Вам также может понравиться
- Society, Schools and Progress in Peru: The Commonwealth and International Library: Education and Educational ResearchОт EverandSociety, Schools and Progress in Peru: The Commonwealth and International Library: Education and Educational ResearchОценок пока нет
- Athletes FormДокумент25 страницAthletes FormNhomz Valdez PasОценок пока нет
- Screening Committee Register: Republic of The Philippines Department of Education Region Ix, Zamboanga PeninsulaДокумент14 страницScreening Committee Register: Republic of The Philippines Department of Education Region Ix, Zamboanga PeninsulaMARLON TABACULDEОценок пока нет
- Lastname Firstname M.I: Inclusive Dates Sports Event Athletic Meet Remarks Coaches Division Pess SupervisorДокумент9 страницLastname Firstname M.I: Inclusive Dates Sports Event Athletic Meet Remarks Coaches Division Pess SupervisorAloha Aguilar BrusasОценок пока нет
- Screening Committee Register: Republic of The Philippines Department of Education Region Ix, Zamboanga PeninsulaДокумент14 страницScreening Committee Register: Republic of The Philippines Department of Education Region Ix, Zamboanga PeninsulaMARLON TABACULDEОценок пока нет
- Regional Table Tennis Athlete ProfileДокумент7 страницRegional Table Tennis Athlete ProfileNelma ArnaizОценок пока нет
- Laudit, Arnel Z.Документ30 страницLaudit, Arnel Z.Japs De la CruzОценок пока нет
- Athlete Record TemplateДокумент12 страницAthlete Record TemplateJessel PalermoОценок пока нет
- DanicaДокумент15 страницDanicaAndrian SasutilОценок пока нет
- Athlete 4Документ17 страницAthlete 4Raniel John Avila SampianoОценок пока нет
- Ar-I (Athlete Record) : Duldulao Frederick LДокумент1 страницаAr-I (Athlete Record) : Duldulao Frederick LRolan Domingo GalamayОценок пока нет
- Billote, CymarcДокумент16 страницBillote, CymarcEllen Bahatan SinahonОценок пока нет
- Athletes CredentialsДокумент22 страницыAthletes CredentialsMael AlimesОценок пока нет
- Climaco, DominicДокумент16 страницClimaco, DominicEllen Bahatan SinahonОценок пока нет
- 2023 Athlete RecordДокумент26 страниц2023 Athlete RecordJeferson Eborda RoselОценок пока нет
- 2023 Athlete Record1Документ26 страниц2023 Athlete Record1daxian.barrettoОценок пока нет
- Palaro Entry - PiatorДокумент24 страницыPalaro Entry - PiatorGenner RazОценок пока нет
- Athletes Glaisa AgbayДокумент6 страницAthletes Glaisa AgbayJerome DesameroОценок пока нет
- Classroom Daily Health Monitoring Tool For Covid-19: Grade 11-ChrysanthemumДокумент4 страницыClassroom Daily Health Monitoring Tool For Covid-19: Grade 11-Chrysanthemumkimbeerlyn doromasОценок пока нет
- Screening Committee Register: Republic of The Philippines Department of Education Region Ix, Zamboanga PeninsulaДокумент21 страницаScreening Committee Register: Republic of The Philippines Department of Education Region Ix, Zamboanga PeninsulaVenna Ross URGОценок пока нет
- 2023 Athlete RecordДокумент22 страницы2023 Athlete Recorddaxian.barrettoОценок пока нет
- Subacos 2024 - Athlete-Record V3Документ20 страницSubacos 2024 - Athlete-Record V3Nayr ZdahbОценок пока нет
- Lastname Firstname M.I: Inclusive Dates Sports Event Athletic Meet Remarks Coaches Divisio School Sports OfficerДокумент9 страницLastname Firstname M.I: Inclusive Dates Sports Event Athletic Meet Remarks Coaches Divisio School Sports Officeraljohn esplanaОценок пока нет
- Palaro Data Entry ATHLETE Athletics Copy 2Документ23 страницыPalaro Data Entry ATHLETE Athletics Copy 27vytdp64z9Оценок пока нет
- Department of Education Region Vii, Central Visayas: Enrolment Form Picture Gallery/ AR - 1Документ23 страницыDepartment of Education Region Vii, Central Visayas: Enrolment Form Picture Gallery/ AR - 1Jeraldine RepolloОценок пока нет
- Eclass For Shs Sample Made by A.C.PДокумент59 страницEclass For Shs Sample Made by A.C.PAnna Ruth de GuzmanОценок пока нет
- Masterlist of School BeneficiariesДокумент101 страницаMasterlist of School BeneficiariesGlenn MadriagaОценок пока нет
- Screening Committee Register: Republic of The Philippines Department of Education Region Ix, Zamboanga PeninsulaДокумент17 страницScreening Committee Register: Republic of The Philippines Department of Education Region Ix, Zamboanga PeninsulaMike PerezОценок пока нет
- SF 4& 6 Form FinalДокумент106 страницSF 4& 6 Form FinalMarissa JaramilloОценок пока нет
- SAMPLE 2Документ26 страницSAMPLE 2Edson Aljas LagudОценок пока нет
- Template For Athlete 1Документ26 страницTemplate For Athlete 1Florita LagramaОценок пока нет
- Template For Athlete 1Документ26 страницTemplate For Athlete 1Florita LagramaОценок пока нет
- SP Resolution No. 143 Birth RecordsДокумент2 страницыSP Resolution No. 143 Birth RecordsMely DelacruzОценок пока нет
- Athlete 1Документ14 страницAthlete 1Rolelie SombilonОценок пока нет
- List of Senior Citiens Federation Member of Brgy 2Документ3 страницыList of Senior Citiens Federation Member of Brgy 2Marvin PascualОценок пока нет
- Palarong Pambansa 2018Документ26 страницPalarong Pambansa 2018John Earl JohnОценок пока нет
- Regional Basketball Champ QualifiesДокумент18 страницRegional Basketball Champ QualifiesReagan DigalОценок пока нет
- Elementary Table Tennis Athlete ProfileДокумент10 страницElementary Table Tennis Athlete ProfileAvi Auerbach AvilaОценок пока нет
- School Form 1 School Register for SHS StudentsДокумент66 страницSchool Form 1 School Register for SHS Studentsmary diosaОценок пока нет
- Athlete RecordДокумент2 страницыAthlete RecordJessabelle OnzaОценок пока нет
- 2020 Athlete RecordДокумент3 страницы2020 Athlete RecordEM GinaОценок пока нет
- Senior High School Forms (1-7)Документ45 страницSenior High School Forms (1-7)Annalyn PeñaОценок пока нет
- 2020 Parents Consent Revised 2 1Документ12 страниц2020 Parents Consent Revised 2 1Gwyneth MarañaОценок пока нет
- Mati Doctors Academy 11 Humss B: School ID Region VIII Division District School Name School Year SectionДокумент3 страницыMati Doctors Academy 11 Humss B: School ID Region VIII Division District School Name School Year SectionBrian Alo VicenteОценок пока нет
- Regional Athlete RecordsДокумент10 страницRegional Athlete RecordsAldrinBalitaОценок пока нет
- Palaro Data Entry ATHLETE ACAINДокумент12 страницPalaro Data Entry ATHLETE ACAINmarina abanОценок пока нет
- Athlete RiveraДокумент10 страницAthlete RiveraAvi Auerbach AvilaОценок пока нет
- 2024_ Athlete RecordДокумент17 страниц2024_ Athlete RecordNoralyn Ngislawan-GunnawaОценок пока нет
- 2020 Athlete RecordДокумент2 страницы2020 Athlete RecordBriones Tiamzon JordanОценок пока нет
- Elementary Table Tennis Athlete RecordsДокумент10 страницElementary Table Tennis Athlete RecordsAvi Auerbach AvilaОценок пока нет
- Classroom Daily Health Monitoring Tool For CovidДокумент4 страницыClassroom Daily Health Monitoring Tool For Covidkimbeerlyn doromasОценок пока нет
- Athlete - Tumbaga JR Juno 2002Документ9 страницAthlete - Tumbaga JR Juno 2002Avi Auerbach AvilaОценок пока нет
- SF1 Grade 8 StudentsДокумент224 страницыSF1 Grade 8 StudentsRoe UbaldeОценок пока нет
- Main Menu: Department of Education Region Vii, Central VisayasДокумент17 страницMain Menu: Department of Education Region Vii, Central VisayasCjan Malahay GeconcilloОценок пока нет
- ATHLETES CredentialsДокумент14 страницATHLETES CredentialsJerahmae NavarraОценок пока нет
- 2019 Early RegistrantsДокумент42 страницы2019 Early RegistrantsMercedita BalgosОценок пока нет
- School Forms (SFS)Документ59 страницSchool Forms (SFS)Rene L. DelovioОценок пока нет
- Authority To Travel: Mabalacat National High SchoolДокумент1 страницаAuthority To Travel: Mabalacat National High SchoolChristian AlejandrinoОценок пока нет
- Senior High E-Records Sheets 1st QuarterДокумент38 страницSenior High E-Records Sheets 1st Quartermarivic r. delos reyesОценок пока нет
- Attendance Sheet For MeetingДокумент1 страницаAttendance Sheet For Meetingpreseah encarnacionОценок пока нет
- Baroque PeriodДокумент17 страницBaroque PeriodJosephine MeguisoОценок пока нет
- HammaДокумент1 страницаHammaJosephine MeguisoОценок пока нет
- Medical For Athletes 2Документ2 страницыMedical For Athletes 2Josephine MeguisoОценок пока нет
- Allas Complaint LetterДокумент1 страницаAllas Complaint LetterJosephine MeguisoОценок пока нет
- Medical For Athletes 2Документ2 страницыMedical For Athletes 2Josephine MeguisoОценок пока нет
- 1.4 Billion People: SymbolismДокумент2 страницы1.4 Billion People: SymbolismJosephine MeguisoОценок пока нет
- Certificate of Recognition: Villarica High SchoolДокумент13 страницCertificate of Recognition: Villarica High SchoolJosephine MeguisoОценок пока нет
- Medical For Athletes 1Документ2 страницыMedical For Athletes 1Josephine MeguisoОценок пока нет
- Translation: What A Beautiful Jasmine Flower What A Beautiful Jasmine FlowerДокумент3 страницыTranslation: What A Beautiful Jasmine Flower What A Beautiful Jasmine FlowerJosephine MeguisoОценок пока нет
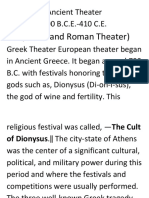
- Ancient TheaterДокумент3 страницыAncient TheaterJosephine MeguisoОценок пока нет
- Master Copy2019-2020Документ2 страницыMaster Copy2019-2020Josephine MeguisoОценок пока нет
- Ancient TheaterДокумент3 страницыAncient TheaterJosephine MeguisoОценок пока нет
- Summat IveДокумент8 страницSummat IveJosephine MeguisoОценок пока нет
- Physical Education?: What IsДокумент42 страницыPhysical Education?: What IsJosephine Meguiso100% (1)
- Allas Complaint LetterДокумент1 страницаAllas Complaint LetterJosephine MeguisoОценок пока нет
- Commendation Letter Praises Renovation WorkmanshipДокумент1 страницаCommendation Letter Praises Renovation WorkmanshipJosephine MeguisoОценок пока нет
- Java's Ancient Shadow Puppet TraditionДокумент22 страницыJava's Ancient Shadow Puppet TraditionJosephine MeguisoОценок пока нет
- K to 12 Health Curriculum GuideДокумент66 страницK to 12 Health Curriculum GuideJinsen Paul MartinОценок пока нет
- Wayang Beber Wayang Klitik Wayang Golek Wayang Topeng Wayang WongДокумент1 страницаWayang Beber Wayang Klitik Wayang Golek Wayang Topeng Wayang WongJosephine MeguisoОценок пока нет
- Music Kto12 CG 1-10 v1.0 PDFДокумент63 страницыMusic Kto12 CG 1-10 v1.0 PDFPrice AquinoОценок пока нет
- K To 12 Physical Education Curriculum GuideДокумент69 страницK To 12 Physical Education Curriculum GuideDr. Joy Kenneth Sala Biasong91% (85)
- Art Curriculum Guide Grades 1-10 December 2013 PDFДокумент93 страницыArt Curriculum Guide Grades 1-10 December 2013 PDFAlly CanaveralОценок пока нет
- K to 12 Health Curriculum GuideДокумент66 страницK to 12 Health Curriculum GuideJinsen Paul MartinОценок пока нет
- K To 12 Physical Education Curriculum GuideДокумент69 страницK To 12 Physical Education Curriculum GuideDr. Joy Kenneth Sala Biasong91% (85)
- Music Kto12 CG 1-10 v1.0 PDFДокумент63 страницыMusic Kto12 CG 1-10 v1.0 PDFPrice AquinoОценок пока нет
- Art Curriculum Guide Grades 1-10 December 2013 PDFДокумент93 страницыArt Curriculum Guide Grades 1-10 December 2013 PDFAlly CanaveralОценок пока нет
- K To 12 Physical Education Curriculum GuideДокумент69 страницK To 12 Physical Education Curriculum GuideDr. Joy Kenneth Sala Biasong91% (85)
- Kan Et Al-2018-Periodontology 2000Документ17 страницKan Et Al-2018-Periodontology 2000Van nguyen hongОценок пока нет
- Billote, CymarcДокумент16 страницBillote, CymarcEllen Bahatan SinahonОценок пока нет
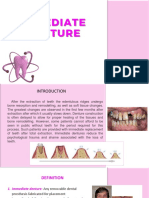
- Immediate DentureДокумент9 страницImmediate Dentureapi-371094867% (3)
- AVILA, Decision Making For Tooth Extraction or ConservationДокумент17 страницAVILA, Decision Making For Tooth Extraction or ConservationKathe LeyvaОценок пока нет
- InterMod OMFSДокумент36 страницInterMod OMFSFahad Qiam75% (4)
- GPNA-BoneSubstituteBrochure Single FINAL PDFДокумент16 страницGPNA-BoneSubstituteBrochure Single FINAL PDFPratyusha VallamОценок пока нет
- Management of Intraocular Foreign BodiesДокумент7 страницManagement of Intraocular Foreign BodiesdebbyОценок пока нет
- Rare Herniation of Buccal Fat Pad into Oral Cavity After Tooth ExtractionДокумент4 страницыRare Herniation of Buccal Fat Pad into Oral Cavity After Tooth ExtractionQuang BuiОценок пока нет
- The Raw Food Diet and Your TeethДокумент117 страницThe Raw Food Diet and Your TeethNeckster Niks100% (5)
- Implant Surgery Complications - Etiology and TreatmentДокумент10 страницImplant Surgery Complications - Etiology and TreatmentStephanie JaramilloОценок пока нет
- Prevention of Post-Extraction PainДокумент8 страницPrevention of Post-Extraction PainThangam VeluОценок пока нет
- Gmhba Member Guide NonvicДокумент37 страницGmhba Member Guide NonvicCarol ColaОценок пока нет
- Reviewer For Perspectives in DentistryДокумент3 страницыReviewer For Perspectives in DentistrySophia Aliyah Miel MacabeoОценок пока нет
- Immediate Denture GuideДокумент19 страницImmediate Denture GuideAyad IbrahimОценок пока нет
- Public Knowledge and Awareness of The Effect of Diabetes Mellitus On Oral HealthДокумент10 страницPublic Knowledge and Awareness of The Effect of Diabetes Mellitus On Oral HealthAnonymous U41F5ISОценок пока нет
- Principles of management of impacted teethДокумент80 страницPrinciples of management of impacted teethdentisdocОценок пока нет
- DentalCertificate PDFДокумент2 страницыDentalCertificate PDFsherlyn de guzmanОценок пока нет
- Comparison of A New Flap Design With The Routinely Used Triangular Flap Design in Third Molar SurgeryДокумент8 страницComparison of A New Flap Design With The Routinely Used Triangular Flap Design in Third Molar SurgeryJean Carlos Barbosa FerreiraОценок пока нет
- An Interview With James A. McNamara Jr.Документ22 страницыAn Interview With James A. McNamara Jr.verhofstadtОценок пока нет
- Dha 022019 PDFДокумент20 страницDha 022019 PDFDrNishchitha K100% (2)
- Fixed functional space maintainer case studyДокумент3 страницыFixed functional space maintainer case studyfelixОценок пока нет
- Treating Complex Non-Skeletal Issues in KidsДокумент11 страницTreating Complex Non-Skeletal Issues in Kidsshahzeb memonОценок пока нет
- J, C Early Vs LateДокумент225 страницJ, C Early Vs LateVenkat ChintadaОценок пока нет
- Corticotomy For Orthodontic Tooth MovementДокумент8 страницCorticotomy For Orthodontic Tooth MovementGissellePantojaОценок пока нет
- Pellegrini 2013 - Surgical Approaches - GTR Vs GBRДокумент14 страницPellegrini 2013 - Surgical Approaches - GTR Vs GBRBryan HeeОценок пока нет
- Transalveolar ExodotiaДокумент57 страницTransalveolar Exodotiakishan100% (1)
- Alveolar Bone Width Preservation After Decoronation of Ankylosed Anterior IncisorsДокумент4 страницыAlveolar Bone Width Preservation After Decoronation of Ankylosed Anterior IncisorsVincent LamadongОценок пока нет
- ProposalДокумент7 страницProposalRANA UsamaОценок пока нет
- Osseointegrasi Pada Perawatan ImplanДокумент8 страницOsseointegrasi Pada Perawatan ImplanMike WazowskiОценок пока нет
- Long-Term Follow Up of 103 Ankylosed Permanent Incisors Surgically Treated With Decoronation - A Retrospective Cohort StudyДокумент7 страницLong-Term Follow Up of 103 Ankylosed Permanent Incisors Surgically Treated With Decoronation - A Retrospective Cohort StudyAnaMariaCastroОценок пока нет