Вам также может понравиться
- SmofKabiven Emulsion For Infusion ENG SMPC - 09001be6801b2eb8Документ11 страницSmofKabiven Emulsion For Infusion ENG SMPC - 09001be6801b2eb8Kirsten HartmanОценок пока нет
- L - Asam Amino+Glukosa+Emulsi Lemak+Elektrolit - DKI1974502349A1 - 2020Документ17 страницL - Asam Amino+Glukosa+Emulsi Lemak+Elektrolit - DKI1974502349A1 - 2020Abu ZidaneОценок пока нет
- Nutriflex Peri MandatoryinformationДокумент5 страницNutriflex Peri MandatoryinformationMafaza KhaisuntahaОценок пока нет
- Nutriflex Lipid 3264periemulsionforinfusion MandatoryinformationДокумент5 страницNutriflex Lipid 3264periemulsionforinfusion MandatoryinformationSwab IndonesiaОценок пока нет
- Update PI BFLUID PTOI - WebsiteДокумент10 страницUpdate PI BFLUID PTOI - WebsiteDietisien MHKNОценок пока нет
- Kabiven G11 PIДокумент13 страницKabiven G11 PIMeidistya Ayu MardhianiОценок пока нет
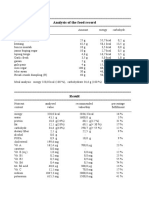
- Analysis of The Food RecordДокумент6 страницAnalysis of The Food RecordAli AkbarОценок пока нет
- Minimal Processing NewДокумент4 страницыMinimal Processing NewRagavi JayaramanОценок пока нет
- Papada de Cerdo USDAДокумент3 страницыPapada de Cerdo USDAMargarita FrancoОценок пока нет
- Nutrition FactsДокумент1 страницаNutrition FactsYaashinie Siva SankarОценок пока нет
- 1 Slice of Ripe Papaya Cup of Mushroom Soup Broth CupДокумент29 страниц1 Slice of Ripe Papaya Cup of Mushroom Soup Broth CupE.J. PelayoОценок пока нет
- Lab Report Whey Protein Isolate Vanilla 1Документ1 страницаLab Report Whey Protein Isolate Vanilla 1sounak SinhaОценок пока нет
- Tugas PKP - Fika Sri AlandaniДокумент3 страницыTugas PKP - Fika Sri AlandaniMuhammad IqbalОценок пока нет
- Gizi Produk Olahan KacangДокумент2 страницыGizi Produk Olahan KacangSalsabilla PutriОценок пока нет
- Development of Media For The Mixotrophic/heterotrophic Culture ofДокумент3 страницыDevelopment of Media For The Mixotrophic/heterotrophic Culture ofTC FreitasОценок пока нет
- Kalabasa Halaya Chapter 2 FinalДокумент16 страницKalabasa Halaya Chapter 2 FinalBryan AustriaОценок пока нет
- Nutriflex LipidДокумент1 страницаNutriflex LipidMarkoMilivojevicОценок пока нет
- NBJДокумент3 страницыNBJAnnisa FitrianiОценок пока нет
- Amount Ingredients: Formulated For Adult Dog MaintenanceДокумент2 страницыAmount Ingredients: Formulated For Adult Dog Maintenanceed drayceОценок пока нет
- Gizi Anak Sekolah 1Документ3 страницыGizi Anak Sekolah 1Fitri WallyОценок пока нет
- Analysis of The Diet PlaДокумент2 страницыAnalysis of The Diet PlaAudylia NoerdaniОценок пока нет
- Analysis of The Food Record For Ghina: BreakfastДокумент4 страницыAnalysis of The Food Record For Ghina: BreakfastiraОценок пока нет
- Gizi Anak Seklah 2Документ3 страницыGizi Anak Seklah 2Fitri WallyОценок пока нет
- Analysis of The Food Record: BreakfastДокумент2 страницыAnalysis of The Food Record: BreakfastAkbar RizkaОценок пока нет
- Hasil Perhitungan Diet/: Sarapan Nasi PutihДокумент4 страницыHasil Perhitungan Diet/: Sarapan Nasi Putihikra ramadhanОценок пока нет
- Hasil Perhitungan Diet/: Sarapan Nasi PutihДокумент4 страницыHasil Perhitungan Diet/: Sarapan Nasi Putihikra ramadhanОценок пока нет
- Low-Carbohydrates DietДокумент17 страницLow-Carbohydrates Dietjanessen caliyoОценок пока нет
- Analysis of The Food RecordДокумент2 страницыAnalysis of The Food RecordSokap TuchОценок пока нет
- Contoh Analisis NutrisurveyДокумент2 страницыContoh Analisis NutrisurveyRr. Annisa AyuningtyasОценок пока нет
- Amount Ingredients: Now E Oil NOW Kelp PowderДокумент2 страницыAmount Ingredients: Now E Oil NOW Kelp Powdered drayceОценок пока нет
- Spec Sheet 09716Документ1 страницаSpec Sheet 09716bcrapoОценок пока нет
- Analysis of The Food Record For Ghina: BreakfastДокумент6 страницAnalysis of The Food Record For Ghina: BreakfastiraОценок пока нет
- Recall Monev 1Документ2 страницыRecall Monev 1tugasandskripinaОценок пока нет
- RecallДокумент3 страницыRecallRohma YuliaОценок пока нет
- NS AzizahДокумент18 страницNS AzizahAzizah DJОценок пока нет
- Menu Anemia Dan Kek (Bentuk Makanan Biasa) (Risnaika Dewi Ayuni G0B017012)Документ3 страницыMenu Anemia Dan Kek (Bentuk Makanan Biasa) (Risnaika Dewi Ayuni G0B017012)Risna IkaОценок пока нет
- Analysis of The Food RecordДокумент2 страницыAnalysis of The Food RecordSokap TuchОценок пока нет
- Analysis of The Food RecordДокумент4 страницыAnalysis of The Food Recordoryza dwi nandaОценок пока нет
- Dry FruitsДокумент30 страницDry FruitskgsbhavaniprasadОценок пока нет
- B Oreo 25 LB Cookie Medium Cookie Pieces Fs Case Sold in CDN and UsДокумент2 страницыB Oreo 25 LB Cookie Medium Cookie Pieces Fs Case Sold in CDN and UsAbby Adriano CosicoОценок пока нет
- Nutriflex Lipid Peri PDFДокумент9 страницNutriflex Lipid Peri PDFAulia KpОценок пока нет
- Reference For Computation of Nutrition Facts Product: Coconut Cream PowderДокумент5 страницReference For Computation of Nutrition Facts Product: Coconut Cream Powdermashuri72Оценок пока нет
- Recall Kasus Harian 1Документ2 страницыRecall Kasus Harian 1NikitaОценок пока нет
- Supplemental Recipe: Perfectly Rawsome Vip MembershipДокумент4 страницыSupplemental Recipe: Perfectly Rawsome Vip MembershipGaby BegetОценок пока нет
- Analysis of The Food Record For Ghina: BreakfastДокумент5 страницAnalysis of The Food Record For Ghina: BreakfastiraОценок пока нет
- Gizi Anak SeklahДокумент3 страницыGizi Anak SeklahFitri WallyОценок пока нет
- Analysis of The Food Record: Pagi Nasi PutihДокумент3 страницыAnalysis of The Food Record: Pagi Nasi PutihNy NyОценок пока нет
- Analysis of The Food Record: BreakfastДокумент2 страницыAnalysis of The Food Record: BreakfastAprianinur SafariantiОценок пока нет
- Nutri Intervensi 3Документ2 страницыNutri Intervensi 3Aprianinur SafariantiОценок пока нет
- Hasil Perhitungan Diet/: Sarapan Nasi Goreng KombinasiДокумент4 страницыHasil Perhitungan Diet/: Sarapan Nasi Goreng Kombinasiikra ramadhanОценок пока нет
- Recall NY Sri EmaliaДокумент2 страницыRecall NY Sri EmaliafifiОценок пока нет
- ChirugiaBariatrica ENG R0-010822Документ34 страницыChirugiaBariatrica ENG R0-010822ahmed yahyaОценок пока нет
- Prolupin - Datasheet - 10102 Lupine Protein Isolate, FreshДокумент3 страницыProlupin - Datasheet - 10102 Lupine Protein Isolate, FreshJaved Khan Nadir KhanОценок пока нет
- Analysis of The Food Record: Makan SiangДокумент4 страницыAnalysis of The Food Record: Makan Siangfirda auliyaОценок пока нет
- Recall Hari 1 Ny KДокумент2 страницыRecall Hari 1 Ny KAnonymous wXozTaОценок пока нет
- Analysis of The Food Record: BreakfastДокумент2 страницыAnalysis of The Food Record: BreakfastAkbar RizkaОценок пока нет
- Nutri Dietetika 2023Документ2 страницыNutri Dietetika 2023Hilya SalmaОценок пока нет
- Analysis of The Food RecordДокумент2 страницыAnalysis of The Food Recordnurma jumatinОценок пока нет
- Peptamen Junior Liquid Data Card April 2019Документ2 страницыPeptamen Junior Liquid Data Card April 2019Dwi ApriliziaОценок пока нет
- Photo Guide HalodocДокумент8 страницPhoto Guide HalodocBobbyОценок пока нет
- Pil 880 PDFДокумент6 страницPil 880 PDFBobbyОценок пока нет
- Martin2015 PDFДокумент16 страницMartin2015 PDFBobbyОценок пока нет
- 120002677E v02 SD BIOLINE Malaria RDT Series - BrochureДокумент4 страницы120002677E v02 SD BIOLINE Malaria RDT Series - BrochureBobbyОценок пока нет
- ICT LegalEthical Issue PowerPoint PresentationДокумент4 страницыICT LegalEthical Issue PowerPoint PresentationReydan MaraveОценок пока нет
- Case Study Diverticulosis PaperДокумент12 страницCase Study Diverticulosis Paperapi-381128376100% (3)
- Statistical TestsДокумент47 страницStatistical TestsUche Nwa ElijahОценок пока нет
- EP105Use of English ArantxaReynosoДокумент6 страницEP105Use of English ArantxaReynosoArantxaSteffiОценок пока нет
- A Portrayal of Gender and A Description of Gender Roles in SelectДокумент429 страницA Portrayal of Gender and A Description of Gender Roles in SelectPtah El100% (1)
- Theology and Pipe Smoking - 7pДокумент7 страницTheology and Pipe Smoking - 7pNeimar HahmeierОценок пока нет
- NAT FOR GRADE 12 (MOCK TEST) Language and CommunicationДокумент6 страницNAT FOR GRADE 12 (MOCK TEST) Language and CommunicationMonica CastroОценок пока нет
- 100 Commonly Asked Interview QuestionsДокумент6 страниц100 Commonly Asked Interview QuestionsRaluca SanduОценок пока нет
- TreeAgePro 2013 ManualДокумент588 страницTreeAgePro 2013 ManualChristian CifuentesОценок пока нет
- Consolidated PCU Labor Law Review 1st Batch Atty Jeff SantosДокумент36 страницConsolidated PCU Labor Law Review 1st Batch Atty Jeff SantosJannah Mae de OcampoОценок пока нет
- Chapter 2Документ16 страницChapter 2nannaОценок пока нет
- AD&D 2nd Edition - Dark Sun - Monstrous Compendium - Appendix II - Terrors Beyond Tyr PDFДокумент130 страницAD&D 2nd Edition - Dark Sun - Monstrous Compendium - Appendix II - Terrors Beyond Tyr PDFWannes Ikkuhyu100% (8)
- Software Development Life CycleДокумент70 страницSoftware Development Life CycleChaitanya MalikОценок пока нет
- 01 History of Grammatical StudyДокумент9 страниц01 History of Grammatical StudyRomanОценок пока нет
- Total Recall and SkepticismДокумент4 страницыTotal Recall and Skepticismdweiss99Оценок пока нет
- NIPMR Notification v3Документ3 страницыNIPMR Notification v3maneeshaОценок пока нет
- Mohit Maru 4th Semester Internship ReportДокумент11 страницMohit Maru 4th Semester Internship ReportAdhish ChakrabortyОценок пока нет
- Dwnload Full Conceptual Physics 12th Edition Hewitt Test Bank PDFДокумент36 страницDwnload Full Conceptual Physics 12th Edition Hewitt Test Bank PDFscreamsoaring.pm7hcv100% (13)
- Baby Brianna Andrew WaltersДокумент14 страницBaby Brianna Andrew WaltersBaby Brianna50% (2)
- Hanum at PanchaДокумент5 страницHanum at PanchaMahadeva MishraОценок пока нет
- The Impact of Video Gaming To The Academic Performance of The Psychology Students in San Beda UniversityДокумент5 страницThe Impact of Video Gaming To The Academic Performance of The Psychology Students in San Beda UniversityMarky Laury GameplaysОценок пока нет
- Item Bank - Science 5 - 2ND QuarterДокумент11 страницItem Bank - Science 5 - 2ND QuarterJasmine AguilaОценок пока нет
- Tutorials in Complex Photonic Media SPIE Press Monograph Vol PM194 PDFДокумент729 страницTutorials in Complex Photonic Media SPIE Press Monograph Vol PM194 PDFBadunoniОценок пока нет
- Sabena Belgian World Airlines vs. CAДокумент3 страницыSabena Belgian World Airlines vs. CARhea CalabinesОценок пока нет
- Di Franco Amended Factum 2021-05-03Документ30 страницDi Franco Amended Factum 2021-05-03Michael BueckertОценок пока нет
- Climate Change Myth or Reality A Critical Analysis of Mainstream English Dailies of India-2019-03!14!09-34Документ13 страницClimate Change Myth or Reality A Critical Analysis of Mainstream English Dailies of India-2019-03!14!09-34Impact JournalsОценок пока нет
- Project Report Format CSE DEPTДокумент16 страницProject Report Format CSE DEPTAnkush KoundalОценок пока нет
- InfoVista Xeus Pro 5 TMR Quick GuideДокумент76 страницInfoVista Xeus Pro 5 TMR Quick GuideNguyen Dang KhanhОценок пока нет
- Final BasantДокумент22 страницыFinal BasantMuqaddas IsrarОценок пока нет