Вам также может понравиться
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- Secretary of State Alex Padilla's Letter To Dean LoganДокумент2 страницыSecretary of State Alex Padilla's Letter To Dean LoganKTLA 5 NewsОценок пока нет
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5795)
- Read Trump's Letter To PelosiДокумент6 страницRead Trump's Letter To Pelosikballuck194% (95)
- DMV Statement On Data BreachДокумент3 страницыDMV Statement On Data BreachKTLA 5 News100% (1)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- Night + Market Song's Drunken Noodle Pastrami Pad Kee MaoДокумент1 страницаNight + Market Song's Drunken Noodle Pastrami Pad Kee MaoKTLA 5 NewsОценок пока нет
- Nam Khao Tod, Vegan PDFДокумент2 страницыNam Khao Tod, Vegan PDFKTLA 5 NewsОценок пока нет
- Nam Khao Tod, Vegan PDFДокумент2 страницыNam Khao Tod, Vegan PDFKTLA 5 NewsОценок пока нет
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Best Neurologist in BangaloreДокумент3 страницыBest Neurologist in BangaloreAlgoTrends AlgoTrendsОценок пока нет
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- Similarities and Differences Between Theravada and Mahayana BuddhismДокумент10 страницSimilarities and Differences Between Theravada and Mahayana BuddhismANKUR BARUA89% (9)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- RRLДокумент4 страницыRRLElaine Lacandula100% (1)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (400)
- Top German AcesДокумент24 страницыTop German AcesKlaus Richter100% (1)
- Micro Analysis Report - Int1Документ3 страницыMicro Analysis Report - Int1kousikkumaarОценок пока нет
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (345)
- Cambridge IGCSE: PHYSICS 0625/63Документ16 страницCambridge IGCSE: PHYSICS 0625/63...Оценок пока нет
- FS0008 Toolangi State Forest Walking TrailsДокумент2 страницыFS0008 Toolangi State Forest Walking TrailsMichael ConosОценок пока нет
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- Redox ChemistryДокумент25 страницRedox ChemistrySantosh G PattanadОценок пока нет
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- Sales Manager Job DescriptionДокумент8 страницSales Manager Job Descriptionsalesmanagement264Оценок пока нет
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- 2003catalog PDFДокумент25 страниц2003catalog PDFPH "Pete" PetersОценок пока нет
- Short-Term Memory and Working MemoryДокумент32 страницыShort-Term Memory and Working Memorysiempreviva84Оценок пока нет
- Preface: How To Use This BookДокумент1 страницаPreface: How To Use This BookCarlos SaavedraОценок пока нет
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- "Written Statement": Tanushka Shukla B.A. LL.B. (2169)Документ3 страницы"Written Statement": Tanushka Shukla B.A. LL.B. (2169)Tanushka shuklaОценок пока нет
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- Nonviolent Communication Lessons 2-20-18Документ210 страницNonviolent Communication Lessons 2-20-18Ice George100% (1)
- LESSON PLAN IN wRITING A REPORTДокумент2 страницыLESSON PLAN IN wRITING A REPORTMarkaton Dihagnos100% (4)
- Holidays Homework 12Документ26 страницHolidays Homework 12richa agarwalОценок пока нет
- NM Rothschild & Sons (Australia) LTD. V Lepanto Consolidated Mining CompanyДокумент1 страницаNM Rothschild & Sons (Australia) LTD. V Lepanto Consolidated Mining Companygel94Оценок пока нет
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- Human Resource Management in The Hospitality Industry Is FullyДокумент14 страницHuman Resource Management in The Hospitality Industry Is FullykiahОценок пока нет
- Cambridge Assessment International Education: Information Technology 9626/13 May/June 2019Документ10 страницCambridge Assessment International Education: Information Technology 9626/13 May/June 2019katiaОценок пока нет
- Catalogue Maltep en PDFДокумент88 страницCatalogue Maltep en PDFStansilous Tatenda NyagomoОценок пока нет
- Tiktok, Identity Struggles and Mental Health Issues: How Are The Youth of Today Coping?Документ6 страницTiktok, Identity Struggles and Mental Health Issues: How Are The Youth of Today Coping?Trúc NgânОценок пока нет
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- Lord of The Flies AnalysisДокумент10 страницLord of The Flies AnalysisMuhammad AsifОценок пока нет
- G.R. No. 178511 - Supreme Court of The PhilippinesДокумент4 страницыG.R. No. 178511 - Supreme Court of The PhilippinesJackie Z. RaquelОценок пока нет
- 06 - Wreak Bodily HavokДокумент40 страниц06 - Wreak Bodily HavokJivoОценок пока нет
- BA Thesis Linguistics 4Документ102 страницыBA Thesis Linguistics 4volodymyrОценок пока нет
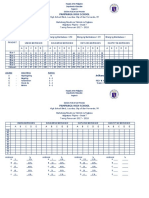
- Silent Reading With Graph1Документ2 страницыSilent Reading With Graph1JonaldSamueldaJoseОценок пока нет
- Individual Development Plans: A. Teaching Competencies (PPST) Objective 13, KRA 4 Objective 1, KRA 1Документ2 страницыIndividual Development Plans: A. Teaching Competencies (PPST) Objective 13, KRA 4 Objective 1, KRA 1Angelo VillafrancaОценок пока нет
- Intensive Care Fundamentals: František Duška Mo Al-Haddad Maurizio Cecconi EditorsДокумент278 страницIntensive Care Fundamentals: František Duška Mo Al-Haddad Maurizio Cecconi EditorsthegridfanОценок пока нет
- TS-1326 (21581) MS For Dismantling Temporary Steel Platform at Grid P-7 To P-8 & P-AC To PTI-AДокумент21 страницаTS-1326 (21581) MS For Dismantling Temporary Steel Platform at Grid P-7 To P-8 & P-AC To PTI-AJiabing ZouОценок пока нет
- Preview ISO+15613-2004Документ6 страницPreview ISO+15613-2004Brijith0% (1)