Вам также может понравиться
- PBQ Scoring KeyДокумент1 страницаPBQ Scoring KeyWendi ChinchayanОценок пока нет
- Hemophilia and Von Willebrand Disease EmergenciesДокумент13 страницHemophilia and Von Willebrand Disease EmergenciesDobrila SimonovicОценок пока нет
- Condensed Mcmdm1-Vwd BleedingДокумент8 страницCondensed Mcmdm1-Vwd BleedingPatmasariОценок пока нет
- Physician or Clinic Coordinating NOAC Treatment Important Patient Instructions What To Do in Certain Occasions Information For Healthcare ProvidersДокумент2 страницыPhysician or Clinic Coordinating NOAC Treatment Important Patient Instructions What To Do in Certain Occasions Information For Healthcare ProvidersgabrimarteОценок пока нет
- Drug StudyДокумент10 страницDrug StudyJeraldine GumpalОценок пока нет
- Narce Sn-Ii, Nocete Sn-Ii NCM 109-n (RLE) BSN-2A Instructor: Mr. Julie Bless Parcon, RN, MAN Drug StudyДокумент2 страницыNarce Sn-Ii, Nocete Sn-Ii NCM 109-n (RLE) BSN-2A Instructor: Mr. Julie Bless Parcon, RN, MAN Drug StudyAlmera Rose NarceОценок пока нет
- Kidney Health HaemodialysisДокумент6 страницKidney Health Haemodialysishamada22xy427Оценок пока нет
- Snake Bite 1234Документ23 страницыSnake Bite 1234awais ahmedОценок пока нет
- Drug Study HemoДокумент5 страницDrug Study HemobarugacristianОценок пока нет
- Anticoagulation Pocket Cards: Adapted From The ACCP Evidence-Based Clinical Practice Guidelines 9 Edition)Документ23 страницыAnticoagulation Pocket Cards: Adapted From The ACCP Evidence-Based Clinical Practice Guidelines 9 Edition)Tricia LlorinОценок пока нет
- Diagnostic Evaluation: Clinical Severity Factor VIII Activity Bleeding TendencyДокумент2 страницыDiagnostic Evaluation: Clinical Severity Factor VIII Activity Bleeding TendencyAno NymousОценок пока нет
- FM Snake - Bite 16 12 14Документ14 страницFM Snake - Bite 16 12 14M Yandi Noer MoelamsyahОценок пока нет
- Cardio FinalsДокумент17 страницCardio FinalsNadia AbdurasidОценок пока нет
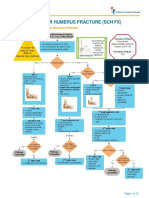
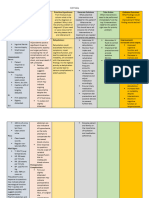
- Fracture Supracondylar HumerusДокумент12 страницFracture Supracondylar HumeruskemsОценок пока нет
- Reviewer PrelimsДокумент38 страницReviewer PrelimsKylle AlimosaОценок пока нет
- Drug Study (Tranxenamic)Документ2 страницыDrug Study (Tranxenamic)Leslie LibrandoОценок пока нет
- Ilovepdf Merged 2-69Документ1 страницаIlovepdf Merged 2-69qwivy.comОценок пока нет
- 2 Cardio Lecture PDFДокумент9 страниц2 Cardio Lecture PDFNadia AbdurasidОценок пока нет
- Criteria For Blood Donor Selection: Code: Lcbt-Coll 001Документ20 страницCriteria For Blood Donor Selection: Code: Lcbt-Coll 001Nick MasilaОценок пока нет
- Anti-NenoplasticsДокумент1 страницаAnti-NenoplasticsBaebee LouОценок пока нет
- Management of Patients Receiving Local Anaesthesia 2021Документ76 страницManagement of Patients Receiving Local Anaesthesia 2021Micheal ShawkyОценок пока нет
- Urological RefferalДокумент12 страницUrological Refferalmichelle octavianiОценок пока нет
- Snake Bite & Its ManagementДокумент29 страницSnake Bite & Its ManagementSUNIL KUMARОценок пока нет
- Anaesthetic 07Документ3 страницыAnaesthetic 07AinunОценок пока нет
- Pharmacology Hematologic SystemДокумент19 страницPharmacology Hematologic SystemCurtney PedriaОценок пока нет
- Blood Trasnfusions 1Документ7 страницBlood Trasnfusions 1Silvia RodríguezОценок пока нет
- EpistaxisДокумент2 страницыEpistaxisnurseОценок пока нет
- Snake Bite Management: DR - Padmesh .V, Dept of Pediatrics, DR - SMCSI MCH, KarakonamДокумент31 страницаSnake Bite Management: DR - Padmesh .V, Dept of Pediatrics, DR - SMCSI MCH, KarakonamTheo TОценок пока нет
- What Is TriagingДокумент5 страницWhat Is TriagingshairaОценок пока нет
- Drug NorvascДокумент1 страницаDrug NorvascSrkocherОценок пока нет
- Activity 6 - Drug StudyДокумент14 страницActivity 6 - Drug StudyAl-Mujib TanogОценок пока нет
- Cognitive Aids SupplementДокумент13 страницCognitive Aids SupplementKe YuheОценок пока нет
- Medication - ALT-Template - Enoxaparin SodiumДокумент1 страницаMedication - ALT-Template - Enoxaparin SodiumNancyAmissahОценок пока нет
- Drug Study orДокумент6 страницDrug Study orAlliah MayoОценок пока нет
- Sirosis Hepatis Dan KomplikasiДокумент36 страницSirosis Hepatis Dan KomplikasiMuhammad HafizdОценок пока нет
- Dental MedicineДокумент59 страницDental Medicinechh56k6tndОценок пока нет
- Treatment Protocol of SnakebiteДокумент23 страницыTreatment Protocol of SnakebiteEduconsultОценок пока нет
- Drug LovenoxДокумент2 страницыDrug LovenoxSrkocherОценок пока нет
- B. Caso Clinico. Turchin, I., & Barankin, B. 2006. Dermacase. Chronic Venous Insufficiency.Документ3 страницыB. Caso Clinico. Turchin, I., & Barankin, B. 2006. Dermacase. Chronic Venous Insufficiency.Alex Andrés Cuevas UrriolaОценок пока нет
- Vascular Surgery: Summary of A Subspecialty !Документ102 страницыVascular Surgery: Summary of A Subspecialty !Dr-Mohammad Ali-Fayiz Al TamimiОценок пока нет
- Selmar Maribojo JR, MD First Year Medical ResidentДокумент52 страницыSelmar Maribojo JR, MD First Year Medical ResidentSelmar Quimpo Maribojo Jr.Оценок пока нет
- Generic Name: Brand Name: Route: Frequency: Before:: AE: HemorrhageДокумент2 страницыGeneric Name: Brand Name: Route: Frequency: Before:: AE: HemorrhageKim SunooОценок пока нет
- Bleeding DisordersДокумент26 страницBleeding DisordersChelleyOllitroОценок пока нет
- Vitamin K (Phytonadione)Документ1 страницаVitamin K (Phytonadione)E75% (4)
- CardizemДокумент1 страницаCardizemSheri490100% (1)
- CASE STUDY PPT Group1 - Revised WithoutvideoДокумент34 страницыCASE STUDY PPT Group1 - Revised WithoutvideoSamantha BolanteОценок пока нет
- LovenoxДокумент1 страницаLovenoxAdrianne BazoОценок пока нет
- Post Operative ComplicationsДокумент11 страницPost Operative ComplicationsIlyas HarunОценок пока нет
- Case Study #7Документ22 страницыCase Study #7Christian Dave EndinoОценок пока нет
- Deep Vein Thrombosis (DVT) : DisclaimerДокумент9 страницDeep Vein Thrombosis (DVT) : DisclaimerKaka FebriantoОценок пока нет
- Blood TransfusionДокумент7 страницBlood TransfusionSamantha Orozco PinedaОценок пока нет
- Drugs That Affect The Hematological SystemДокумент4 страницыDrugs That Affect The Hematological Systemoxidalaj100% (2)
- Pingen, Kathleen Joy R. BSN 3AДокумент3 страницыPingen, Kathleen Joy R. BSN 3AKathleen Joy PingenОценок пока нет
- Pressure Immobilisation Snake BiteДокумент12 страницPressure Immobilisation Snake BiteSony Yanuar NugrohoОценок пока нет
- 3rd Year - READINGSДокумент48 страниц3rd Year - READINGSBryelleОценок пока нет
- Autonomic Dysreflexia BlueДокумент20 страницAutonomic Dysreflexia BlueanjelikaОценок пока нет
- CJSS 11Документ3 страницыCJSS 11j5khdwgywwОценок пока нет
- Priapism (Painful Erection), A Simple Guide To The Condition, Treatment And Related ConditionsОт EverandPriapism (Painful Erection), A Simple Guide To The Condition, Treatment And Related ConditionsОценок пока нет
- Orthopedic Inpatient Protocols: A Guide to Orthopedic Inpatient RoundingОт EverandOrthopedic Inpatient Protocols: A Guide to Orthopedic Inpatient RoundingОценок пока нет
- Treatment of Hemophilia A and B PDFДокумент268 страницTreatment of Hemophilia A and B PDFYusry SuryawiraОценок пока нет
- Chapter 30Документ16 страницChapter 30Ba LitОценок пока нет
- Bailey CH 7 81-120Документ82 страницыBailey CH 7 81-120melaniaОценок пока нет
- Acquired Factor VIII Inhibitors: Pathophysiology and TreatmentДокумент6 страницAcquired Factor VIII Inhibitors: Pathophysiology and TreatmentSakinah Mar'ie SanadОценок пока нет
- Diabetes InsipidusДокумент60 страницDiabetes Insipidusperie_md100% (1)
- Diabetes InsipidusДокумент7 страницDiabetes Insipiduspaul_stefenson10Оценок пока нет
- GRP4 - Ppt-Diabetes InsipidusДокумент12 страницGRP4 - Ppt-Diabetes InsipidusNicole Villanueva, BSN - Level 3A100% (2)
- Treatment of Orthostatic and Postprandial Hypotension - UpToDateДокумент25 страницTreatment of Orthostatic and Postprandial Hypotension - UpToDateCipriano Di MauroОценок пока нет
- (A) (B) (C) (D) : (A) Primary Polydipsia Is Not The Answer Here Because in Primary PolydipsiaДокумент1 страница(A) (B) (C) (D) : (A) Primary Polydipsia Is Not The Answer Here Because in Primary PolydipsiaAbdul QuyyumОценок пока нет
- GuiademedicamentosДокумент59 страницGuiademedicamentospaolarestauroОценок пока нет
- Nocturnal Enuresis:: Current ConceptsДокумент9 страницNocturnal Enuresis:: Current Conceptsdstu20Оценок пока нет
- DesmopresinДокумент9 страницDesmopresinNARESH JANDIALОценок пока нет
- Treatment of Orthostatic and Postprandial HypotensionДокумент13 страницTreatment of Orthostatic and Postprandial HypotensionRebeca RiveraОценок пока нет
- Diabetes InsipidusДокумент17 страницDiabetes InsipidusSan Siddz100% (2)
- Fludrocortisone (Florinef)Документ15 страницFludrocortisone (Florinef)passer by100% (1)
- Pediatric Diabetes InsipidusДокумент11 страницPediatric Diabetes InsipidusVictor Matias BarriosОценок пока нет
- Hematologic DisordersДокумент32 страницыHematologic DisordersQuolette ConstanteОценок пока нет
- 1 Pituitary and Thyroid PharmacologyДокумент64 страницы1 Pituitary and Thyroid PharmacologyZaina MasriОценок пока нет
- Antidiuretic HormoneДокумент1 страницаAntidiuretic HormoneFalaq2Оценок пока нет
- Diurnal Enuresis Case Study Group 2Документ108 страницDiurnal Enuresis Case Study Group 2JUDE ARIZALAОценок пока нет
- Jurnal LUTS PDFДокумент8 страницJurnal LUTS PDFmitaОценок пока нет
- Biology Investigatory Project On Mendelian DisordersДокумент42 страницыBiology Investigatory Project On Mendelian DisordersPrasaanth Rock86% (14)
- Haad BulletsДокумент25 страницHaad BulletsViola A. Atilano83% (6)
- Anesthesia For Transsphenoidal Pituitary Surgery.Документ6 страницAnesthesia For Transsphenoidal Pituitary Surgery.ismaelОценок пока нет
- ButlerДокумент9 страницButlerHepicentar NišaОценок пока нет
- Advances in Therapeutic Peptides Targeting G Protein-Coupled ReceptorsДокумент25 страницAdvances in Therapeutic Peptides Targeting G Protein-Coupled ReceptorsAyberk BinbayОценок пока нет
- Product Catalogue: Keep Life FlowingДокумент12 страницProduct Catalogue: Keep Life FlowingTheencyclopediaОценок пока нет
- Endocrinology: Nplex Review Kimberly Sanders, NDДокумент37 страницEndocrinology: Nplex Review Kimberly Sanders, NDValeria AcevedoОценок пока нет
- HemophiliaДокумент20 страницHemophiliamuhirwa SamuelОценок пока нет
- Deficient Fluid Volume (Vanene)Документ7 страницDeficient Fluid Volume (Vanene)jajalerОценок пока нет