Вам также может понравиться
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5795)
- 1 s2.0 S1201971216310244 MainДокумент2 страницы1 s2.0 S1201971216310244 Mainnurahmi widyani ratriОценок пока нет
- 12 - Chronic Care ManagementДокумент54 страницы12 - Chronic Care Managementnurahmi widyani ratriОценок пока нет
- Kesici 2019Документ7 страницKesici 2019nurahmi widyani ratriОценок пока нет
- Changes in Contrast Sensitivity in Young Adults With DiabetesДокумент5 страницChanges in Contrast Sensitivity in Young Adults With Diabetesnurahmi widyani ratriОценок пока нет
- Trauma ServikalДокумент7 страницTrauma Servikalnurahmi widyani ratriОценок пока нет
- Nihms 604943Документ15 страницNihms 604943nurahmi widyani ratriОценок пока нет
- Muchiri 2016Документ10 страницMuchiri 2016nurahmi widyani ratriОценок пока нет
- JBI Quasi-Experimental Appraisal Tool2017Документ7 страницJBI Quasi-Experimental Appraisal Tool2017nurahmi widyani ratriОценок пока нет
- V. Mallikarjun RaoДокумент6 страницV. Mallikarjun Raonurahmi widyani ratriОценок пока нет
- STROBE Statement-Checklist of Items That Should Be Included in Reports of Case-Control StudiesДокумент10 страницSTROBE Statement-Checklist of Items That Should Be Included in Reports of Case-Control Studiesnurahmi widyani ratriОценок пока нет
- Rundown Acara AДокумент5 страницRundown Acara Anurahmi widyani ratriОценок пока нет
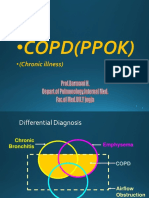
- Differential Staining of Ocular Goblet CellsДокумент5 страницDifferential Staining of Ocular Goblet Cellsnurahmi widyani ratriОценок пока нет
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (400)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- TX 1 Abs at TX 2 Abs atДокумент3 страницыTX 1 Abs at TX 2 Abs atNagita NabilaОценок пока нет
- NURS2002 Assignment 4 Case-Study Instructions 2019 PDFДокумент2 страницыNURS2002 Assignment 4 Case-Study Instructions 2019 PDFjohnmccauleyОценок пока нет
- Discovery 2020Документ6 страницDiscovery 2020BusinessTech100% (1)
- Adult Early Warning Score Observation Chart For Cardiology UnitДокумент1 страницаAdult Early Warning Score Observation Chart For Cardiology UnitalexipsОценок пока нет
- Research # 1: Laguna State Polytechnic UniversityДокумент10 страницResearch # 1: Laguna State Polytechnic UniversityAbigael Patricia GutierrezОценок пока нет
- DR AbcДокумент9 страницDR AbcAnonymousОценок пока нет
- APA - DSM5 - Level 1 Measure Child Age 11 To 17 PDFДокумент3 страницыAPA - DSM5 - Level 1 Measure Child Age 11 To 17 PDFdavidhoracioОценок пока нет
- Antenatal SteroidsДокумент30 страницAntenatal Steroidskhadzx100% (2)
- The Efficacy of Venlafaxine, Flunarizine, and Valproic Acid in The Prophylaxis of Vestibular MigraineДокумент5 страницThe Efficacy of Venlafaxine, Flunarizine, and Valproic Acid in The Prophylaxis of Vestibular MigraineagustianaОценок пока нет
- Perception DisordersДокумент4 страницыPerception DisordersSabi HassanОценок пока нет
- TelemedicineДокумент39 страницTelemedicineraju raj100% (1)
- Vitamin C Pamphlet PDFДокумент2 страницыVitamin C Pamphlet PDFgreeenbee100% (2)
- Pulmonary EdemaДокумент10 страницPulmonary EdemaNader Smadi100% (6)
- 2 Hand HygieneДокумент44 страницы2 Hand HygieneAdelina SilimonОценок пока нет
- Massive Transfusion ProtocolДокумент2 страницыMassive Transfusion ProtocolmukriОценок пока нет
- Cardio DrillДокумент24 страницыCardio DrillDemuel Dee L. BertoОценок пока нет
- DM Reporting ZДокумент52 страницыDM Reporting ZZsazsaОценок пока нет
- 2 CPAP and NIV HelmetsДокумент8 страниц2 CPAP and NIV HelmetsjvalgalОценок пока нет
- PRIMARY TYPE 2 DiabetesДокумент33 страницыPRIMARY TYPE 2 DiabetesPunam Patel100% (1)
- Inlays and Onlays ReportДокумент32 страницыInlays and Onlays ReportAlnielJoManlapigОценок пока нет
- Bell''s PalsyДокумент54 страницыBell''s Palsywahyu_sitaОценок пока нет
- Small Incision CholecystectomyДокумент8 страницSmall Incision CholecystectomyCatalin SavinОценок пока нет
- Medical Management of Missed AbortionДокумент4 страницыMedical Management of Missed AbortionJonathan San MartinОценок пока нет
- B30 SpecsДокумент4 страницыB30 SpecsChristian Garcia100% (1)
- Neural Retraining Project Highlights: Completion of First Phase Informs Creation of Clinical Trials ProtocolДокумент2 страницыNeural Retraining Project Highlights: Completion of First Phase Informs Creation of Clinical Trials ProtocolDeepak RanaОценок пока нет
- Hospital Information SystemДокумент12 страницHospital Information SystemUcu YeuhzОценок пока нет
- Project ProposalДокумент2 страницыProject ProposalDrmonisha MhaОценок пока нет
- 2012 FDA - Warning Letter To Home Care Technologies USA, IncДокумент4 страницы2012 FDA - Warning Letter To Home Care Technologies USA, IncWhatYou HaventSeenОценок пока нет
- Hospital Standards For Accreditation For Afghanistan Hosp - Standards - PharmacyДокумент10 страницHospital Standards For Accreditation For Afghanistan Hosp - Standards - PharmacyMaria Camila100% (1)
- Blood Groups: DR - Agus Alim Abdullah, SPPK (K)Документ60 страницBlood Groups: DR - Agus Alim Abdullah, SPPK (K)Salim JufriОценок пока нет