid-encoded toxin (tetanospasmin) that causes the clinical
syndrome of tetanus. C. tetani spores are present worldwide in soil and in the ● Non-neonatal,
nonmaternal tetanus
intestinal tract (and hence feces) of humans and other animals. Tetanus spores (referred to in this article
cause human disease when they enter wounds, germinate, and produce simply as tetanus) can be
tetanus toxin. caused by infections of
major or minor wounds,
chronic otitis media,
Pathophysiology injection drug use,
Tetanus toxin travels hematogenously to peripheral nerve terminals, where it or surgery.
undergoes retrograde transport through peripheral nerve axons to their cell
bodies.1,4 Tetanus toxin then traverses the synapse to arrive at presynaptic
inhibitory neuron terminals, where it cleaves synaptobrevin, resulting in
impaired fusion of synaptic vesicles, thus decreasing inhibitory neuronal
transmission (FIGURE 10-1, FIGURE 10-2).1 Disinhibited peripheral motor, cranial,
and autonomic nerves are rendered hyperactive, leading to the clinical features
of tetanus, which are described below.
Classification and Causes of Tetanus
Tetanus can occur across the life span. When occurring in neonates, it is referred
to as neonatal tetanus, defined by the World Health Organization (WHO) as
“any neonate with normal ability to suck and cry during the first 2 days of
life and who between 3 and 28 days of age cannot suck normally and becomes
stiff or has spasms.”5 Neonatal tetanus is most often due to infection of the
umbilical stump in infants born to unvaccinated women. Infection of the
umbilical stump may be caused by unhygienic instruments used to sever it
or traditional practices of applying animal products (eg, cow dung) or soil to
the umbilical stump.6
When occurring in the peripartum or periabortion setting, tetanus is referred
to as maternal tetanus,6 defined by Thwaites and colleages7 as “tetanus during
pregnancy or within 6 weeks of the end of pregnancy (birth, miscarriage, or
abortion).”6,7 Maternal tetanus is most commonly due to unhygienic birth or
abortion practices.
Aside from lack of maternal vaccination, risk factors for neonatal and
maternal tetanus include births outside health care settings, untrained birth
attendants, unsanitary birth practices or locations, use of traditional substances
(eg, animal products, dirt) in birth or umbilical cord care, ritual neonatal
surgeries (eg, circumcision, ear piercing, uvulectomy), poverty, poor maternal
education, poor antenatal care, young age at first pregnancy, and cultural
constraints on women’s movements and contacts.6
Non-neonatal, nonmaternal tetanus (referred to in this article simply as
tetanus) can be caused by infections of major or minor wounds, chronic otitis
media, injection drug use, or surgery. No apparent cause is found in up to
CONTINUUMJOURNAL.COM 1461
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
TETANUS, BOTULISM, AND DIPHTHERIA
one-third of patients with
tetanus, which is suggestive of
minor unnoticed wounds that
became infected.8–11 Lower limb
wounds are the most common
site of infection. In regions of
high incidence, tetanus is more
common in men, which is
attributed to the higher
likelihood of occupations leading
to injury and a lower vaccination
rate compared to women (who
are generally vaccinated
during pregnancy).8–10,12
Between 2001 and 2008, the
majority of tetanus cases in the
United States were wound
related, with 15% of cases
occurring in IV drug users and
15% of cases occurring in patients
with diabetes mellitus (due to
infection of chronic ulcers).13
Only one case of neonatal tetanus
was reported in the United States
during this period.
Epidemiology
Although only 466 cases of
tetanus were reported in the
United States between 2000 and
2015, many countries in South
FIGURE 10-1
Sites of action of tetanus and botulinum toxins. Asia, Southeast Asia, and
Schematic illustration of motor neuron and sub-Saharan Africa far exceeded
interacting spinal inhibitory interneuron with this figure in 2015 alone,
pathways and sites of action of tetanus neurotoxin including India (2268 cases),
(TeNT) (green) and botulinum neurotoxins
(BoNTs) (blue) shown. Uganda (1804 cases), Nepal (888
ER = endoplasmic reticulum. cases), Philippines (880 cases),
Reprinted with permission from Lalli G, et al, Trends Pakistan (667 cases), and
Microbiol.1 © 2003 Elsevier.
Bangladesh (559 cases).14 This
persistent high incidence of a
vaccine-preventable disease
is attributed to only 65% of countries reporting vaccine coverage of greater
than 90%.15
With the rise in vaccine coverage, the number of reported cases of tetanus
worldwide has fallen from more than 100,000 per year in the early 1980s (when
vaccine coverage was less than 30%) to 10,337 reported cases in 2015 (with
86% worldwide vaccine coverage).15 Reported neonatal cases peaked above
30,000 per year in the 1980s (6.7 per 1000 live births), when the vaccine
coverage of pregnant women was less than 10%, and fell to 3569 cases by 2015 as
vaccine coverage of pregnant women rose to 69%.16 However, these reported
1462 OCTOBER 2018
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
FIGURE 10-2
Cellular mechanism of action of tetanus and botulinum neurotoxins. Tetanus neurotoxin (TeNT)
(green) and botulinum neurotoxin (BoNT) (red) follow a four-step mechanism to enter
and inhibit neurons: (1) membrane binding, (2) internalization, (3) translocation, and
(4) intracellular action.
GPI = glycosylphosphatidylinositol (GPI)–anchored glycoprotein; SNAP-25 = synaptosome-associated
protein 25; SNARE = soluble N-ethylmaleimide-sensitive fusion protein (NSF) attachment protein receptor;
VAMP = vesicle-associated membrane protein.
Reprinted with permission from Lalli G, et al, Trends Microbiol.1 © 2003 Elsevier.
figures are believed to be underestimates of the true incidence of tetanus because
of underreporting in high-incidence regions; estimates of true incidence were as
high as 700,000 to 1 million cases per year in the 1980s, nearly 80% of which
were estimated to be neonatal tetanus.6,7,17,18
Using vital registration data, verbal autopsy studies, and mortality surveillance
data along with modeling for regions without available data, the 2015 Global
Burden of Disease Study estimated 56,743 deaths due to tetanus in 2015, with
35% of those deaths occurring in neonates.19 Compared to 1990 estimates, these
2015 figures represent a 90% decrease in the estimated global mortality rate of
non-neonatal cases and an 81% decrease for neonatal cases.19 This progress is
attributed to the WHO/United Nations Children’s Fund (UNICEF)/United
Nations Population Fund (UNFPA) Maternal and Neonatal Tetanus Elimination
program, the goal of which is to reduce the incidence of neonatal tetanus to fewer
than 1 per 1000 live births in every district worldwide through immunization
of pregnant women and women of childbearing age, promotion of hygienic birth
and umbilical cord practices, and increased surveillance.18 As of 2016, only 18
countries had not met this program’s elimination goal: Afghanistan, Angola,
Central African Republic, Chad, Democratic Republic of Congo, Ethiopia,
Guinea, Haiti, Kenya, Mali, Nigeria, Pakistan, Papua New Guinea, Philippines,
Somalia, Sudan, South Sudan, and Yemen.20 Ethiopia and the Philippines have
achieved partial elimination.20
From 2001 to 2008, the US annual incidence of tetanus was 0.1 per 1 million
(0.23 per 1 million in individuals aged 65 years and older), a 97.5% decrease from
3.9 per 1 million in 1947, the first year tetanus became a reportable disease in the
CONTINUUMJOURNAL.COM 1463
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
TETANUS, BOTULISM, AND DIPHTHERIA
KEY POINTS United States.13 Between 2001 and 2008, the fatality rate for cases of tetanus
in the United States was 13.2%.13 In the United States between 2001 and 2008,
● The clinical presentation
of tetanus can be classified
of the 92 cases (out of 233 total) for whom vaccination status was available,
as generalized, local nearly 70% had never been vaccinated, and of the remaining patients who had
(affecting a single limb at the received three or more doses of the primary series, 62% had not received a
site of wound infection), booster in the previous 10 years.13
or cephalic (affecting
only muscles innervated by
cranial nerves after a head Clinical Manifestations
wound infection). The clinical presentation of tetanus can be classified as generalized, local
(affecting a single limb at the site of wound infection), or cephalic (affecting only
● Disinhibition of motor muscles innervated by cranial nerves after a head wound infection). Local and
neurons of peripheral and
cranial nerves due to tetanus cephalic tetanus generally account for a very small percentage of cases9,11,21
leads to increased motor and may evolve into generalized tetanus.
activity and manifests The incubation period from time of injury to onset of clinical symptoms
clinically as muscle spasms. averages 7 to 10 days with a range of 1 to 60 days.9,11,12 Disinhibition of motor
In the cranial nerve–
innervated muscles, this
neurons of peripheral and cranial nerves leads to increased motor activity and
leads to the classic features manifests clinically as muscle spasms. In the cranial nerve–innervated muscles,
of risus sardonicus, trismus, this leads to the classic features of risus sardonicus (facial spasm producing a
and laryngospasm. In smiling appearance), trismus (lockjaw), and laryngospasm. In extremity and
extremity and axial
musculature, this leads to
axial musculature, increased motor activity results in muscle rigidity with
muscle rigidity with superimposed painful spasms of the limbs and abdominal and paraspinal muscles
superimposed painful and opisthotonos (extension of the head, neck, and spine leading to an arching of
spasms of the limbs and the back) (FIGURE 10-322).
abdominal and paraspinal
Consciousness is preserved. The
muscles and opisthotonos.
time from first symptoms to
● Attempting to elicit the onset of spasms averages 2 to
gag reflex results in spasm 4 days and ranges from fewer
of the masseter muscles, than 1 day to 11 days.9,11,12 Spasms
causing the patient to bite
down (the “spatula test”). generally last for 2 weeks.12
Despite disinhibited activity
● As a result of disinhibited of motor neurons, reflexes have
sympathetic overactivity in been reported to be normal and
patients with tetanus,
autonomic instability can
plantar reflexes to be flexor,
occur several days into although plantar stimulation
the illness and becomes may induce spasm of the tested
more prominent in the lower extremity.23 Attempting to
second week.
elicit the gag reflex results in
spasm of the masseter muscles,
causing the patient to bite
down. This “spatula test” has
been reported to have 94%
sensitivity and 100% specificity
for the diagnosis of tetanus
(CASE 10-1).24
FIGURE 10-3 The most common signs at
Clinical signs of tetanus. A, Risus sardonicus; presentation include trismus
B, opisthotonos. (96% to 97.7% of patients),
Panel A reprinted from World Health Organization. Panel B
spasms of the body (41% to
reprinted from the Centers for Disease Control and
Prevention. Images found at Immunization Action 73%; opisthotonos in 49%9),
Coalition. immunize.org/photos/tetanus-photos.asp.22 dysphagia (27% to 82%), and
1464 OCTOBER 2018
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
body stiffness (71% to 94%).8–11 Less common symptoms at presentation include
dyspnea (3% to 10%) and fever (6% to 11%).8–11
As a result of disinhibited sympathetic overactivity, autonomic instability can
occur several days into the illness and becomes more prominent in the second
week.12 Autonomic complications have been reported in 20% to 60% of patients9–11,25
and can include tachyarrhythmias or bradyarrhythmias, hypertension or
hypotension, severe sweating, and exquisite sensitivity to beta-blockers.26
Intensive care is required for an average of 2 to 3 weeks, with a median
duration of ventilatory support reported at 23 days (range of 17 to 60 days).7
Muscular rigidity may persist after resolution of the acute phase of the illness,27
and complete recovery may require months of rehabilitation.7 Data on long-term
outcomes of non-neonatal tetanus are rare; in one series, long-term sequelae
occurred in 8.6% of survivors (two patients had hypoxic brain injury, two
required limb amputation, and one had an abnormal gait).11
When intensive care unit (ICU) facilities capable of mechanical ventilation
are not available, the most common cause of death is respiratory failure.8,28
A 67-year-old man with a history of type 2 diabetes mellitus and chronic CASE 10-1
nonhealing toe ulcers presented to the emergency department for
new-onset muscle stiffness throughout his body. Two days prior, he had
presented to his dentist for evaluation of jaw pain and difficulty
chewing; the dental examination and a dental x-ray to evaluate for
temporomandibular syndrome and dental abscess were unremarkable.
He denied illicit drug use, infection, or injury. A toxicology screen
was normal.
While undergoing evaluation in the emergency department, he
developed spasms of his entire body in which his back arched and his
neck extended. Attempts to examine him between spasms would
provoke spasms of his extremities, and an attempt to assess his gag reflex
was notable for limited jaw opening and biting down on the tongue
depressor when the palate was stimulated. As his spasms increased in
frequency and severity, he developed compromise of his airway and was
intubated and admitted to the intensive care unit. A diagnosis of tetanus
was made, and diazepam, tetanus antitoxin, and metronidazole were
initiated. During the course of the patient’s treatment, it was discovered
that his last booster vaccine was at age 48.
Tetanus is infrequently seen in the United States, so early symptoms such COMMENT
as trismus and body stiffness may not lead to immediate diagnosis, which
may only be recognized when opisthotonic spasms develop. Chronic
diabetic foot ulcers represent a common nidus for entry of Clostridium
tetani in patients in the United States. A positive “spatula test” (masseter
spasm on attempted elicitation of the gag reflex) is highly sensitive and
specific for tetanus. Supportive care in an intensive care unit along with
treatment of spasms with benzodiazepines and administration of antitoxin
and antibiotics are key components of initial management.
CONTINUUMJOURNAL.COM 1465
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
TETANUS, BOTULISM, AND DIPHTHERIA
When ICU management of respiration and spasms is available, cardiovascular
complications related to autonomic instability emerge as the main cause of
death.28 ICU care can decrease mortality from 44% to 15%,28 but mortality
remains as high as 43% in recent series from regions where ICU care is limited or
unavailable.10,11 In resource-limited settings with limited or no ICU facilities,
older age (older than 60 years), shorter period of onset, and disease severity were
associated with increased mortality.9–11 In the United States between 2001 and
2008, the case fatality rate was 13.2%, with increased mortality seen in patients
who were older than 65 years of age, diabetic, or unvaccinated.13
NEONATAL TETANUS. Neonatal tetanus presents similarly to adult tetanus except
that refusal to feed is an early sign and the disease tends to progress more rapidly,
ostensibly because of shorter axonal length for retrograde transport of toxin.6
Spasms are characterized as clenched fists and dorsiflexion of the feet progressing
to opisthotonos.7 Other common symptoms and signs at presentation include
inconsolable crying and refusal to feed (100% of patients), intermittent tetanic
spasms (85.3%), risus sardonicus (73.3%), generalized rigidity (66.3%), umbilical
sepsis (63.4%), respiratory arrest (59.4%), and fever (53.5%).29
The median incubation period of neonatal tetanus is 5 to 7 days (range of 3 to
24 days).7 In the majority of patients, the period from first symptom to onset of
spasms is less than 24 hours and nearly always occurs within 4 days.8
Improved ICU care has had a dramatic effect on neonatal tetanus mortality,
which was 2.6% to 12.5% in 2009 and 2016 studies30,31 compared to 66.3% to
86.4% in series where ICU care is not available.8,29,32
Factors associated with risk of mortality include low birth weight, age of onset
at 7 days old or younger, age at presentation of younger than 10 days, respiratory
arrest, fever, risus sardonicus, generalized rigidity, and intercurrent infection.29,33
In survivors of neonatal tetanus, long-term sequelae occur in 26% of patients and
include developmental delay/cognitive impairment, behavioral problems,
motor/coordination deficits, and cerebral palsy.34
Diagnosis
Tetanus is a clinical diagnosis. Since clostridial culture from wounds may be negative
in cases of tetanus25 and can be positive in patients without tetanus,4 culture is
considered neither sensitive nor specific.4 Tetanus has been reported even in
adequately immunized neonatal35 and non-neonatal patients36,37 with serum titers
of antitoxin above presumed protective levels of 0.01 IU/mL. Therefore, evaluation
for antitoxin level is generally not indicated in the evaluation of patients with tetanus.
EMG is generally not necessary to make the diagnosis of generalized tetanus,
although it may be helpful in cases of local tetanus. The EMG features of tetanus
result from disinhibition of motor neurons: continuous involuntary spontaneous
motor activity (with normal amplitude/morphology of motor units), prolonged
motor activity during attempted relaxation after voluntary contraction, increased
F-wave amplitude (20% to 75% of compound muscle action potential [CMAP]
amplitude as compared to its normal value of 5%38), and absence of the silent
period that is normally present after peripheral stimulation (eg, elicitation of
tendon reflex).23,38,39
The differential diagnosis of acute muscular rigidity and spasms includes
strychnine poisoning, drug-induced dystonic reactions, and neuroleptic
malignant syndrome.12 Trismus (lockjaw) can be seen in isolation with dental
1466 OCTOBER 2018
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
infection but, unlike tetanus, would not lead to other manifestations beyond this KEY POINTS
region. Tetany can be seen in hypocalcemia but is usually accompanied by
● When intensive care unit
perioral and extremity paresthesia (which would not be expected in tetanus), facilities capable of
Chvostek sign (facial contraction when tapping the facial nerve over the upper mechanical ventilation are
jaw), and Trousseau sign (spasm of the hand after a blood pressure cuff is not available, the most
inflated on the arm). The differential diagnosis for neonatal tetanic spasms common cause of death in
patients with tetanus is
includes seizures due to a perinatal insult, meningitis, or encephalitis.
respiratory failure. When
intensive care unit
Treatment management of respiration
Treatment of tetanus must address several elements in parallel: airway and spasms is available,
cardiovascular
management, neutralization of tetanus toxin, treatment of spasms, treatment of
complications related to
the infected wound believed to be the portal of entry, treatment of autonomic autonomic instability
instability, and meticulous supportive care.6,12,40 emerge as the main cause
of death.
AIRWAY MANAGEMENT. Laryngeal and respiratory muscle spasms generally require
● Neonatal tetanus
intubation and mechanical ventilation, usually with pressure-controlled settings and
presents similarly to adult
positive end-expiratory pressure.12 Because of the potential compromise of the tetanus except that refusal
endotracheal tube by masseter and laryngeal spasm and the need for prolonged to feed is an early sign and
mechanical ventilation, early tracheostomy should be considered.41,42 the disease tends to
progress more rapidly.
NEUTRALIZATION OF TOXIN. IM injection of antitoxin in the form of human tetanus ● Tetanus is a clinical
immunoglobulin or equine antitoxin (where tetanus immunoglobulin is not diagnosis. Since clostridial
available) is recommended to neutralize circulating toxin and prevent further culture from wounds may be
neurologic toxicity, although ongoing toxin effects on the nervous system are not negative in cases of tetanus
and can be positive in
reversible by administration of antitoxin. Tetanus immunoglobulin dosing patients without tetanus,
regimens of 500 U may be as effective as higher doses of 3000 U to 6000 U,43 and culture is considered neither
it is recommended that some portion of the dose be injected at the site of the sensitive nor specific.
wound.43 If neither tetanus immunoglobulin nor equine antitoxin are available,
● The EMG features of
IV immunoglobulin (IVIg) may be considered since it contains antibodies
tetanus result from
against tetanus.21,43 disinhibition of motor
Immunization with tetanus toxoid vaccine is also recommended in patients neurons.
with active tetanus, both for long-term immunity and because it may compete
with active toxin for binding at sites of entry into the nervous system.12 ● Treatment of tetanus
must address several
Intrathecal administration of antitoxin has been compared to IM elements in parallel: airway
administration in several small trials, with a meta-analysis of these trials management, neutralization
suggesting a mortality benefit of intrathecal administration.40,44 The largest and of tetanus toxin, treatment
most recent trial did not demonstrate a mortality benefit of intrathecal antitoxin of spasms, treatment of the
infected wound believed to
compared to IM administration but reported decreases in the length of be the portal of entry,
hospitalization, duration of spasms, and duration of mechanical ventilation.45 treatment of autonomic
Current guidelines do not recommend intrathecal administration of tetanus instability, and meticulous
antitoxin as data are conflicting and available antitoxin in the United States is supportive care.
neither licensed nor formulated for intrathecal use.43
● IM injection of antitoxin in
the form of human tetanus
TREATMENT OF SPASMS. Patients should be cared for in a dark, quiet room since immunoglobulin or equine
sensory stimulation may provoke spasms. Classes of medications used in the antitoxin (where tetanus
immunoglobulin is not
treatment of spasms include benzodiazepines, neuromuscular blocking agents,
available) is recommended
and magnesium sulfate. to neutralize circulating
toxin and prevent further
BENZODIAZEPINES. Benzodiazepines are considered the standard of care for the neurologic toxicity.
treatment for tetanus spasms.40 Despite limited evidence, diazepam is used
CONTINUUMJOURNAL.COM 1467
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
TETANUS, BOTULISM, AND DIPHTHERIA
most commonly because of its widespread availability in regions of highest
incidence.12,46 Doses of diazepam as high as 3 mg/kg/d to 8 mg/kg/d may be
necessary, frequently inducing respiratory depression requiring intubation and
mechanical ventilation.12 Patients receiving high doses of diazepam for a prolonged
period must be monitored for metabolic acidosis caused by the preservative
propylene glycol in IV formulations of diazepam.40 Midazolam may be a preferable
benzodiazepine given its shorter duration of action, but data are limited and
midazolam is often not available in regions of high tetanus incidence.12,40
NEUROMUSCULAR BLOCKADE. If spasms cannot be adequately controlled with
sedating agents, neuromuscular blocking agents may be required. Vecuronium,
pipecuronium, and rocuronium are preferred, whereas pancuronium is thought
to be suboptimal because of its inhibition of catecholamine reuptake, which may
exacerbate autonomic instability.12
MAGNESIUM. Data for magnesium sulfate in the treatment of tetanus are
conflicting.40 The largest clinical trial of magnesium versus placebo demonstrated
no difference in mortality or need for mechanical ventilation but did demonstrate
decreases in the necessary dosages of benzodiazepine and neuromuscular
blocking agents.47 However, a meta-analysis of this trial and two smaller trials
found that heterogeneity prevented firm conclusions beyond the lack of
mortality benefit for magnesium versus placebo or versus diazepam.48
OTHER AGENTS. Data on treatment of spasms with dantrolene, ketamine,
propofol, botulinum toxin, and intrathecal baclofen are limited to small case
series and case reports, and many of these agents are generally not available in
settings of highest tetanus incidence.40
WOUND TREATMENT. If a wound is present, it should be cleaned and debrided to
reduce the source of toxin production. Antibiotic therapy consists of oral or IV
metronidazole (30 mg/kg/d divided into four daily doses) or IV penicillin G
(100,000 U/kg/d divided into four to six doses) for 7 to 10 days.43 Although one
randomized trial demonstrated superiority of metronidazole (500 mg every
6 hours or 1 g rectally every 8 hours) over penicillin (procaine 1.5 million U IM
every 8 hours) with respect to mortality rate, length of hospital stay, and clinical
course,49 another trial showed no difference between IM benzathine penicillin
(1.2 million U as a single dose), oral metronidazole (600 mg every 6 hours for
10 days), and IV benzylpenicillin (2 million U every 4 hours for 10 days).50
Metronidazole is generally preferred over penicillin because a theoretical risk
exists of worsening spasms with penicillin because of penicillin’s competitive
antagonism of g-aminobutyric acid (GABA) receptors.12,40
TREATMENT OF AUTONOMIC INSTABILITY. Agents used in the management of
autonomic instability include labetalol, esmolol, morphine, magnesium sulfate,
atropine, clonidine, and epidural bupivacaine.12,40 Data are limited to small
case series and case reports with the exception of magnesium sulfate, which
was shown to reduce the need for verapamil for treatment of tachycardia in a
randomized trial.47 Longer-acting pure beta-blockers (eg, propranolol) should be
avoided or used only with great caution, as they may lead to hypotension,
bradycardia, unopposed alpha activity, or sudden death.12,25,26,51
1468 OCTOBER 2018
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
SUPPORTIVE CARE. As with any critically ill patient with neurologic disease, KEY POINTS
intensive supportive care is essential to avoid common complications such as
● Benzodiazepines are
ventilator-associated pneumonia, deep venous thrombosis, gastric ulcer, and considered the standard of
decubitus ulcer. Because excessive muscular and autonomic activity lead to high care for the treatment for
metabolic demands, early enteral feeding is recommended.12 Early percutaneous tetanus spasms. Despite
endoscopic gastrostomy should be considered since a nasogastric tube may limited evidence, diazepam
is used most commonly
trigger spasms.12
because of its widespread
availability in regions of
Prevention highest incidence.
Tetanus can be prevented by maintenance of vaccination status. Even in patients
who are unvaccinated or undervaccinated who develop acute wounds, tetanus ● If spasms from tetanus
cannot be adequately
may be prevented by appropriate prophylactic treatment. controlled with sedating
agents, neuromuscular
VACCINATION. All individuals should be vaccinated against tetanus. Tetanus blocking agents may
toxoid vaccine is created by using formaldehyde, which inactivates the toxin be required.
while maintaining its immunogenicity. Tetanus toxoid is generally administered ● If a wound is present, it
in combination with diphtheria toxoid and acellular pertussis (DTaP or Tdap should be cleaned and
vaccines; DT and Td formulations without pertussis are also available for patients debrided to reduce the
with a contraindication to the pertussis vaccine). The Centers for Disease Control source of toxin production.
Antibiotic therapy consists
and Prevention (CDC) recommends completion of a series of DTaP or DT
of oral or IV metronidazole
between ages 6 weeks and 6 years (at 2 months, 4 months, 6 months, between or IV penicillin G for 7 to
15 and 18 months, and between 4 and 6 years of age), a dose of Tdap or Td at age 10 days.
11 to 12 years, and subsequent boosters every 10 years.43,52 Notably, in a study of
more than 18,000 individuals in the United States in 2002, only 50% of ● All individuals should be
vaccinated against tetanus.
participants older than 60 years of age and 31% of participants older than 70 years
of age had serologic evidence of immunity to tetanus, suggesting inadequate ● Vaccination of pregnant
maintenance of booster administration every 10 years in older patients.2 women can prevent both
Vaccination of pregnant women can prevent both maternal tetanus and maternal tetanus and
neonatal tetanus, since
neonatal tetanus since tetanus IgG is transferred to the fetus transplacentally.7,21,53 tetanus IgG is transferred to
For pregnant women who have not completed a primary immunization series the fetus transplacentally.
(or with unknown immunization history), two doses of toxoid vaccine should be
administered 4 weeks apart, with the second dose administered at least 2 weeks ● For patients with wounds
of any type who have
before delivery, and three subsequent doses (6 months after the second dose and
received fewer than three
then yearly for 2 years) should be given over the course of postnatal visits and doses of tetanus toxoid
subsequent pregnancies.7,21,43 Maternal human immunodeficiency virus (HIV) vaccine or do not know their
or malaria infection may reduce maternal tetanus immunity and passive tetanus vaccine status, a
placental transfer, but data are conflicting and guidelines for how to optimize dose of tetanus toxoid
should be given. Patients
immunization in this context have not been developed.7,21 In parallel with with major wounds or
maternal vaccination, prevention of maternal and neonatal tetanus involves unclean wounds should
education programs to improve hygiene of birth and umbilical cord practices,6,7 also receive tetanus
which alone have been shown to lead to a 100-fold decrease in the incidence of immunoglobulin.
neonatal tetanus.54
ACUTE WOUND PROPHYLAXIS. For patients with wounds of any type who have
received fewer than three doses of tetanus toxoid vaccine or who do not know
their tetanus vaccine status, a dose of tetanus toxoid should be given (DTaP
[or DT] if younger than 7 years of age, Tdap [or Td] if 7 years of age or older)
(TABLE 10-2).43,52 Patients with major wounds (eg, puncture, avulsion,
crush, burn, frostbite, necrotic/gangrenous wounds) or unclean wounds (eg,
contaminated with dirt, feces, or saliva from an animal bite) should also receive
CONTINUUMJOURNAL.COM 1469
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
TETANUS, BOTULISM, AND DIPHTHERIA
tetanus immunoglobulin (250 U).43,52 For patients who are fully vaccinated
(three or more prior doses) with clean minor wounds, tetanus toxoid vaccine
is only indicated if it has been 10 or more years since the last vaccine dose.
For major or unclean wounds, tetanus toxoid vaccine should be given if the
last vaccine dose was 5 or more years prior; tetanus immunoglobulin is not
recommended in these scenarios.43,52 Notably, of US patients with acute
wound-related tetanus between 2001 and 2008 who sought care at the time of
the initial wound (only 36.5% of cases), 96.1% did not receive prophylactic
treatment as recommended by CDC guidelines.13
An exception to the above guidelines is patients who developed
hypersensitivity (Arthus-like reaction) or fever with a prior tetanus vaccine,
since their tetanus antibody titers are believed to be very high; it is recommended
that such patients not receive boosters more frequently than 10-year intervals
even if they develop a major or unclean wound.43
Adverse events associated with tetanus toxoid vaccine include anaphylaxis
(1.6 per 1 million) and brachial neuritis (0.69 per 10 million).21 Although
Guillain-Barré syndrome has been reported to occur after tetanus toxoid vaccine,
population studies have not demonstrated a definitive association.21
BOTULISM
Botulism is caused by Clostridium botulinum, an anaerobic gram-positive spore-
forming bacillus. Clinical disease is caused by botulinum toxin, of which there are
seven subtypes (A, B, C, D, E, F, G; a potentially novel toxin type [type H] was
subsequently found to be a hybrid of types A and F55). Human botulism is most
commonly caused by toxin types A, B, E, and F. Types C and D predominantly
affect animals; type G does not cause known naturally occurring disease.56
Pathophysiology
Botulinum toxin inhibits acetylcholine release at presynaptic nerve terminals
through interference with proteins involved in neurotransmitter vesicle fusion:
types A and E affect SNAP-25, types B, D, F, and G affect synaptobrevin,
and type C affects syntaxin and SNAP-25 (FIGURE 10-1, FIGURE 10-2).1 This results
in decreased neural transmission in both autonomic and motor peripheral nerves.
TABLE 10-2 Tetanus Prophylaxis in Woundsa
Clean, Minor Wounds All Other Woundsb
Vaccination History Tdap or Tdc Tetanus Immunoglobulin Tdap or Tdc Tetanus Immunoglobulin
Unknown or fewer than three doses Yes No Yes Yes
Three or more doses Nod No Noe No
Tdap = tetanus, diphtheria, acellular pertussis vaccine; Td = tetanus and diphtheria vaccine.
a
Reprinted from the Centers for Disease Control and Prevention.52
b
Wounds such as, but not limited to, those contaminated with dirt, feces, soil, and saliva; puncture sounds; avulsions; and wounds resulting from
missiles, crushing, burns, and frostbite.
c
Tdap is preferred to Td for adults who have never received Tdap. Single-antigen tetanus toxoid is no longer available in the United States.
d
Yes, if more than 10 years since the last tetanus toxoid–containing vaccine dose.
e
Yes, if more than 5 years since the last tetanus toxoid–containing vaccine dose.
1470 OCTOBER 2018
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
Classification of Botulism
Botulism is classified as infant botulism, foodborne botulism, wound botulism,
adult intestinal colonization botulism, and iatrogenic botulism (TABLE 10-3).
Botulinum toxin is also a potential agent of bioterrorism since it is considered the
most potent known toxin; with a lethal dose of 0.7 mcg to 0.9 mcg, a gram of toxin
would have the power to kill more than 1 million people if effectively disseminated.3
Failed attempts to use aerosolized botulinum toxin were conducted in Japan by
the cult Aum Shinrikyo (responsible for the 1995 sarin gas subway attacks in
Tokyo), and botulinum toxin–containing missiles were reportedly deployed by
Saddam Hussein’s forces in Iraq during the 1991 Persian Gulf War.3
INFANT BOTULISM. Infant botulism, the most common type of botulism,
is caused by ingestion of C. botulinum spores that germinate in the
gastrointestinal tract and release botulinum toxin. The infant gut may be more
susceptible to colonization because of immature gut flora.57 Type A accounts for
the majority of cases (83.4%), followed by type B (10.7%) and type E (0.9%).58
FOODBORNE BOTULISM. Foodborne botulism is caused by ingestion of food
contaminated by botulinum toxin. Types A (50%), E (37%), and B (10%) are the
most common causes in the United States, with type E primarily occurring
Comparison of Features of Types of Botulism TABLE 10-3
Adult
Intestinal
Infant Foodborne Wound Colonization Iatrogenic
Percent of 71% 13% 15% <1% <1%
US cases
2000–2015
Most common A, B, rarely E A, B, E A, B A, B, F A, B
botulinum toxin
types
Clinical Hypotonia, Dry mouth, nausea/ Same as foodborne Same as Same as foodborne
syndrome constipation, weak vomiting, botulism except no foodborne botulism except no
cry and suck, absent dysphagia, diplopia, abdominal pain or botulism abdominal pain or
or decreased gag, fixed, dilated constipation and gastrointestinal
ptosis pupils,a extraocular fever is common symptoms
muscle weakness,
extremity weakness
Treatment Human-derived Heptavalent Heptavalent Heptavalent Heptavalent
botulism botulinum botulinum botulinum botulinum
immunoglobulin antitoxin antitoxin antitoxin antitoxin
(BIG-IV)
Prevention Avoidance of honey Proper food Avoidance of IV Unknown Avoidance of excess
preparation and drug use (or use of dosage
canning techniques sterile needles)
IV = intravenous.
a
Not as common as typically believed; see text for discussion.
CONTINUUMJOURNAL.COM 1471
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
TETANUS, BOTULISM, AND DIPHTHERIA
among Alaska Natives (refer to the following section on epidemiology for
more information).59
WOUND BOTULISM. Wound botulism is caused by wound infection with
C. botulinum (most commonly types A and B) or its spores.60
ADULT INTESTINAL COLONIZATION BOTULISM. Adult intestinal colonization
botulism (also referred to as adult botulism of unknown etiology,56 hidden
botulism,61 and adult intestinal toxemia62) is a rare variant of botulism believed
to result from colonization of the gut with C. botulinum (types A or B) or
Clostridium baratii (type F) in patients with altered gastrointestinal flora due
to gastrointestinal disease, instrumentation, or recent antibiotics.63
IATROGENIC BOTULISM. Iatrogenic botulism has rarely occurred in patients
treated with inappropriately high doses of botulinum toxin (types A and B
are commercially available)64 and even more rarely in patients treated with
appropriate doses of botulinum toxin.65
Epidemiology
In the United States from 2001 to 2015, 2223 cases of botulism were reported to
the CDC; infant botulism accounted for 71% of reported cases (average of 105
cases per year), wound botulism accounted for 15% (average of 22 cases per year),
foodborne botulism accounted for 13% (average of 19 cases per year), and adult
intestinal colonization botulism, iatrogenic botulism, and botulism of unknown
cause accounted for less than 1% each (average of fewer than one case per year).66
INFANT BOTULISM. Although infant botulism is the most common form of
botulism, it remains rare, with an average incidence of 2.1 cases per 100,000 live
births in the United States from 1976 to 2006.58 Of 106 worldwide cases of infant
botulism in which an etiology was determined, 59% were linked to ingestion
of honey, the only known avoidable risk factor for the condition.58 Other cases
are thought to be caused by ingestion of spores in the environment (eg, dust).58
Because of increased awareness of honey exposure as a risk factor for infant
botulism, the rate of cases attributable to honey fell from 39.7% in the 1970s to
4.7% in the early 2000s.58
FOODBORNE BOTULISM. Refrigeration and cooking inhibit clostridial growth, and
cooking inactivates the toxin and spores.59 Canning and fermentation can provide
anaerobic conditions for germination of C. botulinum spores, as can nonrefrigerated
storage of food in airtight containers.59 In the United States from 1990 to 2000,
263 cases of foodborne botulism were reported, yielding an annual incidence of
1 per 10 million population.59 Alaska accounted for the most cases of any state
(39%) due to illness acquired through Alaska Natives’ consumption of seal oil and
fermented whale, seal, fish, and fish eggs.59 In Canada from 1985 to 2005, traditional
Native seafood preparation practices accounted for 83.5% of botulism outbreaks.67
In the lower 48 states and Hawaii, homemade foods were the cause of 88%
of foodborne botulism events (defined as a sporadic case or outbreak of two cases
or more) in which a cause was identified, and 69% of those events were due to
home-canned foods (affecting 70 people).59 Five events (affecting 10 people
total) were due to commercial food products, and two events (affecting 22 people
total) resulted from restaurant-related outbreaks.
1472 OCTOBER 2018
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
Of the few countries reporting foodborne botulism incidence, the Republic KEY POINTS
of Georgia is believed to have the highest rate with 879 cases between 1980 and
● For patients who are fully
2002 (median annual incidence of 0.9 per 100,000 from 1990 to 2002).68 vaccinated against tetanus
Home-preserved vegetables (80%) and smoked fish (12%) accounted for the (three or more prior doses)
majority of cases. with clean, minor wounds,
tetanus toxoid vaccine is
WOUND BOTULISM. Although botulism infection can complicate any wound, only indicated if it has been
nearly all cases of wound botulism in the United States occur in injection drug users, 10 or more years since the
last vaccine dose. For major
particularly patients who inject black tar heroin subcutaneously (skin-popping).56,60 or unclean wounds, tetanus
toxoid vaccine should be
Clinical Manifestations given if the last vaccine dose
Botulism is characterized by weakness affecting cranial nerve–innervated, was 5 or more years prior;
extremity, and respiratory musculature. tetanus immunoglobulin is
not recommended in
these scenarios.
INFANT BOTULISM. Infant botulism should be considered in the differential
diagnosis of the hypotonic infant. Median age at presentation is 4 months (age ● Botulism is classified as
range of 1.25 to 11 months).69 Common presenting symptoms and signs include infant botulism, foodborne
constipation, weak cry and suck, absent or decreased gag reflex, ptosis, and botulism, wound botulism,
preserved muscle stretch reflexes at presentation.69 Dilated pupils, respiratory adult intestinal colonization
botulism, and iatrogenic
distress, and ophthalmoplegia may also be seen.69 Nearly one-half of infants botulism.
require intubation, usually within 1 day of presentation.69 Recovery from infant
botulism generally occurs over weeks to months, and most infants make a ● Although botulism
complete recovery.57 The mortality rate worldwide is 1.1%.58 infection can complicate
any wound, nearly all cases
of wound botulism in the
FOODBORNE BOTULISM. Foodborne botulism presents as a rapidly progressive
United States occur in
descending paralysis involving the cranial nerves innervating the eyes and bulbar injection drug users,
musculature followed by the extremities. Neurologic symptoms are often particularly patients
accompanied by gastrointestinal symptoms. The median incubation period who inject black tar
after exposure is 1 day (range of 0 to 12 days).70,71 The classic pentad of heroin subcutaneously
(skin-popping).
symptoms and signs in botulism is dry mouth, nausea/vomiting, dysphagia,
diplopia, and fixed dilated pupils, although it is uncommon to observe the full ● Infant botulism should
pentad (only 13% of patients had all five features in one series).71 Three or more be considered in the
features of the pentad were present in 93% of patients in an Alaskan series (73% differential diagnosis of
the hypotonic infant.
type E)72 and 68% of patients in a series from the Republic of Georgia (presumed
to be predominantly type B).71 The individual findings of the classic pentad were ● Foodborne botulism
present as follows in studies of type A and B cases: dysphagia (82% to 96%), dry presents as a rapidly
mouth (80% to 93%), diplopia (76% to 91%), nausea (65% to 73%), vomiting progressive descending
paralysis involving the
(56% to 59%), and dilated pupils (27% to 44%).71,73 Although dilated pupils are
cranial nerves innervating
thought to distinguish botulism from Miller Fisher syndrome, this should not be the eyes and bulbar
relied upon, as many series demonstrate the low sensitivity of this finding in musculature followed by
botulism (present in 14% to 63% of patients).72–74 Dilated pupils may be more the extremities.
common in type B botulism (46%) compared to type A botulism (17%).73
● The classic pentad of
Other common symptoms of botulism include fatigue (77% to 90%), extremity symptoms and signs in
weakness (69% to 89%), dysarthria (58% to 84%), dizziness (51% to 71%), botulism is dry mouth,
constipation (35% to 73%), and abdominal pain/cramps (42% to 54%).71,73 Although nausea/vomiting, dysphagia,
uncommon, paresthesia (3% to 14%) and diarrhea (19% to 25%) may occur.71,73 diplopia, and fixed, dilated
pupils, although it is
The most common examination findings are upper extremity weakness uncommon to observe the
(75%), ptosis (73% to 76%), lower extremity weakness (69%), hypoactive gag full pentad.
reflex (8% to 65%), extraocular muscle weakness or ophthalmoplegia (65% to
79%), facial weakness (8% to 63%), and tongue weakness (58%).71,73 The majority
of patients are alert at presentation, although lethargy and obtundation may rarely
CONTINUUMJOURNAL.COM 1473
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
TETANUS, BOTULISM, AND DIPHTHERIA
be observed.73 Reflexes may be normal (54%), hypoactive or absent (40%), or,
rarely, hyperactive (6%).73 Nystagmus (22%) and ataxia (17%) can occur.73
Type A botulism is associated with a more severe illness than types B
and E with respect to need for mechanical ventilation70,73 and length of
hospitalization,73 although there appears to be no difference in mortality rates
between types of botulism when patients are treated with adequate supportive
care.73 An incubation period shorter than 1 day is associated with a higher
likelihood of intubation.70
Mortality rates for foodborne botulism in a series of 260 US patients from 1990
to 2004 were 5% for type A, 4% for type B, and 3% for type E.59 Higher mortality
rates have been reported in resource-limited settings (8% in the Republic of
Georgia)71 and older series before the advent of modern critical care (11% overall;
18% for type A, 53% for type E, and 29% for unknown type from 1947 to 1985).72
Factors most strongly associated with a higher likelihood of mortality include
older age; history of congestive heart failure or coronary artery disease; shortness
of breath or dysphagia at time of presentation;71 need for mechanical ventilation;
and clinical syndrome at presentation including shortness of breath, impaired
gag reflex, and no history of diarrhea.71,73,75 The combination of no history of
shortness of breath or vomiting and presence of normal facial strength was
associated with survival in all patients in one series.71
In one study of long-term outcome in patients with foodborne botulism in the
Republic of Georgia with median 4.3 years of follow-up from the time of illness,
patients were more likely than control subjects to report fatigue, weakness,
dizziness, dry mouth, difficulty with heavy lifting, exertional dyspnea,
limitations in vigorous activities, and decreased psychosocial well-being.76
Worse health was more likely in patients who were older or required mechanical
ventilation during the acute illness.
WOUND BOTULISM. Wound botulism presents similarly to foodborne botulism,
although gastrointestinal symptoms are typically absent and fever may be
present (attributable to other bacteria in the cutaneous abscess rather than to
botulism).56 In one series of six patients with wound botulism, return to
ambulation took up to 4 months.60
ADULT INTESTINAL COLONIZATION BOTULISM. In a series of 11 cases of type F
botulism, clinical features were generally similar to the above descriptions of
foodborne botulism.63 All patients required intubation within 48 hours of
presentation (73% within 24 hours of presentation), had extraocular muscle
dysfunction, developed quadriplegia by day 5, had hyporeflexia or areflexia, and
were alert on presentation. Dry mouth and dizziness occurred less commonly
than in types A and B. Cases of type F botulism were characterized as having a
rapidly progressive and severe course similar to type A but with a relatively rapid
time to recovery (occurring on average by day 8) akin to that of type B cases. All
patients reported in this series survived.
IATROGENIC BOTULISM. In a series of four patients treated for cosmetic purposes
with nearly 3000 times the recommended dose of IM injections of botulinum
toxin A, the clinical syndrome was similar to foodborne botulism with the
exception that none of the four patients had gastrointestinal symptoms.64 All
patients in this series survived.
1474 OCTOBER 2018
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
Diagnosis KEY POINTS
The differential diagnosis for botulism includes Guillain-Barré syndrome
● Although dilated pupils
(in particular, Miller Fisher syndrome and the pharyngeal-cervical-brachial are thought to distinguish
variant), myasthenia gravis, and acute brainstem stroke (CASE 10-2). botulism from Miller Fisher
syndrome, this should not
LABORATORY TESTING. Laboratory testing for botulism in the United States is be relied upon, as many
series demonstrate the low
conducted by the CDC in collaboration with local state health departments. A
sensitivity of this finding
diagnosis of botulism can be confirmed by detection of botulinum toxin in the in botulism.
serum, stool, or suspected food source. Stool sample is preferable in cases of
infant botulism77 and adult intestinal colonization botulism.63 Toxin detection ● Type A botulism is
and classification is performed using a mouse-based assay or enzyme-linked associated with a more
severe illness than types B
immunosorbent assay (ELISA), and polymerase chain reaction (PCR) may also and E with respect to
be used to detect Clostridium.78 In wound botulism, the mouse bioassay was need for mechanical
only 68% sensitive in one study (with clinical impression as the reference ventilation and length of
standard).79 Given the time it may take to obtain results and potential hospitalization, although no
difference appears to exist
false-negative results, treatment with antitoxin should not be delayed if in mortality rates between
clinical suspicion for botulism is high. Electrophysiologic studies may provide types of botulism that are
findings in support of the diagnosis, although characteristic findings may be treated with adequate
absent early in the clinical course.80,81 supportive care.
● Wound botulism presents
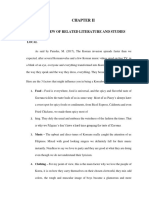
NERVE CONDUCTION STUDIES AND ELECTROMYOGRAPHY. As a presynaptic similarly to foodborne
neuromuscular junction disorder, botulism shares many electrophysiologic botulism, although
features with Lambert-Eaton myasthenic syndrome (LEMS) on nerve gastrointestinal symptoms
are typically absent and
conduction study and EMG: decreased CMAP amplitudes, decremental response
fever may be present
to low-frequency repetitive stimulation (FIGURE 10-482), incremental response (attributable to other
(facilitation) to high-frequency repetitive stimulation, short-duration bacteria in the cutaneous
low-amplitude motor unit potentials, and increased jitter on single fiber EMG. abscess rather than
Sensory nerve action potentials (SNAPs), sensory and motor conduction to botulism).
velocities, and distal latencies are normal.61 Normal nerve conduction velocities ● The differential diagnosis
do not fully exonerate Guillain-Barré syndrome, since these may be normal in for botulism includes
axonal variants (acute motor axonal neuropathy [AMAN] and acute motor- Guillain-Barré syndrome (in
sensory axonal neuropathy [AMSAN]) and may also be normal early in the particular, Miller Fisher
syndrome and the
course of acute inflammatory demyelinating polyradiculoneuropathy (AIDP). pharyngeal-cervical-
Therefore, repetitive stimulation is essential to distinguish botulism from brachial variant), myasthenia
Guillain-Barré syndrome. The acuity of presentation of botulism and prominence gravis, and acute brainstem
of ocular and bulbar symptoms clinically distinguishes botulism from LEMS. stroke.
Nerve conduction study and EMG findings that may distinguish botulism from
other presynaptic disorders such as LEMS include less post-tetanic facilitation
with high-frequency repetitive stimulation compared to LEMS (30% to 100% in
botulism versus >100% in LEMS) and persistence of post-tetanic facilitation for
several minutes in botulism (compared to less than 1 minute in LEMS).61,83
In one series, only 8 of 13 (62%) patients with foodborne botulism
demonstrated facilitation with high-frequency repetitive stimulation, a finding
more common in type B than in type A botulism.73 This incremental response
to high-frequency repetitive stimulation appears to be a more reliable finding
in infant botulism (present in 92% of 25 patients in one series).82 Differences
in post-tetanic facilitation in type B foodborne and infant botulism compared
to type A foodborne botulism have been attributed to the amount of toxin to
which individuals are exposed; with larger quantities of toxin exposure in
type A foodborne botulism compared to type B foodborne and infant
CONTINUUMJOURNAL.COM 1475
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
TETANUS, BOTULISM, AND DIPHTHERIA
CASE 10-2 A 48-year-old woman presented to the emergency department for
evaluation of double vision and difficulty swallowing. She described a
2-day history of abdominal pain and had vomited once.
Her initial examination in the emergency department was
unremarkable, although she reported double vision at the extremes of
gaze. An abdominal x-ray and head CT were normal. Two hours later, she
reported worsening double vision and was found to have mild bilateral
ptosis, bilateral eye abduction weakness, and a nasal voice. Her mental
status, pupillary reactions, extremity strength, and reflexes were normal.
The patient was admitted to the neurology service with a preliminary
diagnosis of “early Guillain-Barré syndrome versus myasthenia gravis
versus brainstem stroke.”
Over the next 12 hours, the patient developed progressive dysphagia,
dyspnea, and extremity weakness. Repeat examination revealed
worsening ptosis, limited extraocular movements in all directions of gaze,
absence of the gag reflex, and symmetric bilateral extremity weakness.
Her pupillary size and reactions remained normal. The patient was
intubated for airway protection. Nerve conduction study and EMG
demonstrated decreased compound muscle action potential (CMAP)
amplitudes with preserved conduction velocities, low-amplitude motor
unit potentials, decrement in CMAP amplitudes with low-frequency
stimulation, and increment with high-frequency stimulation, the latter
findings suggesting a presynaptic neuromuscular junction disorder.
Further history from the patient’s husband revealed that the patient
had prepared salsa from raw vegetables for a party and stored it in sealed
containers in her car overnight but consumed some the next day. A
diagnosis of botulism was made, and the Centers for Disease Control and
Prevention (CDC) was contacted to provide heptavalent botulinum
antitoxin. Fortunately, no others had yet consumed the salsa. CDC
analysis of the patient’s serum and food samples revealed type A
botulism. The patient made a full recovery.
COMMENT Botulism is a rare neuromuscular disorder that shares clinical features with
myasthenia gravis (ptosis, extraocular movement weakness) and Guillain-
Barré syndrome (cranial neuropathies followed by flaccid paralysis).
Although dilated pupils are believed to be a characteristic sign
distinguishing botulism from other conditions in the differential diagnosis,
pupils may be normal and normally reactive in a significant proportion of
patients with botulism. Nerve conduction study and EMG findings share
features with Lambert-Eaton myasthenic syndrome since both are
presynaptic neuromuscular junction disorders, but botulism presents
acutely, whereas Lambert-Eaton myasthenic syndrome presents
subacutely and does not typically affect the extraocular muscles at
presentation. Antitoxin can be obtained from the CDC, and the CDC can
also analyze serum and food samples.
1476 OCTOBER 2018
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
botulism, neuromuscular KEY POINTS
blockade may be severe enough
● As a presynaptic
to prevent post-tetanic neuromuscular disorder,
facilitation.82 This hypothesis is botulism shares many
supported by EMG studies of electrophysiologic features
patients with severe botulism with Lambert-Eaton
myasthenic syndrome on
(ventilator-dependent patients nerve conduction studies
with complete paralysis) in and EMG: decreased
whom high-frequency repetitive compound muscle action
stimulation yields no motor potential amplitudes,
decremental response to
responses and post-tetanic low-frequency repetitive
facilitation emerges over the stimulation, incremental
course of recovery.84 CSF analysis response (facilitation) to
is not necessary for diagnosis high-frequency repetitive
stimulation, short-duration
of botulism but, when reported, low-amplitude motor unit
has shown mild protein elevation potentials, and increased
(50 mg/dL to 60 mg/dL) in jitter on single fiber EMG.
type A botulism but no Sensory nerve action
potentials, sensory and
abnormalities in type FIGURE 10-4 motor velocities, and distal
B botulism.73 Repetitive stimulation of the left abductor pollicis latencies are normal.
brevis in infantile botulism. At 5 Hz, a mild
decrement is seen (8%). At 10 Hz, an increment is ● Nerve conduction study
Treatment
seen (25%), which increases with higher rates of and EMG findings that that
As with other acute stimulation (20 Hz [38%] and 50 Hz [94%]). may distinguish botulism
neuromuscular disorders Reprinted with permission from Cornblath DR, et al, from other presynaptic
affecting the respiratory Muscle Nerve.82 © 2004 John Wiley and Sons.
disorders such as Lambert-
musculature, such as Guillain-Barré Eaton myasthenic syndrome
syndrome and myasthenic crisis, include less post-tetanic
facilitation with high
supportive care in an intensive care unit is the cornerstone of management and has frequency repetitive
led to the greatest improvement in outcomes over time.56,77 stimulation compared to
In both infant botulism and foodborne botulism, antitoxin should be Lambert-Eaton myasthenic
administered as early as possible.77 Human-derived botulism immunoglobulin syndrome and persistence
of post-tetanic facilitation
(BIG-IV) is used for the treatment of infant botulism and is available through for several minutes in
the California Department of Public Health (refer to the Useful Resources botulism.
section), whereas equine-derived heptavalent botulinum antitoxin
(containing antitoxin against toxin types A, B, C, D, E, F, and G) is used in ● In both infant botulism
and foodborne botulism,
the treatment of all other forms of botulism and is available through the antitoxin should be
CDC (refer to the Useful Resources section).77,85 Wound debridement and administered as early
antibiotics are recommended in addition to antitoxin in patients with wound as possible.
botulism, but antibiotics are not recommended in infant, foodborne, or
adult intestinal colonization botulism.77 ● Human-derived botulism
immunoglobulin is used for
In a randomized placebo-controlled trial involving 122 infants, BIG-IV was the treatment of infant
found to decrease the length of hospital stay and duration of mechanical botulism, whereas equine-
ventilation by a mean of 3.3 weeks and 3.6 weeks, respectively, with no increase derived heptavalent
botulinum antitoxin
in adverse events.86 In an open-label study of 382 patients reported with this
(containing antitoxin against
clinical trial, treatment within 3 days decreased the mean length of a hospital stay toxin types A, B, C, D, E, F,
by nearly 1 week (from 2.9 weeks to 2 weeks) when compared to administration and G) is used in the
between days 4 and 7, with no increase in adverse events. Seven deaths occurred treatment of all other forms
of botulism and is available
and were not attributable to BIG-IV (five patients did not have botulism, one
through the Centers for
had a concurrent neuroblastoma, and one had cardiac arrest before BIG-IV Disease Control and
administration). Prevention.
CONTINUUMJOURNAL.COM 1477
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
TETANUS, BOTULISM, AND DIPHTHERIA
Heptavalent botulinum antitoxin has been tested in a small, randomized,
placebo-controlled trial in healthy subjects for safety, since a placebo-controlled
trial in patients with botulism would not be ethical.87 Data are available from
an open-label expanded access study reporting on 231 patients87: Adverse
events (most commonly pyrexia, rash, chills, nausea, and edema) occurred
in 10% of patients; one patient had mild serum sickness; one patient had a
severe reaction characterized by bradyarrhythmia, tachyarrhythmia, and
asystole of unclear relationship to heptavalent botulinum antitoxin (versus due to
botulism infection); and no patients had anaphylaxis. Patients receiving heptavalent
botulinum antitoxin should therefore be carefully monitored for
hypersensitivity reactions.
In a retrospective study of 132 cases of type A foodborne botulism in
which patients received a previously available form of antitoxin (trivalent
containing antitoxin to toxin types A, B, and E), the mortality rate was 10% for
patients who received the antitoxin in the first 24 hours, 15% for patients
who received the antitoxin after the first 24 hours, and 46% in patients who
did not receive the antitoxin.75 Early antitoxin administration also decreased
days in the hospital, days of mechanical ventilation, and time to sustained
improvement. Early administration of antitoxin is thought to be particularly
beneficial because it neutralizes the toxin before extensive binding to nerve
terminals occurs.75
Prevention
Prevention of foodborne botulism relies on safe food preparation procedures,
including adequate cooking temperature and time, refrigeration, and safe home
canning methods.59 Botulism spores are ubiquitous but require an anaerobic,
low-acid environment between 4.4°C and 48.8°C (40°F and 120°F) for
germination,59,88 which occurs in canning and fermentation. Safe home canning
requires use of a pressure cooker at 116°C (240.8°F) to kill spores prior to canning
and cooking canned goods to 85°C (185°F) for 10 or more minutes to destroy
the toxin before consumption.77,89 Recommendations vary with altitude since
boiling temperatures are lower at higher altitudes.74,77
The only known avoidable source of infant botulism is honey, which should
not be given to children younger than 1 year of age.58,77
DIPHTHERIC NEUROPATHY
Diphtheria is caused by the aerobic gram-positive bacillus Corynebacterium
diphtheriae. Humans are the only host and may be asymptomatic carriers even
when vaccinated. Transmission may be either respiratory (in pharyngeal
diphtheria) or cutaneous (in cutaneous diphtheria).
Pathophysiology
The bacterium produces a bacteriophage-encoded exotoxin that attaches to host
cells and mediates cellular death through interference with protein synthesis.90,91
The toxin can cause diphtheric neuropathy through effects on protein synthesis
in Schwann cells, leading to demyelination of peripheral nerves.92,93 Pathologic
analysis of nerves in diphtheric neuropathy has revealed demyelination in dorsal
root ganglia, nerve roots, and proximal peripheral nerves with no or minimal
inflammatory cellular infiltrate, consistent with a direct toxic effect of diphtheria
toxin on peripheral myelin.94,95
1478 OCTOBER 2018
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
Epidemiology KEY POINTS
The introduction of the diphtheria vaccine in the United States in the early 20th
● Prevention of foodborne
century led to a rapid decline in diphtheria incidence from a peak of more than botulism relies on safe food
200,000 per year in the early 1920s to just half as many cases by the end of the preparation procedures
1920s, 20,000 per year by the 1940s, and 5000 per year by the early 1950s.90,96,97 including adequate heating,
Diphtheria is now rare in the United States, with only six reported cases between refrigeration, and safe home
canning methods.
2000 and 2015.98 Although diphtheria was previously predominantly a childhood
illness, the majority of US cases now occur in adults because of lack of ● The only known
immunization, incomplete immunization, or waning immunity.96 preventable source of infant
Vaccine coverage was not available in many lower-income regions until later botulism is honey, which
in the 20th century, with an estimated 1 million cases per year in lower-income should not be given to
children younger than 1 year
regions before the 1970s.97 The WHO’s Expanded Programme on Immunization, of age.
launched in the 1970s with the goal of universal immunization for all children by
1990,99 played a major role in reducing the worldwide incidence of diphtheria. ● The most common
Worldwide incidence has fallen from nearly 100,000 reported cases in 1980 manifestation of diphtheria
is pharyngitis characterized
to 4530 in 2015.100 Diphtheria continues to occur in South and Southeast Asia by pharyngeal
(more than half of the reported worldwide cases in 2015 occurred in India) and pseudomembranes
Africa (more than one-third of reported worldwide cases in 2015 occurred in (adherent gray patches on
Madagascar),101 regions where vaccine the pharynx that bleed if
manipulated) accompanied
coverage is less than 80%,102 as it was in
by low-grade fever.
72% of countries as of 2015.100 The global
decline in diphtheria has been punctuated
by epidemics such as those in countries of
the former Soviet Union in the 1990s, which
peaked at more than 50,000 cases in 1995
and accounted for the majority of the
world’s cases during this period.96,97,103
Clinical Manifestations
The most common manifestation of
diphtheria is pharyngitis characterized by
pharyngeal pseudomembranes (adherent
gray patches on the pharynx that bleed
if manipulated) (FIGURE 10-5104)
accompanied by low-grade fever. Less
commonly, laryngeal involvement or
extreme swelling of the tonsils and cervical
lymph nodes leading to a “bull neck”
appearance can result in stridor and acute
respiratory compromise. Respiratory
diphtheria is a reportable disease in the
United States.
Diphtheria may cause myocarditis
(occurs in 10% to 25% of cases, and
FIGURE 10-5
manifests as congestive heart failure, heart Clinical findings in diphtheria.
block, or arrhythmias); renal failure (due A, Pharyngeal pseudomembranes.
to hypotension or toxin effect); and, less B, Bull neck.
commonly, endocarditis, mycotic Panel A reprinted with permission from
MacGregor RR.91 © 2015 Elsevier.
aneurysms, osteomyelitis, and septic Panel B reprinted from the Centers for
arthritis.90 Disease Control and Prevention.105
CONTINUUMJOURNAL.COM 1479
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
TETANUS, BOTULISM, AND DIPHTHERIA
Cutaneous diphtheria occurs when a preexisting skin lesion is infected
with C. diphtheriae. Cutaneous diphtheria is usually caused by nontoxigenic
strains of the bacterium, so systemic complications are uncommon.90 Cutaneous
diphtheria is not a reportable condition in the United States.
Neurologically, diphtheria infection can cause a peripheral polyneuropathy
with prominent involvement of the lower cranial nerves. In a study of 2292
cases of diphtheria that occurred in Germany between 1944 and 1949, 7.6%
of participants developed polyneuropathy.105 The likelihood of developing
diphtheric neuropathy was related to the severity of the initial diphtheria
infection, varying from 2% of patients with mild symptoms to 76.6% of patients
with severe symptoms.105 In more recent data from the diphtheria epidemics in
the former Soviet Union in the 1990s, 5% to 15.2% of patients developed
diphtheric neuropathy.106,107
CASE 10-3 A 27-year-old man presented for evaluation after developing flaccid
extremity paralysis while recovering from a respiratory illness at a
rehabilitation facility. The patient had developed a severe febrile
pharyngeal illness with tonsillar swelling and cervical lymphadenopathy
leading to airway compromise and intubation several weeks earlier.
Throat cultures had been inconclusive, but the patient was treated with
empiric antibiotics. Despite resolution of the acute pharyngeal illness,
the patient required mechanical ventilation for nearly 2 weeks. His course
was complicated by myocarditis and acute renal failure. After
extubation, he reported difficulty swallowing, and his voice was hoarse,
but these symptoms were attributed to being intubated for nearly
2 weeks. While undergoing rehabilitation over the following 2 weeks, he
began to have progressive improvement in his swallowing and speaking
but developed progressive weakness of his arms and legs.
His examination was notable for flaccid symmetric weakness of the
bilateral upper and lower extremities, areflexia, and diminished vibration
sensation to the level of the knees and wrists. The patient had recently
immigrated to the United States from India, and his prior vaccination
history was unknown.
COMMENT Diphtheric neuropathy has a biphasic course with bulbar weakness
emerging weeks after pharyngeal infection and extremity weakness
developing weeks after this as cranial neuropathies improve. This patient’s
bulbar phase was likely mistaken for persistent pharyngeal illness and
residual effects of intubation. Rapid processing of culture specimens on an
appropriate medium is necessary for diagnosis, so laboratories must be
alerted if diphtheria is under consideration, which it should be in patients
from endemic regions with incomplete vaccination coverage. Antitoxin
treatment may improve outcome if administered early in the course of the
pharyngeal illness, but administration at the time of development of
diphtheric neuropathy is of unclear benefit.
1480 OCTOBER 2018
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
Diphtheric neuropathy is usually biphasic. Within several weeks after KEY POINTS
pharyngeal infection, lower cranial neuropathies develop, leading to dysphonia;
● Diphtheric neuropathy is
dysphagia; and numbness of the face, tongue, and gingiva.108 Polyneuropathy usually biphasic. Within
affecting the extremities emerges several weeks later as cranial neuropathies several weeks after
improve,107,108 although 38% of patients in one series had secondary pharyngeal infection, lower
deterioration of bulbar dysfunction after initial resolution.107 The biphasic nature cranial neuropathies
develop, leading to
of diphtheric neuropathy, presence of severe bulbar symptoms in the absence of
dysphonia; dysphagia; and
limb symptoms at onset, and prolonged course of evolution of the condition numbness of the face,
distinguish it from other acute polyneuropathies such as Guillain-Barré tongue, and gingiva.
syndrome (CASE 10-3).107 Polyneuropathy affecting
the extremities emerges
A study of 50 patients in Latvia by Logina and colleagues107 and a study of
several weeks later as
32 patients in Russia by Piradov and colleagues108 described the clinical features cranial neuropathies
of adult patients who developed diphtheric polyneuropathy during the improve.
diphtheria epidemics in the former Soviet Union in the 1990s. Adults were
thought to have been primarily affected in these epidemics because of waning ● In one study,
administration of antitoxin
immunity from childhood vaccination.107 within 48 hours of
Latency from pharyngitis to first bulbar symptoms in these series ranged from pharyngeal symptom onset
2 to 50 days107,108 (median of 10 days in one study107 and a mean of 30 days in led to better outcomes for
the other108), and latency to nadir of extremity weakness was approximately 5 to patients with diphtheric
neuropathy, although it did
7 weeks (range of 2.5 to 8.7 weeks).107,108 Shorter latency to onset of neurologic not prevent severe disability
symptoms was associated with the most severe symptoms of diphtheric at nadir. No difference was
polyneuropathy and longer latency with earlier regression of motor symptoms.108 found in the outcome
Common clinical symptoms and signs at onset included dysarthria/dysphagia between patients who
received antitoxin after
(98% to 100% of patients), facial weakness (10% to 88%), extraocular movement
day 3 of pharyngeal
dysfunction (30% to 50%), respiratory failure (20% to 75%), cardiovascular infection and patients who
autonomic dysfunction (36% to 100%), and bladder dysfunction (31% to did not receive antitoxin.
34%).107,108 Other findings included pupillary abnormalities (including mydriasis
[50%], impaired light reflex [28%], anisocoria [25%]),108 ptosis (19%),108 impaired
visual acuity (with pale optic discs and delayed visual evoked potentials; 6%),
and dysfunction of cranial nerves XI (84%), XII (72%), and V (53%).107,108
Subsequent development of extremity weakness occurred in 81% to 88%
of patients,107,108 with up to 42% of these patients becoming quadriplegic at
nadir.108 Sensory deficits (including hypoesthesia, hyperesthesia, decreased joint
position and vibration sense, and sensory ataxia) occurred in 84% to 100% of
patients.107,108 Systemic involvement was common, including myocarditis (64%
to 94%),107,108 renal impairment (18% to 84%),107,108 pneumonia (38%),107 and
thromboembolism (6%).107
Most patients in these series made a complete or near-complete recovery with
only mild deficits at discharge.107,108 However, although 91% of patients had only
mild deficits at 1 year, 41% of these patients were still unable to return to manual
work despite being able to walk.107 Death occurred in 6% to 16% of patients
with diphtheric polyneuropathy, predominantly due to cardiopulmonary
complications.107,108 Administration of antitoxin within 48 hours of pharyngeal
symptom onset led to better outcomes for patients with diphtheric neuropathy,
although it did not prevent severe disability at nadir.107 No difference was
found in the outcome between patients who received antitoxin after day 3 of
pharyngeal infection and patients who did not receive antitoxin.107
A more attenuated presentation of diphtheric polyneuropathy has been
described in patients who are vaccinated, characterized by less frequent and less
severe bulbar symptoms, less severe extremity weakness, and longer latency
CONTINUUMJOURNAL.COM 1481
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
TETANUS, BOTULISM, AND DIPHTHERIA
to onset of neuropathy after pharyngeal symptoms (median of 43 days, range
of 35 to 58 days).109 The longer latency to onset of diphtheric neuropathy was
attributed to less frequent bulbar symptoms, with presentation of neuropathy
therefore occurring at the usual time of onset of extremity symptoms.109
Diagnosis
In the setting of acute pharyngeal diphtheria, diagnosis is made by throat culture.
Gram stain typically shows a pattern described as having a “Chinese character”
appearance, and halos around colonies are observed on Tinsdale medium.90 Tests
to evaluate for whether the cultured bacterium is toxigenic include PCR for the
gene encoding the toxin (TOX) and an antitoxin-based assay (Elek test),90,110
performed by state health authorities in conjunction with the CDC. Two negative
cultures more than 24 hours apart are recommended to confirm elimination of
the infection.111
Given the delay in emergence of diphtheric neuropathy after initial pharyngeal
infection, if a patient presents at the time of diphtheric neuropathy, pharyngeal
diphtheria cultures are likely to be negative during the period of neurologic
illness.112 High-titer antidiphtheria toxin antibodies (10 IU/mL) have been
described in a patient with diphtheric polyneuropathy who was not vaccinated
against diphtheria112; however, IgG against diphtheria toxin can be present in
patients who were previously vaccinated who subsequently become infected.109
CSF analysis in diphtheric neuropathy revealed albuminocytologic dissociation
in 78% of patients in one series: mean protein was 103 mg/dL (range of 15 mg/dL
to 283 mg/dL) and white blood cell count was 12 cells/mm3 or less (range
not reported).108
Nerve conduction studies in diphtheric polyneuropathy demonstrate slowed
conduction velocities, prolonged distal latencies, conduction block, and
prolonged F waves with preserved amplitudes, consistent with a
demyelinating polyneuropathy.94,107,112
Treatment
Acute pharyngeal diphtheria is treated with antibiotics and antitoxin. The
antibiotic regimen recommended by the CDC is erythromycin (40 mg/kg/d;
maximum, 2 g/d) orally or IV for 14 days or IM procaine penicillin G 300,000 U/d
(if weight 10 kg [22 lb] or less) and 600,000 U/d (if weight greater than 10 kg
[22 lb]) for 14 days.96
Diphtheria antitoxin binds circulating toxin and can prevent cellular entry and
toxicity. Antitoxin must be administered very early in the acute pharyngeal
illness to be maximally effective, and patients may still develop severe neurologic
illness despite early administration.107 The utility of administering antitoxin in a
patient who presents at the onset of neuropathy is uncertain. In the United States,
diphtheria antitoxin is only available through the CDC (refer to the Useful
Resources section). The antitoxin is produced in horses, so testing for sensitivity to
horse serum is recommended before administration to avoid allergic reactions.96
Patients with pharyngeal diphtheria should be isolated with droplet
precautions until two negative cultures are obtained from the nose and throat
24 hours after completing antibiotic therapy.111 Close contacts of patients should
undergo culture for C. diphtheriae and receive antibiotic prophylaxis (7 to 10 days
of oral erythromycin [40 mg/kg/d to 50 mg/kg/d; maximum 1 g/d] or one dose
of IM benzathine penicillin G [600,000 U in children less than 30 kg (66 lb);
1482 OCTOBER 2018
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
1.2 million U for adults or children more than 30 kg (66 lb)]; IM penicillin is KEY POINTS
preferred if concern exists regarding follow-up or adherence); they should also
● Nerve conduction
receive a booster dose of diphtheria toxoid vaccine if they have not had one in studies in diphtheric
more than 5 years (or completion of vaccine series if incomplete) and should be polyneuropathy
monitored for signs of diphtheria for 7 days.96,111 demonstrate slowed
conduction velocities,
prolonged distal latencies,
Prevention
conduction block, and
All individuals should be vaccinated against diphtheria. Diphtheria toxoid prolonged F waves with
vaccine is created by using formaldehyde to inactivate the toxin while preserved amplitudes,
retaining its immunogenicity. Diphtheria toxoid is generally administered consistent with a
demyelinating
in combination with tetanus toxoid and acellular pertussis (refer to the
polyneuropathy.
information on vaccinations in the tetanus section above for discussion of
this vaccine series). ● Acute pharyngeal
Notably, in a US study of more than 18,000 individuals in 2002, only diphtheria is treated with
38% of participants older than 60 years of age and 29.5% of participants antibiotics and antitoxin.
older than 70 years of age had serologic evidence of immunity to diphtheria,
suggesting inadequate adherence to booster immunization every 10 years in
older patients.2
CONCLUSION
Tetanus, botulism, and diphtheric neuropathy are bacterial toxin–mediated
neuromuscular syndromes that are now rare in the United States and other
high-income countries, although tetanus remains common worldwide and
botulism and diphtheric neuropathy may be underdiagnosed or underreported
in settings of limited resources. Increased injection drug use (botulism and
tetanus), waning immunity in an aging population (tetanus and diphtheria),
migration from areas where vaccination may not be universal (tetanus and
diphtheria), and the threat of bioterrorism (botulism has been considered a
potential bioterrorism agent) may result in a rise in cases of these diseases.
Neurologists must therefore be familiar with the key features of these conditions
to provide prompt diagnosis and early administration of antitoxin and tailored
supportive care.
ACKNOWLEDGMENTS
The author would like to thank Allan H. Ropper, MD, FAAN; Anthony A. Amato,
MD, FAAN; and Joseph R. Zunt, MD, MPH for helpful comments on a prior draft
of this manuscript.
USEFUL RESOURCES
CALIFORNIA DEPARTMENT OF PUBLIC HEALTH CENTERS FOR DISEASE CONTROL AND PREVENTION
To obtain consultation on a patient with suspected To obtain consultation on an adult patient with
infant botulism and to obtain human-derived suspected botulism or diphtheria and obtain
botulism immunoglobulin (BIG-IV), physicians should botulism antitoxin or diphtheria antitoxin, physicians
contact the Infant Botulism Treatment and should contact the Centers for Disease Control and
Prevention Program on-call physician at the Prevention Emergency Operations Center.
California Department of Health. 770-488-7100
510-231-7600 For botulinum antitoxin: cdc.gov/laboratory/
cdph.ca.gov/Programs/CID/DCDC/Pages/ drugservice/formulary.html#bat
ObtainBabyBig.aspx For diphtheria antitoxin: cdc.gov/laboratory/
drugservice/formulary.html#dat
CONTINUUMJOURNAL.COM 1483
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
TETANUS, BOTULISM, AND DIPHTHERIA
REFERENCES
1 Lalli G, Bohnert S, Deinhardt K, et al. The journey 15 World Health Organization. Tetanus. who.int/
of tetanus and botulinum neurotoxins in neurons. immunization/monitoring_surveillance/burden/
Trends Microbiol 2003;11(9):431–437. doi:10.1016/ vpd/surveillance_type/passive/tetanus/en/.
S0966-842X(03)00210-5. Updated August 25, 2017. Accessed August 29, 2018.
2 McQuillan GM, Kruszon-Moran D, Deforest A, 16 World Health Organization. Neonatal tetanus.
et al. Serologic immunity to diphtheria and who.int/immunization/monitoring_surveillance/
tetanus in the United States. Ann Intern Med burden/vpd/surveillance_type/active/neonatal_
2002;136(9):660–666. tetanus/en/. Updated August 25, 2017. Accessed
August 29, 2018.
3 Arnon SS, Schechter R, Inglesby TV, et al.
Botulinum toxin as a biological weapon: medical 17 Thwaites CL, Farrar JJ. Preventing and treating
and public health management. JAMA 2001; tetanus. BMJ 2003;326(7381):117–118.
285(8):1059–1070.
18 World Health Organization. Maternal and
4 Hodowanec A, Bleck TP. Tetanus (Clostridium neonatal tetanus elimination (MNTE): the
tetani). In: Bennett JE, Dolin R, Blaser MJ, editors. initiative and challenges. who.int/immunization/
Mandell, Douglas, and Bennet’s principles and diseases/MNTE_initiative/en/. Updated April 23,
practice of infectious diseases 8th ed. 2018. Accessed August 29, 2018.
Philadelphia, PA: Saunders, 2014:2757–2762.
19 Kyu HH, Mumford JE, Stanaway JD, et al.
5 World Health Organization. WHO-recommended Mortality from tetanus between 1990 and 2015:
standards for surveillance of selected findings from the Global Burden of Disease
vaccine-preventable diseases. apps.who.int/iris/ Study 2015. BMC Public Health 2017;17(1):179.
bitstream/10665/68334/1/WHO_V-B_03.01_eng. doi:10.1186/s12889-017-4111-4.
pdf. Updated July 2008. Accessed August 29, 2018.
20 World Health Organization. Maternal and
6 Roper MH, Vandelaer JH, Gasse FL. Maternal and neonatal tetanus elimination (MNTE): the
neonatal tetanus. Lancet 2007;370(9603): partnership. who.int/immunization/diseases/
1947–1959. doi:10.1016/S0140-6736(07)61261-6. MNTE_initiative/en/index1.html. Updated April
23, 2018. Accessed August 29, 2018.
7 Thwaites CL, Beeching NJ, Newton CR. Maternal
and neonatal tetanus. Lancet 2015;385(9965): 21 World Health Organization. Tetanus vaccines:
362–370. doi:10.1016/S0140-6736(14)60236-1. WHO position paper, February 2017. Wkly
Epidemiol Rec 2017;92(6):53–76.
8 Patel JC, Mehta BC. Tetanus: study of 8,697
cases. Indian J Med Sci 1999;53(9):393–401. 22 Immunization Action Coalition. immunize.org/
photos/tetanus-photos.asp. Accessed
9 Anuradha S. Tetanus in adults—a continuing
August 29, 2018.
problem: an analysis of 217 patients over 3 years
from Delhi, India, with special emphasis on 23 Struppler A, Struppler E, Adams RD. Local
predictors of mortality. Med J Malaysia tetanus in man. Its clinical and neurophysiological
2006;61(1):7–14. characteristics. Arch Neurol 1963;8:162–178.
doi:10.1001/archneur.1963.00460020062005.
10 Marulappa VG, Manjunath R, Mahesh Babu N,
Maligegowda L. A ten year retrospective study 24 Apte NM, Karnad DR. Short report: the spatula
on adult tetanus at the Epidemic Disease (ED) test: a simple bedside test to diagnose tetanus.
Hospital, Mysore in Southern India: a review of Am J Trop Med Hyg 1995;53(4):386–387.
512 cases. J Clin Diagn Res 2012;6(8):1377–1380. doi:10.4269/ajtmh.1995.53.386.
doi: 10.7860/JCDR/2012/4137.2363.
25 Edmondson RS, Flowers MW. Intensive care in
11 Chalya PL, Mabula JB, Dass RM, et al. Ten-year tetanus: management, complications, and
experiences with tetanus at a tertiary hospital in mortality in 100 cases. Br Med J 1979;1(6175):
Northwestern Tanzania: a retrospective review 1401–1404. doi:10.1136/bmj.1.6175.1401.
of 102 cases. World J Emerg Surg 2011;6:20.
26 Udwadia FE, Lall A, Udwadia ZF, et al. Tetanus
doi:10.1186/1749-7922-6-20.
and its complications: intensive care and
12 Farrar JJ, Yen LM, Cook TJ, et al. Tetanus. J Neurol management experience in 150 Indian patients.
Neurosurg Psychiatry 2000;69(3):292–301. Epidemiol Infect 1987;99(3):675–684. doi:10.1017/
S095026880006653X.
13 Centers for Disease Control and Prevention
(CDC). Tetanus surveillance—United States, 27 Sathirapanya P, Sathirapanya C, Limapichat K, et al.
2001–2008. MMWR Morb Mortal Wkly Rep 2011; Tetanus: a retrospective study of clinical
60(12):365–369. presentations and outcomes in a medical teaching
hospital. J Med Assoc Thai 2009;92(3):315–319.
14 World Health Organization. Tetanus (total)
reported cases. apps.who.int/immunization_ 28 Trujillo MH, Castillo A, España J, et al. Impact of
monitoring/globalsummary/timeseries/ intensive care management on the prognosis of
tsincidencettetanus.html. Updated February 28, tetanus. Analysis of 641 cases. Chest 1987;92(1):
2018. Accessed August 29, 2018. 63–65. doi:10.1378/chest.92.1.63.
1484 OCTOBER 2018
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
29 Basu S, Paul DK, Ganguly S, Chandra PK. Risk 43 Kimberlin DW, Brady MT, Jackson MA, Long SS;
factors for mortality from neonatal tetanus: Committee on Infectious Diseases; American
7 years experience in North Bengal,India. Ann Academy of Pediatrics. Tetanus. In: Red book:
Trop Paediatr 2006;26(3):233–239. doi:10.1179/ 2015 report of the Committee on Infectious
146532806X120336. Diseases Itasca, IL: American Academy of
Pediatrics, 2015. redbook.solutions.aap.org/
30 Amar-Singh HS. Neonatal tetanus in Malaysia.
chapter.aspx?sectionid=88187250
Med J Malaysia 2009;64(1):1–2.
&bookid=1484. Accessed August 29, 2018.
31 Trieu HT, Lubis IN, Qui PT, et al. Neonatal tetanus
44 Kabura L, Ilibagiza D, Menten J, Van den Ende J.
in Vietnam: comprehensive intensive care
Intrathecal vs. intramuscular administration of
support improves mortality. J Pediatric Infect Dis
human antitetanus immunoglobulin or equine
Soc 2016;5(2):227–230. doi:10.1093/jpids/piv059.
tetanus antitoxin in the treatment of tetanus: a
32 Mwaniki MK, Gatakaa HW, Mturi FN, et al. An meta-analysis. Trop Med Int Health 2006;11(7):
increase in the burden of neonatal admissions to 1075–1081. doi:10.1111/j.1365-3156.2006.01659.x.
a rural district hospital in Kenya over 19 years.
45 Miranda-Filho Dde B, Ximenes RA, Barone AA,
BMC Public Health 2010;10:591. doi:10.1186/
et al. Randomised controlled trial of tetanus
1471-2458-10-591.
treatment with antitetanus immunoglobulin by
33 Lambo JA, Anokye EA. Prognostic factors for the intrathecal or intramuscular route. BMJ 2004;
mortality in neonatal tetanus: a systematic 328(7440):615. doi:10.1136/bmj.38027.560347.7C.
review and meta-analysis. Int J Infect Dis 2013;
46 Okoromah CN, Lesi FE. Diazepam for treating
17(12):e1100–e1110. doi:10.1016/j.ijid.2013.05.016.
tetanus. Cochrane Database Syst Rev 2004;(1):
34 Mwaniki MK, Atieno M, Lawn JE, Newton CR. CD003954. doi:10.1002/14651858.CD003954.pub2.
Long-term neurodevelopmental outcomes after
47 Thwaites CL, Yen LM, Loan HT, et al. Magnesium
intrauterine and neonatal insults: a systematic
sulphate for treatment of severe tetanus: a
review. Lancet 2012;379(9814):445–452.
randomised controlled trial. Lancet 2006;368(9545):
doi:10.1016/S0140-6736(11)61577-8.
1436–1443. doi:10.1016/S0140-6736(06)69444-0.
35 Maselle SY, Matre R, Mbise R, Hofstad T.
48 Rodrigo C, Samarakoon L, Fernando SD,
Neonatal tetanus despite protective serum
Rajapakse S. A meta-analysis of magnesium
antitoxin concentration. FEMS Microbiol
for tetanus. Anaesthesia 2012;67(12):1370–1374.
Immunol 1991;3(3):171–175. doi:10.1016/
doi:10.1111/anae.12020.
0378-1097(91)90054-E.
49 Ahmadsyah I, Salim A. Treatment of tetanus: an
36 Abrahamian FM, Pollack CV Jr, LoVecchio F. Fatal
open study to compare the efficacy of procaine
tetanus in a drug abuser with “protective”
penicillin and metronidazole. Br Med J (Clin Res
antitetanus antibodies. J Emerg Med 2000;18(2):
Ed) 1985;291(6496):648–650. doi:10.1136/
189–193. doi:10.1016/S0736-4679(99)00192-4.
bmj.291.6496.648.
37 Livorsi DJ, Eaton M, Glass J. Generalized tetanus
50 Ganesh Kumar AV, Kothari VM, Krishnan A,
despite prior vaccination and a protective
Karnad DR. Benzathine penicillin, metronidazole
level of anti-tetanus antibodies. Am J
and benzyl penicillin in the treatment of tetanus:
Med Sci 2010;339(2):200–201. doi:10.1097/
a randomized, controlled trial. Ann Trop Med
MAJ.0b013e3181c2f534.
Parasitol 2004;98(1):59–63. doi:10.1179/
38 Risk WS, Bosch EP, Kimura J, et al. Chronic 000349804225003037.
tetanus: clinical report and histochemistry of
51 Buchanan N, Smit L, Cane RD, De Andrade M.
muscle. Muscle Nerve 1981;4(5):363–366.
Sympathetic overactivity in tetanus: fatality
doi:10.1002/mus.880040502.
associated with propranolol. Br Med J 1978;
39 Auger RG. AAEM minimonograph #44: diseases 2(6132):254–255.
associated with excess motor unit activity.
52 Centers for Disease Control and Prevention.
Muscle Nerve 1994;17(11):1250–1263. doi:10.1002/
Tetanus: epidemiology and prevention of
mus.880171103.
vaccine-preventable diseases. cdc.gov/vaccines/
40 Rodrigo C, Fernando D, Rajapakse S. pubs/pinkbook/tetanus.html. Updated
Pharmacological management of tetanus: an September 8, 2015. Accessed August 29, 2018.
evidence-based review. Crit Care 2014;18(2):217.
53 Demicheli V, Barale A, Rivetti A. Vaccines for
doi:10.1186/cc13797.
women for preventing neonatal tetanus.
41 Mukherjee DK. Tetanus and tracheostomy. Cochrane Database Syst Rev 2015;(7):
Ann Otol Rhinol Laryngol 1977;86(1 pt 1):67–72. CD002959. doi:10.1002/14651858.
CD002959.pub4.
42 Fasunla AJ. Challenges of tracheostomy in
patients managed for severe tetanus in a 54 Meegan ME, Conroy RM, Lengeny SO, et al.
developing country. Int J Prev Med Effect on neonatal tetanus mortality after a
2010;1(3):176–181. culturally-based health promotion programme.
Lancet 2001;358(9282):640–641. doi:10.1016/
S0140-6736(01)05787-7.
CONTINUUMJOURNAL.COM 1485
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
TETANUS, BOTULISM, AND DIPHTHERIA
55 Maslanka SE, Lúquez C, Dykes JK, et al. A novel 69 Thompson JA, Filloux FM, Van Orman CB, et al.
botulinum neurotoxin, previously reported as Infant botulism in the age of botulism immune
serotype H, has a hybrid-like structure with globulin. Neurology 2005;64(12):2029–2032.
regions of similarity to the structures of doi:10.1212/01.WNL.0000166950.35189.5E.
serotypes A and F and is neutralized with
70 Woodruff BA, Griffin PM, McCroskey LM, et al.
serotype A antitoxin. J Infect Dis 2016;213(3):
Clinical and laboratory comparison of botulism
379–385. doi:10.1093/infdis/jiv327.
from toxin types A, B, and E in the United States,
56 Hodowanec A, Bleck TP. Botulism (Clostridium 1975–1988. J Infect Dis 1992;166(6):1281–1286.
botulinum). In: Bennett JE, Dolin R, Blaser MJ, doi:10.1093/infdis/166.6.1281.
editors. Mandell, Douglas, and Bennet’s
71 Varma JK, Katsitadze G, Moiscrafishvili M, et al.
principles and practice of infectious diseases
Signs and symptoms predictive of death in
8th ed. Philadelphia, PA: Saunders, 2014:
patients with foodborne botulism—Republic of
2763–2767.
Georgia, 1980–2002. Clin Infect Dis 2004;39(3):
57 Rosow LK, Strober JB. Infant botulism: review 357–362. doi:10.1086/422318.
and clinical update. Pediatr Neurol 2015;52(5):
72 Wainwright RB, Heyward WL, Middaugh JP, et al.
487–492. doi:10.1016/j.pediatrneurol.2015.01.006.
Food-borne botulism in Alaska, 1947-1985:
58 Koepke R, Sobel J, Arnon SS. Global occurrence epidemiology and clinical findings. J Infect Dis
of infant botulism, 1976–2006. Pediatrics 2008; 1988;157(6):1158–1162. doi:10.1093/infdis/
122(1):e73–e82. doi:10.1542/peds.2007-1827. 157.6.1158.
59 Sobel J, Tucker N, Sulka A, et al. Foodborne 73 Hughes JM, Blumenthal JR, Merson MH, et al.
botulism in the United States, 1990–2000. Emerg Clinical features of types A and B food-borne
Infect Dis 2004;10(9):1606–1611. doi:10.3201/ botulism. Ann Intern Med 1981;95(4):442–445.
eid1009.030745. doi:10.7326/0003-4819-95-4-442.
60 Maselli RA, Ellis W, Mandler RN, et al. Cluster 74 Cherington M. Botulism. Ten-year experience.
of wound botulism in California: clinical, Arch Neurol 1974;30(6):432–437. doi:10.1001/
electrophysiologic, and pathologic study. archneur.1974.00490360008003.
Muscle Nerve 1997;20(10):1284–1295.
75 Tacket CO, Shandera WX, Mann JM, et al. Equine
doi:10.1002/(SICI)1097-4598(199710)20:10<1284::
antitoxin use and other factors that predict
AID-MUS11>3.0.CO;2-3.
outcome in type A foodborne botulism. Am J
61 Cherington M. Botulism: update and review. Med 1984;76(5):794–798. doi:10.1016/0002-9343
Semin Neurol 2004;24(2):155–163. doi:10.1055/ (84)90988-4.
s-2004-830901.
76 Gottlieb SL, Kretsinger K, Tarkhashvili N, et al.
62 David WS, Temin ES, Kraeft JJ, Hooper DC. Case Long-term outcomes of 217 botulism cases in the
3-2015: a woman with abdominal pain, dyspnea, Republic of Georgia. Clin Infect Dis 2007;45(2):
and diplopia. N Engl J Med 2015;372(4):364–372. 174–180. doi:10.1086/518890.
63 Gupta A, Sumner CJ, Castor M, et al. Adult 77 Kimberlin DW, Brady MT, Jackson MA, Long SS;
botulism type F in the United States, 1981–2002. Committee on Infectious Diseases; American
Neurology 2005;65(11):1694–1700. doi:10.1212/ Academy of Pediatrics. Botulism. In: Red book:
01.wnl.0000187127.92446.4c. 2015 report of the Committee on Infectious
Diseases Itasca, IL: American Academy of
64 Chertow DS, Tan ET, Maslanka SE, et al. Botulism
Pediatrics, 2015. redbook.solutions.aap.org/
in 4 adults following cosmetic injections with an
chapter.aspx?sectionid=88187124&bookid=1484.
unlicensed, highly concentrated botulinum
Accessed September 14, 2018.
preparation. JAMA 2006;296(20):2476–2479.
doi:10.1001/jama.296.20.2476. 78 Lindström M, Korkeala H. Laboratory diagnostics
of botulism. Clin Microbiol Rev 2006;19(2):
65 Bakheit AM, Ward CD, McLellan DL. Generalised
298–314. doi:10.1128/CMR.19.2.298-314.2006.
botulism-like syndrome after intramuscular
injections of botulinum toxin type A: a report of 79 Wheeler C, Inami G, Mohle-Boetani J, Vugia D.
two cases. J Neurol Neurosurg Psychiatry 1997; Sensitivity of mouse bioassay in clinical wound
62(2):198. botulism. Clin Infect Dis 2009;48(12):1669–1673.
doi:10.1086/599029.
66 Centers for Disease Control and Prevention.
National botulism surveillance. cdc.gov/ 80 Bakshi N, Rauf S, Fenton GE, Maselli RA.
botulism/surveillance.html. Updated April 18, Diagnostic difficulties in patients with adult
2017. Accessed August 29, 2018. botulism type A. J Clin Neuromuscul Dis
2000;2(1):18–21.
67 Leclair D, Fung J, Isaac-Renton JL, et al.
Foodborne botulism in Canada, 1985–2005. 81 Maselli RA, Bakshi N. AAEM case report 16.
Emerg Infect Dis 2013;19(6):961–968. doi:10.3201/ Botulism. American Association of
eid1906.120873. Electrodiagnostic Medicine. Muscle Nerve
2000;23(7):1137–1144. doi:10.1002/1097-4598
68 Varma JK, Katsitadze G, Moiscrafishvili M, et al.
(200007)23:7<1137::AID-MUS21>3.0.CO;2-7.
Foodborne botulism in the Republic of Georgia.
Emerg Infect Dis 2004;10(9):1601–1605.
doi:10.3201/eid1009.030806.
1486 OCTOBER 2018
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
82 Cornblath DR, Sladky JT, Sumner AJ. Clinical 94 Solders G, Nennesmo I, Persson A. Diphtheritic
electrophysiology of infantile botulism. Muscle neuropathy, an analysis based on muscle and
Nerve 1983;6(6):448–452. doi:10.1002/ nerve biopsy and repeated neurophysiological
mus.880060609. and autonomic function tests. J Neurol
Neurosurg Psychiatry 1989;52(7):876–880.
83 Fakadej AV, Gutmann L. Prolongation of
post-tetanic facilitation in infant botulism. 95 Fisher CM, Adams RD. Diphtheritic polyneuritis; a
Muscle Nerve 1982;5:727–729. doi:10.1002/ pathological study. J Neuropathol Exp Neurol
mus.880050911. 1956;15(3):243–268. doi:10.1097/00005072-
195607000-00002.
84 Kongsaengdao S, Samintarapanya K,
Rusmeechan S, et al. Electrophysiological 96 Centers for Disease Control and Prevention.
diagnosis and patterns of response to treatment Epidemiology and Prevention of Vaccine-
of botulism with neuromuscular respiratory Preventable Diseases: Diphtheria. cdc.gov/
failure. Muscle Nerve 2009;40(2):271–278. vaccines/pubs/pinkbook/dip.html. Accessed
doi:10.1002/mus.21256. August 29, 2018.
85 Centers for Disease Control and Prevention 97 Vitek CR. Diphtheria. Curr Top Microbiol Immunol
(CDC). Investigational heptavalent botulinum 2006;304:71–94.
antitoxin (HBAT) to replace licensed
98 World Health Organization. WHO vaccine-
botulinum antitoxin AB and investigational
preventable diseases: monitoring system 2017
botulinum antitoxin E. MMWR 2010;59(10):299.
global summary. apps.who.int/immunization_
86 Arnon SS, Schechter R, Maslanka SE, et al. Human monitoring/globalsummary/incidences?c=USA.
botulism immune globulin for the treatment of Updated February 28, 2018. Accessed August 29,
infant botulism. N Engl J Med 2006;354(5): 2018.
462–471. doi:10.1056/NEJMoa051926.
99 World Health Organization. The expanded
87 Botulism antitoxin heptavalent prescribing programme on immunization. who.int/
information. Cangene Corporation. BAT immunization/programmes_systems/supply_
(botulism antitoxin heptavalent [A, B, C, D, E, F, G] - chain/benefits_of_immunization/en/. Updated
[equine]) sterile solution for injection December 1, 2013. Accessed August 29, 2018.
prescribing information. fda.gov/downloads/
100 World Health Organization. Diphtheria. who.int/
BiologicsBloodVaccines/BloodBloodProducts/
immunization/monitoring_surveillance/burden/
ApprovedProducts/LicensedProductsBLAs/
diphtheria/en/. Updated May 15, 2018. Accessed
FractionatedPlasmaProducts/UCM345147.pdf.
August 29, 2018.
Updated March 2017. Accessed August 29, 2018.
101 World Health Organization. Diphtheria reported
88 United Stated Department of Agriculture.
cases. apps.who.int/immunization_monitoring/
Complete guide to home canning: guide 1
globalsummary/timeseries/tsincidencediphtheria.
principles of home canning. nchfp.uga.edu/
html. Updated February 28, 2018. Accessed
publications/usda/GUIDE01_HomeCan_rev0715.
August 29, 2018.
pdf. Accessed August 29, 2018.
102 World Health Organization. Immunization
89 Centers for Disease Control and Prevention.
coverage with DTP3 vaccines in infants (from
Botulism in the United States, 1899–1996:
<50%), 2016. who.int/immunization/monitoring_
handbook for epidemiologists, clinicians, and
surveillance/burden/vpd/surveillance_type/
laboratory workers. cdc.gov/botulism/pdf/
passive/big_dtp3_map_global_coverage.jpg?ua=1.
bot-manual.pdf. Accessed August 29, 2018.
Updated July 19, 2017. Accessed August 29, 2018.
90 MacGregor RR. Corynebacterium diphtheriae. In:
103 Galazka A. The changing epidemiology of
Bennett JE, Dolin R, Blaser MJ, editors. Mandell,
diphtheria in the vaccine era. J Infect Dis 2000;
Douglas, and Bennett’s principles and practice of
181(suppl 1):S2–S9. doi:10.1086/315533.
infectious diseases 8th ed. Philadelphia, PA:
Saunders, 2015;2366–2372. 104 Centers for Disease Control and Prevention.
Diphtheria symptoms. cdc.gov/diphtheria/
91 World Health Organization. Diphtheria vaccine:
about/symptoms.html. Updated January 15, 2016.
WHO position paper. Wkly Epidemiol Rec 2006;
Accessed August 29, 2018.
81(3):24–32.
105 Scheid W. Diphtherial paralysis; an analysis of
92 Pleasure DE, Feldmann B, Prockop DJ. Diphtheria
2,292 cases of diphtheria in adults, which
toxin inhibits the synthesis of myelin proteolipid
included 174 cases of polyneuritis. J Nerv Ment
and basic proteins by peripheral nerve in vitro.
Dis 1952;116(6):1095–1101.
J Neurochem 1973;20(1):81–90. doi:10.1111/
j.1471-4159.1973.tb12106.x. 106 Kadirova R, Kartoglu HU, Strebel PM. Clinical
characteristics and management of 676
93 Pleasure D, Messing A. Diphtheritic
hospitalized diphtheria cases, Kyrgyz Republic,
polyneuropathy. In: PJ Dyck, PK Thomas, editors.
1995. J Infect Dis 2000;181(suppl 1):S110–S115.
Peripheral neuropathy Vol. 2. Philadelphia, PA:
doi:10.1086/315549.
Elsevier Saunders, 2005:2147–2151.
CONTINUUMJOURNAL.COM 1487
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
TETANUS, BOTULISM, AND DIPHTHERIA
107 Logina I, Donaghy M. Diphtheritic 110 Efstratiou A, Engler KH, Mazurova IK, et al.
polyneuropathy: a clinical study and Current approaches to the laboratory diagnosis
comparison with Guillain-Barré syndrome. of diphtheria. J Infect Dis 2000;181(suppl 1):
J Neurol Neurosurg Psychiatry 1999;67(4): S138–S145. doi:10.1086/315552.
433–438.
111 Kimberlin DW, Brady MT, Jackson MA, Long SS;
108 Piradov MA, Pirogov VN, Popova LM, Avdunina Committee on Infectious Diseases; American
IA. Diphtheritic polyneuropathy: clinical analysis Academy of Pediatrics. Diphtheria. In: Red book:
of severe forms. Arch Neurol 2001;58(9): 2015 Report of the Committee on Infectious
1438–1442. doi:10.1001/archneur.58.9.1438. Diseases Itasca, IL: American Academy of
Pediatrics, 2015. redbook.solutions.aap.org/
109 Krumina A, Logina I, Donaghy M, et al. Diphtheria
chapter.aspx?sectionId=88187137&bookId=
with polyneuropathy in a closed community
1484&resultClick=1. Accessed August 29, 2018.
despite receiving recent booster vaccination.
J Neurol Neurosurg Psychiatry 2005;76(11): 112 Créange A, Meyrignac C, Roualdes B, et al.
1555–1557. doi:10.1136/jnnp.2004.056523. Diphtheritic neuropathy. Muscle Nerve 1995;
18(12):1460–1463. doi:10.1002/mus.880181217.
1488 OCTOBER 2018
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
Вам также может понравиться
- Managing Post Traumatic Olfactory Disorders: Iordanis KonstantinidisДокумент10 страницManaging Post Traumatic Olfactory Disorders: Iordanis Konstantinidisnight.shadowОценок пока нет
- Epilepsy Emergencies - Status Epilepticus, Acute Repetitite Seizures, and Autoimmune EncephalitisДокумент23 страницыEpilepsy Emergencies - Status Epilepticus, Acute Repetitite Seizures, and Autoimmune Encephalitisnight.shadowОценок пока нет
- Neuromyelitis Optica Spectrum DIsorder and Other Non-Multiple Sclerosis Central Nervous System Inflammatory DIseasesДокумент30 страницNeuromyelitis Optica Spectrum DIsorder and Other Non-Multiple Sclerosis Central Nervous System Inflammatory DIseasesnight.shadow100% (1)
- Management of Multiple SclerosisДокумент15 страницManagement of Multiple Sclerosisnight.shadowОценок пока нет
- Clinically Isolated Syndrome and Early Relapsing Multiple SclerosisДокумент19 страницClinically Isolated Syndrome and Early Relapsing Multiple Sclerosisnight.shadowОценок пока нет
- Central Nervous System Infections Complicating Immunosuppression and TransplantationДокумент27 страницCentral Nervous System Infections Complicating Immunosuppression and Transplantationnight.shadowОценок пока нет
- Antiepileptic Drug Treatment of Epilepsy in ChildrenДокумент27 страницAntiepileptic Drug Treatment of Epilepsy in Childrennight.shadowОценок пока нет
- Counseling and Management of The RIskis of Living With EpilepsyДокумент15 страницCounseling and Management of The RIskis of Living With Epilepsynight.shadowОценок пока нет
- Tuberculosis of The Central Nervous SystemДокумент17 страницTuberculosis of The Central Nervous Systemnight.shadowОценок пока нет
- Preventive Therapy of Migraine: Review ArticleДокумент14 страницPreventive Therapy of Migraine: Review Articlenight.shadowОценок пока нет
- Phases and PhenotypesДокумент19 страницPhases and Phenotypesnight.shadowОценок пока нет
- Disorders of The Cauda EquinaДокумент19 страницDisorders of The Cauda Equinanight.shadowОценок пока нет
- Myelopathies Due To Structural Cervical and Thoracic DiseaseДокумент17 страницMyelopathies Due To Structural Cervical and Thoracic Diseasenight.shadowОценок пока нет
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5795)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (345)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1091)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- Tutorial Week 10 Topic 9Документ14 страницTutorial Week 10 Topic 9patricia93limОценок пока нет
- Escalation Estimating Principles and Methods Using IndicesДокумент4 страницыEscalation Estimating Principles and Methods Using IndicesAlejandro RuizОценок пока нет
- May (2012) Nonequivalent Comparison Group DesignsДокумент21 страницаMay (2012) Nonequivalent Comparison Group Designsmathworld_0204Оценок пока нет
- 2021 Moon Calendar-Cosmic RevolutionДокумент47 страниц2021 Moon Calendar-Cosmic RevolutionYahira NoeliОценок пока нет
- Internet BillДокумент2 страницыInternet Billshiva ramОценок пока нет
- UA&P-JD Application FormДокумент4 страницыUA&P-JD Application FormuapslgОценок пока нет
- Bohemian RhapsodyДокумент5 страницBohemian RhapsodyTheresia Angel WidianaОценок пока нет
- Understanding Advertising and Consumer Behaviour: Pankaj KumarДокумент7 страницUnderstanding Advertising and Consumer Behaviour: Pankaj KumarAlfredo ValeraОценок пока нет
- Surf Excel ND AirelДокумент13 страницSurf Excel ND AirelPratibha Chandil100% (1)
- CEP Presentation AOL 2023Документ143 страницыCEP Presentation AOL 2023Josh DezОценок пока нет
- Module Virus Viroids PrionsДокумент17 страницModule Virus Viroids PrionsJennifer MartinОценок пока нет
- 01 Connecting Things 2.01 Chapter1-STUDENT 2Документ22 страницы01 Connecting Things 2.01 Chapter1-STUDENT 2ShafinОценок пока нет
- Gear CouplingДокумент10 страницGear CouplingKlmdaya BashisОценок пока нет
- Stoeger Airguns Product Catalog 2022Документ10 страницStoeger Airguns Product Catalog 2022Jack JackОценок пока нет
- CMC Business PlanДокумент32 страницыCMC Business PlanRobert ShisokaОценок пока нет
- Guidelines For Execution of Adapt-Pt: Structural Concrete Software SystemДокумент6 страницGuidelines For Execution of Adapt-Pt: Structural Concrete Software SystemJoe IztadaОценок пока нет
- Il Ruolo Delle Esperienze Religiose Nella Cultura Della LegalitàДокумент42 страницыIl Ruolo Delle Esperienze Religiose Nella Cultura Della LegalitàMarisa La BarberaОценок пока нет
- CSPL v1.2.0 Install-Eng Memo1Документ3 страницыCSPL v1.2.0 Install-Eng Memo1rammirisОценок пока нет
- Folio SainsДокумент15 страницFolio SainsMohammad Afifi Rohman80% (5)
- Company Profile Bureau Veritas ThailandДокумент13 страницCompany Profile Bureau Veritas ThailandPitichai PakornrersiriОценок пока нет
- General Lecture - Paper Deep RiversДокумент13 страницGeneral Lecture - Paper Deep RiversAJ TabuenaОценок пока нет
- CCC4 3.3 Coaching 55566778Документ178 страницCCC4 3.3 Coaching 55566778Mmc MixОценок пока нет
- Ladybug Reflection 10-14 NovДокумент2 страницыLadybug Reflection 10-14 Novapi-272157766Оценок пока нет
- Activity 1-Introduce Biological ToolsДокумент3 страницыActivity 1-Introduce Biological ToolsHaroldОценок пока нет
- Soa Sample ResumeДокумент5 страницSoa Sample Resumesam jessieОценок пока нет
- Week Logical FallaciesДокумент79 страницWeek Logical FallaciesSaqib AbbasОценок пока нет
- Self-Assessment Observation and Assessment of Child DevelopmentДокумент3 страницыSelf-Assessment Observation and Assessment of Child Developmentapi-508676940Оценок пока нет
- Chapter II Sample ThesisДокумент13 страницChapter II Sample ThesisAllen Bradley OngОценок пока нет
- 22 Hand Tool SafetyДокумент8 страниц22 Hand Tool SafetyAlma Tomas-CafeОценок пока нет
- Avy eДокумент11 страницAvy emsvkumar0% (1)