Вам также может понравиться
- The Jewish Way in Death and MourningДокумент67 страницThe Jewish Way in Death and Mourningizzy212100% (1)
- The Assignment Vol.4 - The Pain - Mike Murdock PDFДокумент168 страницThe Assignment Vol.4 - The Pain - Mike Murdock PDFEmmanuel Temiloluwa67% (3)
- Health Insurance BookДокумент3 страницыHealth Insurance BookHarish SihareОценок пока нет
- CS1 Epoxy Curing AgentsДокумент21 страницаCS1 Epoxy Curing AgentsAlptekin100% (1)
- Exploring Patient Safety Culture in Emergency DepartmentsДокумент7 страницExploring Patient Safety Culture in Emergency Departmentsmuhammad ismailОценок пока нет
- Fan Tool Kit - Ad Hoc Group - V4ddДокумент121 страницаFan Tool Kit - Ad Hoc Group - V4ddhmaza shakeelОценок пока нет
- L-6th Sem (Eng Notes) Law Relating To Women and ChildДокумент52 страницыL-6th Sem (Eng Notes) Law Relating To Women and ChildCuriae corporate consultantsОценок пока нет
- Comparative Study of DEA and MDEAДокумент4 страницыComparative Study of DEA and MDEAsaleh4060Оценок пока нет
- FBS Q1 WK1Документ4 страницыFBS Q1 WK1Nicole Eve Pelaez-AbarrientosОценок пока нет
- Epidemiology ReviewДокумент10 страницEpidemiology ReviewSaurabhОценок пока нет
- Pressure Ulcer PreventionДокумент11 страницPressure Ulcer PreventionChi ChangОценок пока нет
- Summary (Adjuncts)Документ2 страницыSummary (Adjuncts)Ngọc MinhОценок пока нет
- Adverse Events in Healthcare A Literature ReviewДокумент4 страницыAdverse Events in Healthcare A Literature Revieweeyjzkwgf100% (1)
- Journal Pone 0249531Документ16 страницJournal Pone 0249531Integração da Assistência à Saúde Militar (INASMIL)Оценок пока нет
- Real ProposalДокумент16 страницReal ProposalAlamgir Khan YousafzaiОценок пока нет
- The Association of Nursing Workloads, Organizational, and Individual Factors With Adverse Patient OutcomeДокумент9 страницThe Association of Nursing Workloads, Organizational, and Individual Factors With Adverse Patient OutcomeWilfred JavierОценок пока нет
- Review: The Ef Ficacy and Safety of Probiotics in People With Cancer: A Systematic ReviewДокумент11 страницReview: The Ef Ficacy and Safety of Probiotics in People With Cancer: A Systematic ReviewNatália LopesОценок пока нет
- 2017 Article 168Документ15 страниц2017 Article 168Rui Pedro PereiraОценок пока нет
- 2015 Article 37 Kontraasepsi OralДокумент10 страниц2015 Article 37 Kontraasepsi OralmemeeeyyyОценок пока нет
- Jurnal LainДокумент22 страницыJurnal LainBudi ArsanaОценок пока нет
- Terapi H5N1Документ6 страницTerapi H5N1davidperdanaОценок пока нет
- 77d8 PDFДокумент7 страниц77d8 PDFRosyid PrasetyoОценок пока нет
- 01 Risk in Pediatric AnesthesiaДокумент11 страниц01 Risk in Pediatric AnesthesiaOmar Sanchez PazОценок пока нет
- Estimation of Population-Based Incidence of Pregnancy-Related Illness and Mortality (PRIAM) in Two Districts in West Java, IndonesiaДокумент10 страницEstimation of Population-Based Incidence of Pregnancy-Related Illness and Mortality (PRIAM) in Two Districts in West Java, IndonesiaSeptina Esthy AyuОценок пока нет
- WOUND CARE Prevention and Early Detection of Pressure Ulcers in Hospitalized PatientsДокумент11 страницWOUND CARE Prevention and Early Detection of Pressure Ulcers in Hospitalized PatientsToye AdeolaОценок пока нет
- WFCCN Chapter 4 Safety-and-Quality-in-the-ICU 2nd EditionДокумент13 страницWFCCN Chapter 4 Safety-and-Quality-in-the-ICU 2nd EditionJuan Carlos Mora TorresОценок пока нет
- Management Vol1 Issue2 Article 8Документ45 страницManagement Vol1 Issue2 Article 8martin ariawanОценок пока нет
- 32 01 09 GrazinaДокумент16 страниц32 01 09 GrazinaDisty AОценок пока нет
- Bakker 2012Документ10 страницBakker 2012ieoОценок пока нет
- British Journal of Clinical PharmacologyДокумент6 страницBritish Journal of Clinical PharmacologyJunerey Hume Torres RodriguezОценок пока нет
- 10 1016@j Ijnurstu 2019 103449Документ24 страницы10 1016@j Ijnurstu 2019 103449mahrani_adrinОценок пока нет
- Journal Critique Jericho S. Javier, R.N. 16 November 2013 Master of Arts in Nursing Dr. Bella G. PanlilioДокумент5 страницJournal Critique Jericho S. Javier, R.N. 16 November 2013 Master of Arts in Nursing Dr. Bella G. PanlilioEköw Santiago JavierОценок пока нет
- CarlsДокумент14 страницCarlsvcutph24Оценок пока нет
- Rheumatology: Real-World Incidence and Prevalence of Low Back Pain Using Routinely Collected DataДокумент8 страницRheumatology: Real-World Incidence and Prevalence of Low Back Pain Using Routinely Collected DataAmanda GómezОценок пока нет
- Risk Factors For Falls in Hospital In-Patients: A Prospective Nested Case Control StudyДокумент7 страницRisk Factors For Falls in Hospital In-Patients: A Prospective Nested Case Control StudyNurhasanah HaryaniОценок пока нет
- IJC 9999 NaДокумент29 страницIJC 9999 NaSimona VisanОценок пока нет
- Ugandan Pregnant and New Mothers' Perceptions, Knowledge, and Information Sources On COVID-19 at Jinja Regional Referral HospitalДокумент11 страницUgandan Pregnant and New Mothers' Perceptions, Knowledge, and Information Sources On COVID-19 at Jinja Regional Referral HospitalKIU PUBLICATION AND EXTENSIONОценок пока нет
- Alqenae 2020 - Prevalencia de Los Errores de MedicacionДокумент21 страницаAlqenae 2020 - Prevalencia de Los Errores de MedicacionJuan camiloОценок пока нет
- Risk in Pediatric Anesthesia PDFДокумент10 страницRisk in Pediatric Anesthesia PDFWisnu PratamaОценок пока нет
- NIH Public Access: Author ManuscriptДокумент22 страницыNIH Public Access: Author ManuscriptHumberto QuimeОценок пока нет
- Farmacos en AncianosДокумент12 страницFarmacos en AncianosKarina Alexandra Vera-Pinto EstacioОценок пока нет
- Improving Medication Safety: Development and Impact of A Multivariate Model-Based Strategy To Target High-Risk PatientsДокумент13 страницImproving Medication Safety: Development and Impact of A Multivariate Model-Based Strategy To Target High-Risk PatientstotoksaptantoОценок пока нет
- UlcerДокумент5 страницUlcerabriyahОценок пока нет
- Infection Control & Hospital EpidemiologyДокумент9 страницInfection Control & Hospital EpidemiologyRianОценок пока нет
- Severe Sepsis-Associated Morbidity and Mortality Among Critically Ill Children With CancerДокумент8 страницSevere Sepsis-Associated Morbidity and Mortality Among Critically Ill Children With CancerFaki D'pasnizerОценок пока нет
- Huang 2019Документ10 страницHuang 2019blume diaОценок пока нет
- 2019 - Härkänen Et AlДокумент8 страниц2019 - Härkänen Et AlazeemathmariyamОценок пока нет
- The Knowledge of Pressure Ulcer Among Nursing Students and Related FactorsДокумент23 страницыThe Knowledge of Pressure Ulcer Among Nursing Students and Related FactorsUrmisha DasОценок пока нет
- A 0240105Документ5 страницA 0240105International Organization of Scientific Research (IOSR)Оценок пока нет
- Risk Factors For Drug-Resistant Streptococcus Pneumoniae and Antibiotic Prescribing Practices in Outpatient Community-Acquired PneumoniaДокумент4 страницыRisk Factors For Drug-Resistant Streptococcus Pneumoniae and Antibiotic Prescribing Practices in Outpatient Community-Acquired PneumoniakingkinresmytaОценок пока нет
- Running Head: Research Proposal 1Документ24 страницыRunning Head: Research Proposal 1Hogan ObiОценок пока нет
- 43 FullДокумент9 страниц43 Fullnayeta levi syahdanaОценок пока нет
- Development of A List of High-Risk Perioperative Medications For The Elderly: A Delphi MethodДокумент8 страницDevelopment of A List of High-Risk Perioperative Medications For The Elderly: A Delphi Methodfabian arassiОценок пока нет
- Diagnostic Errors - UpToDateДокумент23 страницыDiagnostic Errors - UpToDateJoyce SumagaysayОценок пока нет
- 1 s2.0 S2049080121000595 Main1Документ6 страниц1 s2.0 S2049080121000595 Main1Devina ArrandhikasariОценок пока нет
- 25FirouzAmani EtalДокумент6 страниц25FirouzAmani EtaleditorijmrhsОценок пока нет
- Yang 2014Документ11 страницYang 2014Shafar SoliwuntoОценок пока нет
- Evidence For Person-Centred Care in Chronic Wound Care: A Systematic Review and Recommendations For PracticeДокумент24 страницыEvidence For Person-Centred Care in Chronic Wound Care: A Systematic Review and Recommendations For Practiceananda khairulОценок пока нет
- Jurnal BTKV DodiДокумент10 страницJurnal BTKV DodiAchmad Dodi MeidiantoОценок пока нет
- Kumpulan Jurnal InternasionalДокумент15 страницKumpulan Jurnal InternasionalTIKAОценок пока нет
- Journal Pre-Proof: European Journal of Paediatric NeurologyДокумент31 страницаJournal Pre-Proof: European Journal of Paediatric NeurologySebastian SalvadorОценок пока нет
- Research ToolДокумент15 страницResearch Toolmayur.polОценок пока нет
- Clinical Manifestations of Human Brucellosis: A Systematic Review and Meta-AnalysisДокумент9 страницClinical Manifestations of Human Brucellosis: A Systematic Review and Meta-AnalysisgustiОценок пока нет
- Optimizing Delirium Prediction Model in The Management of Hospitalized Elderly PatientsДокумент2 страницыOptimizing Delirium Prediction Model in The Management of Hospitalized Elderly Patientspeni_dwiОценок пока нет
- Bergquist Beringer2013Документ11 страницBergquist Beringer2013wennyОценок пока нет
- Journal Pre-Proof: Journal of Critical CareДокумент26 страницJournal Pre-Proof: Journal of Critical CareMohamed Ben RejebОценок пока нет
- International Journal of Nursing StudiesДокумент9 страницInternational Journal of Nursing StudiesAprilina P SОценок пока нет
- Supportive Care in Pediatric Oncology: A Practical Evidence-Based ApproachОт EverandSupportive Care in Pediatric Oncology: A Practical Evidence-Based ApproachJames H. FeusnerОценок пока нет
- Upper Tract Urothelial CarcinomaОт EverandUpper Tract Urothelial CarcinomaShahrokh F. ShariatОценок пока нет
- Efektifitas Latihan Progressive Muscle Relaxation (PMR) Terhadap Mual Muntah Kemoterapi Pasien Kanker OvariumДокумент8 страницEfektifitas Latihan Progressive Muscle Relaxation (PMR) Terhadap Mual Muntah Kemoterapi Pasien Kanker OvariumMutmin AnsariОценок пока нет
- 10.1177 0300060516638991Документ8 страниц10.1177 0300060516638991Ahmad HafiОценок пока нет
- JurnalДокумент11 страницJurnalAhmad HafiОценок пока нет
- 136 1456411712 PDFДокумент7 страниц136 1456411712 PDFGabriel KlemensОценок пока нет
- R5!Документ6 страницR5!Dyah Paramudita RaharjoОценок пока нет
- 34 68 1 SM PDFДокумент6 страниц34 68 1 SM PDFAhmad HafiОценок пока нет
- Short-Term Effects of Kinesio Taping in Women With Pregnancy-Related Low Back Pain: A Randomized Controlled Clinical TrialДокумент5 страницShort-Term Effects of Kinesio Taping in Women With Pregnancy-Related Low Back Pain: A Randomized Controlled Clinical TrialAhmad HafiОценок пока нет
- 12 24 1 SMДокумент11 страниц12 24 1 SMDrie8Оценок пока нет
- Impact of Kinesio Taping Application On Pregnant WДокумент7 страницImpact of Kinesio Taping Application On Pregnant WAhmad HafiОценок пока нет
- Aggression Self Control Pada Pasien Dengan: Efektifitas Senam Aerobic Low Impact Terhadap Resiko Perilaku KekerasanДокумент9 страницAggression Self Control Pada Pasien Dengan: Efektifitas Senam Aerobic Low Impact Terhadap Resiko Perilaku KekerasanaraahОценок пока нет
- 2529 10019 1 PBДокумент9 страниц2529 10019 1 PBSii KecilОценок пока нет
- Aggression Self Control Pada Pasien Dengan: Efektifitas Senam Aerobic Low Impact Terhadap Resiko Perilaku KekerasanДокумент9 страницAggression Self Control Pada Pasien Dengan: Efektifitas Senam Aerobic Low Impact Terhadap Resiko Perilaku KekerasanaraahОценок пока нет
- Complementary Alternative Medicinepada: NERS JURNAL KEPERAWATAN, Volume 12, No.1, Maret 2016, (Hal 14-22)Документ9 страницComplementary Alternative Medicinepada: NERS JURNAL KEPERAWATAN, Volume 12, No.1, Maret 2016, (Hal 14-22)nonika sianturiОценок пока нет
- JurnalДокумент5 страницJurnalAhmad HafiОценок пока нет
- Terapi Aktivitas Kelompok (Tak) Stimulasi Persepsi Terhadap Kemampuan Pasien Mengontrol HalusinasiДокумент6 страницTerapi Aktivitas Kelompok (Tak) Stimulasi Persepsi Terhadap Kemampuan Pasien Mengontrol HalusinasiDella Nur'ainiОценок пока нет
- Rian UthamiДокумент18 страницRian UthamiAhmad HafiОценок пока нет
- JurnalДокумент9 страницJurnalAhmad HafiОценок пока нет
- Health-Related Quality of Life in Intensive Care Survivors: Associations With Social Support, Comorbidity, and Pain InterferenceДокумент14 страницHealth-Related Quality of Life in Intensive Care Survivors: Associations With Social Support, Comorbidity, and Pain InterferenceAhmad HafiОценок пока нет
- Aaa PAPATHANASSOGLOU Kemajuan Penelitian Dalam Perawatan Kritis Menargetkan Hasil Fisiologis Dan Psikologis PasienДокумент2 страницыAaa PAPATHANASSOGLOU Kemajuan Penelitian Dalam Perawatan Kritis Menargetkan Hasil Fisiologis Dan Psikologis PasienAhmad HafiОценок пока нет
- Jurnal Internasional Life Threatening Illness in PoДокумент8 страницJurnal Internasional Life Threatening Illness in PoAhmad HafiОценок пока нет
- Impact of Kinesio Taping Application On Pregnant WДокумент7 страницImpact of Kinesio Taping Application On Pregnant WAhmad HafiОценок пока нет
- LI, QIAN Efektivitas Protokol Makan Enteral Pada Hasil Klinis Pada Pasien Sakit Kritis A Sebelum Dan Sesudah StudiДокумент17 страницLI, QIAN Efektivitas Protokol Makan Enteral Pada Hasil Klinis Pada Pasien Sakit Kritis A Sebelum Dan Sesudah StudiAhmad HafiОценок пока нет
- Woc Kista OvariumДокумент1 страницаWoc Kista OvariumAhmad HafiОценок пока нет
- Pengalaman Komunikasi Terapeutik Perawat Orang Lanjut Usia: Antar Venus Dina NabilahДокумент12 страницPengalaman Komunikasi Terapeutik Perawat Orang Lanjut Usia: Antar Venus Dina Nabilahagustiawan28Оценок пока нет
- Brikker (Pengaruh Gangguan Keseimbangan Elektrolit Terhadap Fungsi Sistem Cardiovascular. Review of The Literature) .Документ3 страницыBrikker (Pengaruh Gangguan Keseimbangan Elektrolit Terhadap Fungsi Sistem Cardiovascular. Review of The Literature) .Ahmad HafiОценок пока нет
- Apjon 4 162Документ6 страницApjon 4 162Ahmad HafiОценок пока нет
- Incremental Cost of Cardiovascular Disease, Hypertension, and Pain For Patients With Diabetes MellitusДокумент2 страницыIncremental Cost of Cardiovascular Disease, Hypertension, and Pain For Patients With Diabetes MellitusAhmad HafiОценок пока нет
- Rian UthamiДокумент18 страницRian UthamiAhmad HafiОценок пока нет
- Prioritas Ilmu Keperawatan Kardiovaskular Tentang Keperawatan Kardiovaskular Dan Stroke.Документ3 страницыPrioritas Ilmu Keperawatan Kardiovaskular Tentang Keperawatan Kardiovaskular Dan Stroke.Ahmad HafiОценок пока нет
- EcodesДокумент2 страницыEcodesValentin IonutОценок пока нет
- Exam G-9 CookeryДокумент5 страницExam G-9 Cookeryaileenarcabal01Оценок пока нет
- AssaultДокумент12 страницAssaultEd Mundo100% (3)
- Ableism - What It Is and Why It Matters To EveryoneДокумент28 страницAbleism - What It Is and Why It Matters To Everyonellemma admasОценок пока нет
- Winchester Model 9422 Lever Action Rifle Owner's Manual: LicenseeДокумент0 страницWinchester Model 9422 Lever Action Rifle Owner's Manual: Licenseecarlosfanjul1Оценок пока нет
- AT-502 - AT-504 - OM-0-Introduction-1 - 10-12-2019Документ6 страницAT-502 - AT-504 - OM-0-Introduction-1 - 10-12-2019Vinicius RodriguesОценок пока нет
- Using The Time Domain Reflectometer To Check For and Locate A FaultДокумент5 страницUsing The Time Domain Reflectometer To Check For and Locate A FaultSikandar MasoodОценок пока нет
- CombinedList PDFДокумент3 страницыCombinedList PDFMarie BautistaОценок пока нет
- 900 ADA - Rev13Документ306 страниц900 ADA - Rev13Miguel Ignacio Roman BarreraОценок пока нет
- The Information Age CHAPTER 7 StsДокумент7 страницThe Information Age CHAPTER 7 StsAngel FlordelizaОценок пока нет
- Major Head of AccountsДокумент9 страницMajor Head of AccountsArun EmmiОценок пока нет
- Job Satisfaction and Professional Ethics Practices in Public SectorДокумент13 страницJob Satisfaction and Professional Ethics Practices in Public SectorMuhammad NafeesОценок пока нет
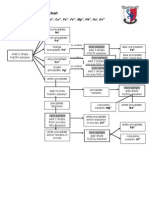
- Testing For Cations Flow ChartДокумент2 страницыTesting For Cations Flow Chartapi-252561013Оценок пока нет
- Astm D 1142Документ11 страницAstm D 1142yusria1982Оценок пока нет
- AFC Refereeing Fitness Training Guidelines - FinalДокумент42 страницыAFC Refereeing Fitness Training Guidelines - FinalAPH FARM BONDOWOSOОценок пока нет
- A211 Reading Set A QuestionДокумент12 страницA211 Reading Set A Questiontasya zakariaОценок пока нет
- Exp 4 Centrifugal CompressorДокумент11 страницExp 4 Centrifugal CompressorFaris HamirОценок пока нет
- Glycerin As A Renewable Feedstock For EpichlorohydДокумент6 страницGlycerin As A Renewable Feedstock For EpichlorohydMuhammad RidhauddinОценок пока нет
- J Jacadv 2022 100034Документ14 страницJ Jacadv 2022 100034Rui FonteОценок пока нет
- 6 Human Diseases That Cause by VirusesДокумент7 страниц6 Human Diseases That Cause by VirusesJefry JapОценок пока нет
- Good Boys Go To Heaven, Bad Boys Go EverywhereДокумент32 страницыGood Boys Go To Heaven, Bad Boys Go Everywherealcantaravic2006Оценок пока нет