Вам также может понравиться
- Reproductive SystemДокумент32 страницыReproductive SystemEdwin OkonОценок пока нет
- Oestrogen, Progesterone, AndrogensДокумент58 страницOestrogen, Progesterone, AndrogensTandin SonamОценок пока нет
- Hormones in Reproduction: Presented To: Dr. Akhtar Rasool Presented By: M Tayyab 2012-VA-300Документ17 страницHormones in Reproduction: Presented To: Dr. Akhtar Rasool Presented By: M Tayyab 2012-VA-300javeria choudharyОценок пока нет
- Drugs Affecting Reproduction: DR - R - PrameelaДокумент76 страницDrugs Affecting Reproduction: DR - R - PrameelaRamadi PrameelaОценок пока нет
- Pharmacology: Drugs Acting On The Reproductive SystemДокумент8 страницPharmacology: Drugs Acting On The Reproductive SystemShun Reigh SumilangОценок пока нет
- SCIENCE Feedback Mechanism in Menstrual CycleДокумент6 страницSCIENCE Feedback Mechanism in Menstrual CycleJasmineОценок пока нет
- Ovarian CycleДокумент78 страницOvarian CyclefasicaregroupОценок пока нет
- Reproductive Hormones: Gonadotropin Releasing Hormone (GNRH)Документ9 страницReproductive Hormones: Gonadotropin Releasing Hormone (GNRH)Pooja RnairОценок пока нет
- Hormone of Reproductive System (Synthesis and Mechanism of Action)Документ38 страницHormone of Reproductive System (Synthesis and Mechanism of Action)pwfОценок пока нет
- Sex HarmoneДокумент22 страницыSex Harmonesuyash jainОценок пока нет
- Outline For The Quarterly Assessment in Science BiologyДокумент8 страницOutline For The Quarterly Assessment in Science BiologyeiОценок пока нет
- Reproductive Hormones and Their FunctionsДокумент6 страницReproductive Hormones and Their FunctionsOwolabi PetersОценок пока нет
- Female Hormonal System: Irfan Idris Physiology Department Hasanuddin UniversityДокумент31 страницаFemale Hormonal System: Irfan Idris Physiology Department Hasanuddin UniversityNur AnniesaОценок пока нет
- Female Sex HormonesДокумент30 страницFemale Sex HormonesMagdy El-GammalОценок пока нет
- Female HormoneДокумент43 страницыFemale Hormoneامجد حسين جواد كاظمОценок пока нет
- Lecture 2 - Reprod - HormonesДокумент5 страницLecture 2 - Reprod - Hormoneskushal NeupaneОценок пока нет
- 1,4) HPG and Physiology of AndrogensДокумент46 страниц1,4) HPG and Physiology of AndrogensBHUWAN BASKOTAОценок пока нет
- Hormon ReproДокумент36 страницHormon Reproalvinrinaldi1101Оценок пока нет
- Classification of Hormone and Their Mechanism of ActionДокумент22 страницыClassification of Hormone and Their Mechanism of ActionMUHAMMAD AWAISОценок пока нет
- PHARMA-R4.3-Gonadal Hormones - InhibitorsДокумент17 страницPHARMA-R4.3-Gonadal Hormones - Inhibitorscharmainemargaret.parreno.medОценок пока нет
- Hormonal Control of GametogenesisДокумент37 страницHormonal Control of GametogenesisZeneishaОценок пока нет
- Female HormoneДокумент24 страницыFemale HormoneZuha HundalОценок пока нет
- Gonadal Hormones & Inhibitors Contraceptives: DR Dhoro Clinical PharmacologyДокумент34 страницыGonadal Hormones & Inhibitors Contraceptives: DR Dhoro Clinical PharmacologykelvinОценок пока нет
- 10 Female Sex HormonesДокумент14 страниц10 Female Sex HormonesRana AbdullahОценок пока нет
- EndocrinologyДокумент21 страницаEndocrinologySANCHAYEETAОценок пока нет
- Female Sex HormonesДокумент28 страницFemale Sex HormonesAbdimalik AliОценок пока нет
- Male Sex Hormones FunctionsДокумент18 страницMale Sex Hormones FunctionsPermanand BheemsinОценок пока нет
- Gonadal Hormones, Their Inhibitors and Fertility and Antifertility AgentsДокумент29 страницGonadal Hormones, Their Inhibitors and Fertility and Antifertility AgentsGopal Prasad DahalОценок пока нет
- Endocrine and Reproductive Pharmacology-By:Dr. DHIREN BHOIДокумент77 страницEndocrine and Reproductive Pharmacology-By:Dr. DHIREN BHOIdrdhirenvet100% (9)
- B11.5 Hormones in Human Reproduction EdДокумент16 страницB11.5 Hormones in Human Reproduction EdBenjamin WatsonОценок пока нет
- MenopauseДокумент21 страницаMenopauseDr K AmbareeshaОценок пока нет
- Handout On ReproДокумент4 страницыHandout On ReproJoe JosephОценок пока нет
- Functions of PlacentaДокумент8 страницFunctions of PlacentappsavidalandОценок пока нет
- 01 Lecture 9 Gonadal Hormones and Drugs (Pod Pharm DR Thatcher 2022)Документ46 страниц01 Lecture 9 Gonadal Hormones and Drugs (Pod Pharm DR Thatcher 2022)sahilaminОценок пока нет
- Gynecology Review: Abigail Elsie Dg. Castro, MD, Maed, Fpogs, Fpsuog August 11, 2017Документ198 страницGynecology Review: Abigail Elsie Dg. Castro, MD, Maed, Fpogs, Fpsuog August 11, 2017Jojo Mendoza100% (1)
- Menstrual Physiology, Amenorrhea: Page 1 of 5Документ5 страницMenstrual Physiology, Amenorrhea: Page 1 of 5seth10Оценок пока нет
- Sex Hormones PDFДокумент54 страницыSex Hormones PDFmohsen mirdamadiОценок пока нет
- The Menstrual Cycle: Dr. Milvan Hadi, M. Ked (Og), SpogДокумент41 страницаThe Menstrual Cycle: Dr. Milvan Hadi, M. Ked (Og), SpogEvi Liana BahriahОценок пока нет
- Hormones of Reproductive System-G6Документ23 страницыHormones of Reproductive System-G6etheljoymabognon851Оценок пока нет
- Reproductive SystemДокумент30 страницReproductive SystemmfaizchejamriОценок пока нет
- Endocrine GlandsДокумент16 страницEndocrine GlandsAgatha BayauaОценок пока нет
- HY ObgynДокумент127 страницHY ObgynSreeja CherukuruОценок пока нет
- HY Obgyn MehlmanmedicalДокумент127 страницHY Obgyn MehlmanmedicalalmostpetergriffinОценок пока нет
- Hormone RegulationДокумент21 страницаHormone RegulationJhansi Reddy TamatamОценок пока нет
- Steroids JenniferKettelДокумент25 страницSteroids JenniferKettelvinay0717Оценок пока нет
- Puberty and The HPG AxisДокумент36 страницPuberty and The HPG AxiskjhkaОценок пока нет
- Let's Pray!Документ45 страницLet's Pray!HONLETH ROMBLONОценок пока нет
- MK Disorders of Menstruation (OBGY)Документ76 страницMK Disorders of Menstruation (OBGY)Moses Jr KazevuОценок пока нет
- Male and Female Reproductive HormonesДокумент15 страницMale and Female Reproductive HormonesPatricia BonganayОценок пока нет
- Reproductive HormonesДокумент43 страницыReproductive HormonesMunchkin CelinaОценок пока нет
- Reproductive EndocrinologyДокумент36 страницReproductive EndocrinologyswetaОценок пока нет
- EndocrinologyДокумент7 страницEndocrinologyVijith.V.kumarОценок пока нет
- MENSTRUATIONДокумент3 страницыMENSTRUATIONAdri SinclaireОценок пока нет
- Oxytocin, ADH Lecture For 2nd Year MBBS by DR Waeem KausarДокумент28 страницOxytocin, ADH Lecture For 2nd Year MBBS by DR Waeem KausarIMDCBiochemОценок пока нет
- Tutorial 4.5Документ4 страницыTutorial 4.5Rosa FinizioОценок пока нет
- ENGL 202C: Technical Definition or Description AssignmentДокумент6 страницENGL 202C: Technical Definition or Description AssignmentMegan MarieОценок пока нет
- ZOO-3202 - Trans 5 - FertilizationДокумент10 страницZOO-3202 - Trans 5 - FertilizationOwen RoldanОценок пока нет
- Menstrual Cycle: Prepared By: Mrs Bini P S Amuel Assistant Professor, SSRC N, VapiДокумент16 страницMenstrual Cycle: Prepared By: Mrs Bini P S Amuel Assistant Professor, SSRC N, VapiBini Don DanielОценок пока нет
- Balancing Hormones Naturally: A Woman's Guide to Hormonal Harmony: HealthОт EverandBalancing Hormones Naturally: A Woman's Guide to Hormonal Harmony: HealthОценок пока нет
- Drug StudyДокумент2 страницыDrug StudyClau MagahisОценок пока нет
- Pemenant Family PlanningДокумент6 страницPemenant Family PlanningKrini TandelОценок пока нет
- Philippine President Emphasis On The Systematic Distribution of Contraceptive in Our Country - by JBTBДокумент5 страницPhilippine President Emphasis On The Systematic Distribution of Contraceptive in Our Country - by JBTBJustine BianesОценок пока нет
- PhysiologyДокумент2 страницыPhysiologyapi-19762967Оценок пока нет
- Menstrual Hygiene Amongst The School Going Adolescent Girls in Rural AreaДокумент5 страницMenstrual Hygiene Amongst The School Going Adolescent Girls in Rural AreaMuhammad GhiffariОценок пока нет
- Continuing Professional Development Questions and Answer For FSRH Guideline Progestogen-Only Implant (February 2021)Документ2 страницыContinuing Professional Development Questions and Answer For FSRH Guideline Progestogen-Only Implant (February 2021)Sarumathy AshokОценок пока нет
- MATERNAL NURSING Commonly Used AbbreviationsДокумент4 страницыMATERNAL NURSING Commonly Used Abbreviations3amabelle arevaloОценок пока нет
- Gross Anatomy Urinary SystemДокумент43 страницыGross Anatomy Urinary SystemMay LacdaoОценок пока нет
- Intrauterine Drug Delivery SystemДокумент33 страницыIntrauterine Drug Delivery SystemAmit Belekar100% (1)
- Family Planning: Soledad Chu-Crisostomo, MD, FPOGSДокумент3 страницыFamily Planning: Soledad Chu-Crisostomo, MD, FPOGSColeen NeyraОценок пока нет
- Togas Tulandi Reproductive Endocrinology and Fertility PDFДокумент297 страницTogas Tulandi Reproductive Endocrinology and Fertility PDFjunediОценок пока нет
- Population Control: Today and TomorrowДокумент4 страницыPopulation Control: Today and Tomorrowsirius57Оценок пока нет
- Hormones and The Menstrual Cycle: Discussion GuideДокумент11 страницHormones and The Menstrual Cycle: Discussion GuideJohnryl FranciscoОценок пока нет
- Condom For Male and FemaleДокумент3 страницыCondom For Male and FemaledeliejoyceОценок пока нет
- Ulipristal Acetate - A New Emergency ContraceptiveДокумент4 страницыUlipristal Acetate - A New Emergency ContraceptiveAnonymous SDUIPeqXОценок пока нет
- Magic Condom BDДокумент3 страницыMagic Condom BDlovetoy5610% (1)
- Abortion EssayДокумент6 страницAbortion EssayAmelia PurcellОценок пока нет
- Menstrual CycleДокумент42 страницыMenstrual CycleBryan BriesОценок пока нет
- SOGC Guideline No. 292 - AUB in Pre-Menopausal WomenДокумент25 страницSOGC Guideline No. 292 - AUB in Pre-Menopausal WomendubblewalkerОценок пока нет
- Case Presentation: Hirsutism and OligomenorrheaДокумент20 страницCase Presentation: Hirsutism and Oligomenorrheadidu91Оценок пока нет
- 6.6 Hormones, Homeostasis and Reproduction: Essential Idea: Hormones Are Used When Signals Need To Be Widely DistributedДокумент37 страниц6.6 Hormones, Homeostasis and Reproduction: Essential Idea: Hormones Are Used When Signals Need To Be Widely DistributedImeeОценок пока нет
- Notes-Maternal Health NursingДокумент22 страницыNotes-Maternal Health NursingRachael Crossgrove100% (4)
- Maternal AnatomyДокумент96 страницMaternal AnatomyIbnu RahmanОценок пока нет
- Practical General Practice Ebook Guidelines For E... - (PG 219 - 224)Документ6 страницPractical General Practice Ebook Guidelines For E... - (PG 219 - 224)Sarah UddinОценок пока нет
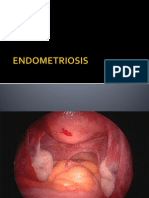
- ENDOMETRIOSISДокумент33 страницыENDOMETRIOSISSusi Indriastuti83% (6)
- Lesson 5 - Physical and Sexual SelfДокумент20 страницLesson 5 - Physical and Sexual Selfsigma rusОценок пока нет
- Progesterone Review of Safety For Clinical StudiesДокумент19 страницProgesterone Review of Safety For Clinical StudiesCatrinescu OanaОценок пока нет
- Unit Test - Unit 14Документ5 страницUnit Test - Unit 14gayathmipereraОценок пока нет
- Unwrapped - Role of CondomsДокумент9 страницUnwrapped - Role of CondomsSimranjit KaurОценок пока нет
- Coitus InterruptusДокумент2 страницыCoitus InterruptusMaulana213Оценок пока нет